


A two-millimeter gap can turn a “good” CPAP night into a morning that feels like sandpaper and sunburned lid margins.
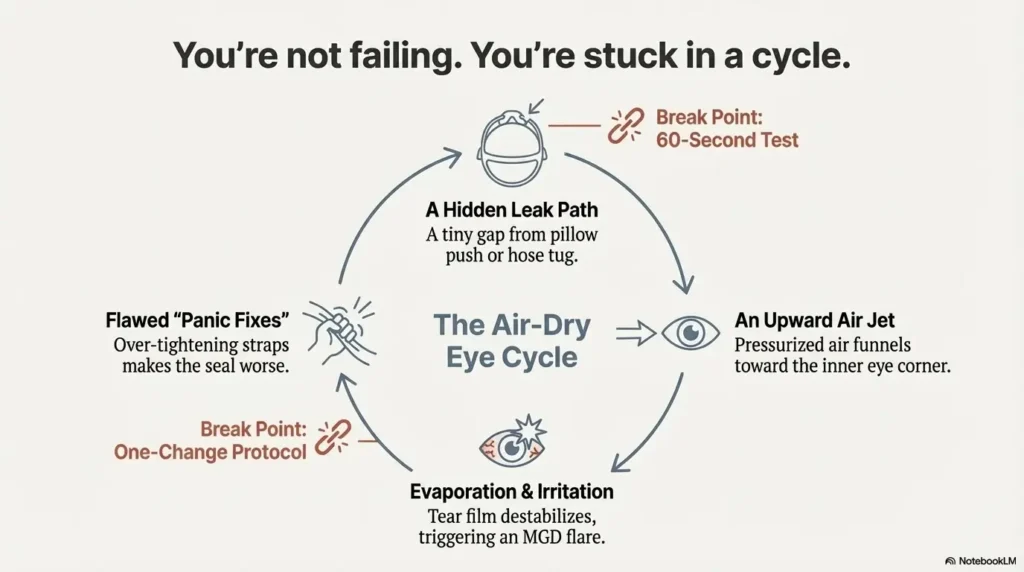
When a CPAP mask leak into eyes collides with MGD/blepharitis, the discomfort isn’t mysterious—it’s mechanical: a tiny overnight wind machine aimed at the most delicate surface you have. MGD (meibomian gland dysfunction) is when the oil glands along your eyelids don’t coat tears well, so the tear film evaporates fast. Add pressurized airflow near the inner eye corner, and that evaporation spike can snowball into a flare.
Keep guessing and you’ll pay for it twice: irritated eyes in the morning, and a higher chance you abandon therapy when you need it most.
I’m not guessing from theory—I learned this by chasing “leaks” broadly until one simple leak-path test finally made the problem solvable.
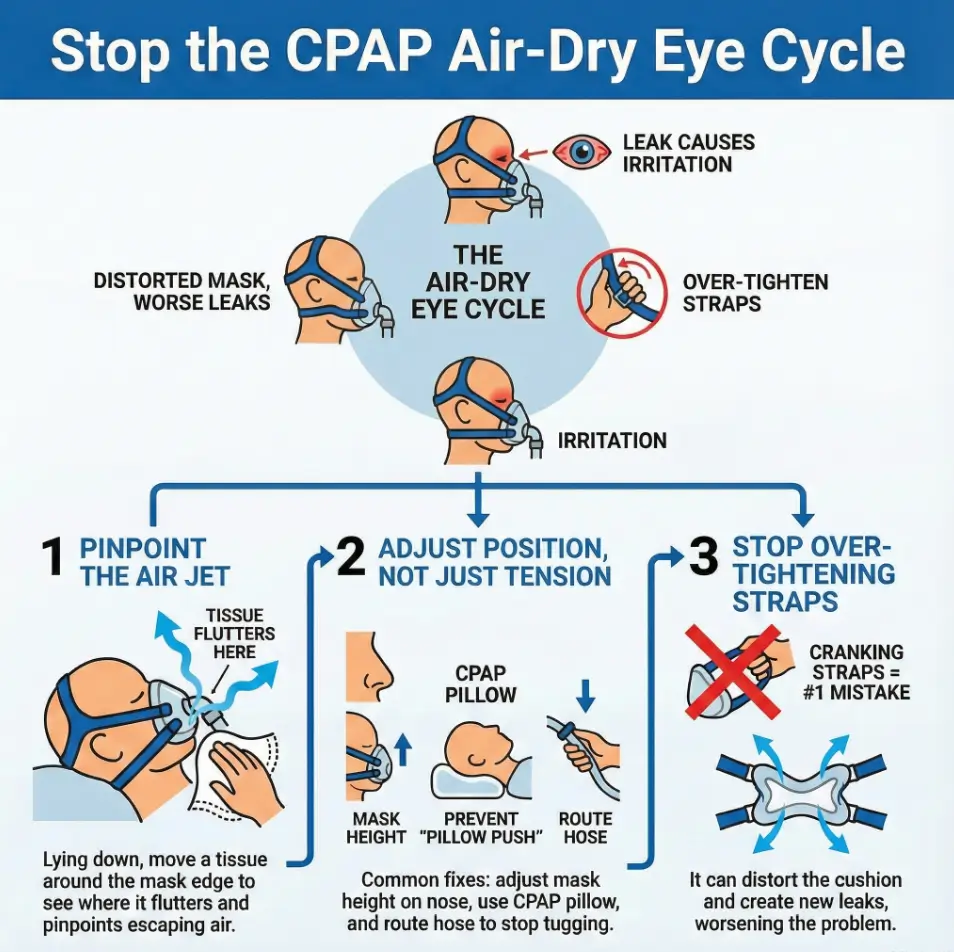
Here’s the part nobody tells you. It’s not “a leak.” It’s a direction.
Name the path first. Then change one thing—on purpose.
Safety note: This is educational, not medical advice. Don’t block mask vents or put adhesives/creams near your eyes unless a clinician specifically approves. Seek care promptly for severe eye pain, light sensitivity, thick discharge, or vision changes.
Table of Contents
- Locate the exact air escape route first.
- Refit while lying down, then stabilize hose + pillow.
- Adjust one variable per night so you can trust your result.
Apply in 60 seconds: Do the tissue test around your mask and name the leak location out loud.
CPAP eye leak, first: a 60-second “leak-path” test
If you only take one thing from this article, take this: every fix gets easier once you know where the air is escaping. My first month on CPAP, I treated “leak” like a single problem. It isn’t. It’s a location problem—bridge, cheek, top edge, hose tug, pillow push—and each location has a different fix.
Tissue drift map (bridge / cheek / top-of-mask)
Grab a tissue (or a thin strip of toilet paper). With your CPAP running, bring the tissue close—without touching your eyes—and move it around the mask perimeter:
- Bridge-of-nose / inner corner of the eye: tissue flutters upward toward your eye = classic “eye leak” route.
- Cheek edge: flutter low and sideways = cushion edge or strap balance issue.
- Top-of-mask: flutter above the cushion = frame angle or pillow push.
Operator move: test it lying down. Sitting up can hide the leak that appears at 2:17 a.m. when gravity and your pillow get involved.
Finger-sweep seal check (spot the micro-gap)
With clean hands, gently sweep a finger along the cushion edge while the machine is on. You’re not pressing hard—you’re hunting for a tiny hiss. If you feel a little “puff” near the inner eye corner, you’ve found your villain.
My own giveaway was embarrassingly small: a gap that only appeared when I relaxed my jaw. Not when I “tested” with my heroic, tense, wide-awake face.
Phone-light reveal (catch tilt you can’t feel)
Turn on your phone flashlight and angle it along the mask edge. In a dim room, micro-gaps show up as a faint line of light. This is especially helpful for nasal masks where the bridge area is the problem.
Let’s be honest… if you can’t name the leak path, you’ll keep buying “solutions” blindly
There’s a special kind of tired that makes you do irrational shopping at 6:30 a.m. after waking with angry eyes. I’ve been there. The leak-path test turns that impulse into a plan.
Show me the nerdy details
Leak “feel” is often misleading because you sense airflow where it lands, not where it starts. A small gap near the bridge can channel air upward along the mask frame and into the inner eye corner. Testing while lying down simulates the exact geometry your pillow and gravity create at night.
Money Block — Eligibility checklist: Is your eye irritation likely leak-driven?
- Yes/No: Do you feel air near the inner corner of one or both eyes?
- Yes/No: Are symptoms worse on side-sleep nights?
- Yes/No: Do symptoms improve when you reseat the mask during the night?
- Yes/No: Do you see higher leak flags (or “large leak”) on your CPAP report?
- Yes/No: Is the irritation worse in the morning than in the evening?
Next step: If you answered “Yes” to 2+ items, run the 60-second leak-path test tonight and fix the exact route (not everything at once).
MGD flare, explained: why CPAP air turns into a “dry-eye accelerator”
MGD (meibomian gland dysfunction) is the “oil layer” problem—those glands along your eyelid margins help slow evaporation. When CPAP air leaks into your eyes, it doesn’t just feel annoying. It can push your tear film toward evaporation overdrive. That’s why a leak that seems minor can create a flare that feels major.
Evaporation spike + tear film instability (the core MGD problem)
Think of your eyes like a soup that needs a lid. MGD is when the lid is thin or patchy, so the soup evaporates faster. Add a stream of pressurized air? The lid struggles. Your eyes wake up feeling like they spent the night in front of a car vent.
Why more drops can fail if airflow exposure stays nightly
Drops can help, but they’re not a force field. If the leak keeps landing on your eyes, you may be pouring water into a bucket with a fan pointed at it. I learned this the hard way: I kept “treating dryness” and ignoring the leak path, then wondered why the cycle returned every morning.
If you’re experimenting with drops, many people prefer gentler options like preservative-free eye drops for seniors—but even the “right” drop can’t outwork a nightly air jet aimed at your inner eye corner.
The clue most people miss: “better at noon” isn’t the same as “healed”
MGD flares often calm later in the day. Your body compensates. You blink. You hydrate. You stop getting blasted by air. But if the leak returns at night, you reset the problem nightly.
Open loop: the one bedtime detail that predicts tomorrow’s flare
It’s not your willpower. It’s geometry: side-sleep + pillow pressure + hose tug. When those three line up, your mask can behave all night like it’s “almost sealed”—which is the most irritating kind of leak because it’s continuous.
Eye-leak causes, decoded: vents vs leaks vs pillow push
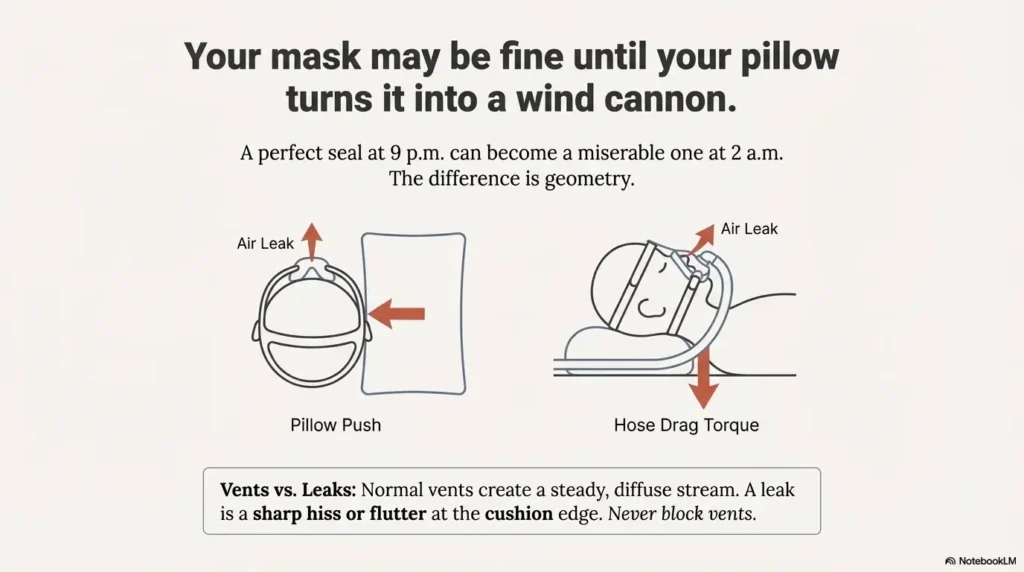
This section matters for safety. Every CPAP mask has intentional venting. Those vents prevent you from rebreathing exhaled air. A real leak is different—and mixing them up can lead to bad choices (like trying to block vents). Let’s separate the three biggest “air feels weird near my eyes” causes.
Normal vent flow (what it should feel like) vs true leak (what it feels like)
| What you’re feeling | Likely cause | What to do |
|---|---|---|
| Steady stream from a specific vent area | Normal venting | Leave it alone; don’t cover vents |
| Hiss + flutter at cushion edge near eye corner | Seal leak | Refit lying down; adjust tension balance |
| Leak appears only on side, disappears on back | Pillow push / hose torque | Change pillow setup + hose routing |
Side-sleeper “pillow push” that breaks the seal by millimeters
If you side-sleep, your pillow can press the mask frame just enough to create an upward gap. It’s subtle. It’s also the most common “my eyes are dying but my mask seems fine” story I hear.
My “aha” moment: I woke, reseated the mask, and the eye blast stopped instantly. That’s not “dry eye out of nowhere.” That’s an airflow problem with a bedtime trigger.
Hose drag torque: the invisible tug that aims air upward
Hose tug is sneaky because it’s not constant. You roll, the hose catches, the mask tilts, and suddenly the inner eye corner gets the worst of it. The fix often isn’t a new mask—it’s hose management.
Here’s what no one tells you… your mask may be “fine” until your pillow turns it into a wind cannon
You can have a perfect seal at 9:00 p.m. and a miserable seal at 2:00 a.m. The pillow is the difference. Which is annoying, because pillows are innocent and fluffy and should not have opinions about your therapy.
Leaky mask into eyes: the bridge-of-nose height fix (the sneaky one)
This is the curiosity loop from the introduction: the “one small thing” that kept sabotaging me. I wore the mask slightly too high because it felt stable. Stable, yes. Sealed? No. That tiny height mistake funneled air straight toward my eye corner.
Refit lying down (seal where you actually sleep)
- Lie in your normal sleep position.
- Turn the machine on (use mask fit mode if you have it).
- Hold the mask gently to your face, then tighten straps just until it stays in place.
- Run the tissue drift test again near the eyes.
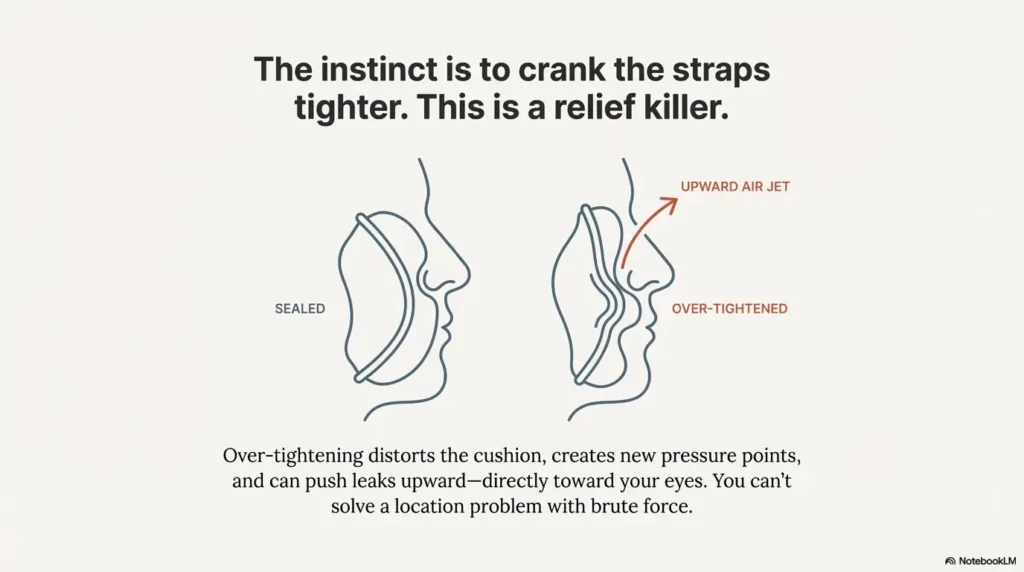
Micro-lesson: Your goal is “stable contact,” not “crank-tight.” Over-tightening can distort the cushion and create the gap you’re trying to fix.
Micro-adjust order: cushion → frame → straps (not the reverse)
- Cushion: make sure it’s seated evenly on the frame (no tiny twists).
- Frame angle: adjust the mask position so the cushion sits naturally, not forced.
- Straps: tighten in small, even steps (left/right balance matters).
What to watch for: “inner eye corner puff”
If you feel a little jet near the inner eye corner, treat it as a location-specific leak, not a global “my mask is bad” verdict. This is where re-positioning by a few millimeters can be more effective than buying something new.
7 fixes, ranked: stop CPAP air blowing into your eyes tonight
Below is the sequence that finally worked for me—and for most time-poor CPAP users who can’t spend three weeks “experimenting.” Run them in order. If you jump around, you’ll end up with a different setup every night and zero confidence in what helped.
Fix 1 — Size audit (why “medium” lies across brands)
Mask sizing isn’t universal. A “medium” from one manufacturer can fit like a “small-ish medium” from another. If you’re between sizes, eye leaks often show up first because that inner corner area is unforgiving.
- Check the manufacturer sizing guide for your exact model.
- If you’re using a DME, ask for a re-fit—most have fit templates.
Personal note: I resisted this because it felt like admitting defeat. The right size felt like cheating. In a good way.
Fix 2 — Strap tension reset (“snug + stable,” not “tight + painful”)
Over-tight straps can flatten or buckle the cushion. You want the cushion to inflate slightly and “float” into a seal.
- Loosen everything, reseat the mask, then tighten evenly.
- Stop as soon as leaks improve—don’t chase “zero sensation.”
Fix 3 — Cushion care (residue + slip-gaps)
Skin oils and leftover soap can make the cushion slide. Sliding becomes micro-leaks. Micro-leaks become eye jets.
- Clean with mild soap and water (avoid harsh cleaners).
- Rinse well. Dry fully.
- If it’s tacky or warped, it may be time to replace the cushion.
Fix 4 — Hose routing & lift (remove nightly tug)
Route your hose so it moves with you, not against you. A simple hose lift (or even a clip to the headboard) can remove the “mask tilt” that aims air upward.
- Give the hose slack where you turn.
- Keep it above pillow level if possible.
I used to wake up and find the hose wrapped like a rebellious scarf. The night I clipped it above my head, my leak pattern changed immediately.
Fix 5 — Pillow strategy (CPAP pillow / edge-sleep setup)
If your pillow presses the mask frame, try:
- A CPAP pillow with side cutouts, or
- Sleeping closer to the edge of the pillow so the mask “hangs” off slightly.
It looks silly. It feels less silly than stinging eyes.
Fix 6 — Humidity + heated tube tuning (comfort without rainout)
Humidity doesn’t “fix” an eye leak, but it can reduce overall dryness stress while you fix the leak mechanics. Heated tubing can help prevent condensation when humidity is higher.
Fix 7 — Mask-style pivot (when nasal pillows/full face actually helps)
Sometimes the fix is switching interface style—especially if your face shape and sleeping position keep defeating the same seal area. Nasal pillows can reduce contact points near the eyes for some people, while a well-fitted full-face mask can reduce mouth leak for others. The right choice depends on where your leak path lives.
- Size and position first.
- Stability second (hose + pillow).
- Humidity last (comfort support, not a seal fix).
Apply in 60 seconds: Refit lying down and stop tightening the moment the eye puff disappears.
Don’t do this: 6 “relief killers” that worsen leaks + MGD
Some mistakes are obvious in daylight and irresistible at midnight. This list is here so you don’t learn them the way I did—half-awake, bargaining with your pillow like it’s a therapist.
Mistake 1 — Cranking straps tighter (creates new gaps + pressure points)
If you have to keep tightening, the fit is wrong. Tight straps often distort the cushion and push leaks upward—right toward the eyes.
Mistake 2 — Blocking vents (unsafe, reduces therapy effectiveness)
Vents are intentional. Covering them can be dangerous. If airflow near your face is bothering you, treat it as a fit or positioning problem—not a “block the holes” problem.
Mistake 3 — Changing 5 variables at once (you can’t tell what worked)
New cushion + new humidity + new pillow + new strap tension = chaos. Change one thing, test two nights, then move on.
Mistake 4 — Ignoring cushion wear schedule (small warps become air jets)
Cushions soften over time. If your leak suddenly worsened with no other changes, wear is a prime suspect.
Mistake 5 — Treating dryness only (and leaving the leak untouched)
This is the “I’ll just use more drops” trap. If air is still hitting your eyes, you’re managing symptoms and feeding the cycle.
Mistake 6 — “Quitting early” during the adjustment window (compliance cliff)
In the US, many insurers and programs track CPAP use early on. If you stop using therapy because of comfort problems, you can end up with both worse sleep and a harder path to coverage support. The goal is not perfection—it’s consistent use while you troubleshoot.
- Don’t tighten blindly.
- Don’t block vents.
- Don’t change everything at once.
Apply in 60 seconds: Pick exactly one fix to test tonight and write it down.
Humidity for eye comfort: how to adjust without creating rainout
Humidity is the comfort dial people love to hate. Too low and you wake up dry. Too high and you get “rainout” (condensation) and a wet mask that feels like sleeping in a tiny aquarium. The trick is stepping slowly and using a heated hose when needed.
Start-point strategy (moderate setting, gradual changes)
Start in the middle of your machine’s range and move by one step every 2 nights. If you jump from low to max, you won’t know whether improvement came from humidity or from a random good seal night.
Signs humidity is too low (dry mouth/throat/nasal irritation)
- Dry nose or stuffy nose in the morning
- Dry mouth (especially if you mouth-breathe)
- Sore throat or frequent waking to sip water
Important: humidity can ease comfort, but it won’t stop a direct air jet into your eye. Treat humidity as support, not the main fix.
Heated hose advantage (reduces condensation and stabilizes comfort)
Heated tubing can keep warm, moist air from cooling too quickly and condensing. If you need more humidity for comfort but keep getting rainout, the heated hose is the “middle path.”
Open loop: the “one diary line” that helps clinicians fix this faster
Use a printable symptom diary for seniors and write this down for three nights: “What woke me up?” (dryness, wet mask, eye sting, pressure, noise). One sentence. That’s it. It turns vague complaints into patterns.
Show me the nerdy details
Humidity affects mucosal comfort (nose/throat) more than it affects a localized eye leak. Rainout happens when humid air cools in the tube, condenses, and pools. Heated tubing reduces that temperature drop, which is why it can allow higher humidity without the “wet mask” problem.
Money Block — Mini calculator: What is this “morning eye tax” costing you?
This isn’t medical. It’s motivation. If eye irritation steals time each morning, quantify it so you treat this like the solvable problem it is.
Estimated time lost: —
Next step: Choose one leak-path fix to test tonight so your mornings stop paying this tax.
Who this is for / not for (so you don’t self-manage the wrong thing)
Because this topic touches both sleep therapy and eye health, it helps to be clear about who can safely troubleshoot at home—and who should escalate quickly.
This is for you if…
- You wake with burning, gritty eyes or eyelid margin irritation after using CPAP.
- You can identify a likely leak path (bridge area, cushion edge, pillow push, hose tug).
- Symptoms are annoying, but you don’t have severe pain, light sensitivity, thick discharge, or vision changes.
This is not for you if…
- You have sudden vision changes, severe pain, or marked light sensitivity.
- You have thick discharge or suspect infection, corneal irritation, or a significant allergic reaction.
- Your clinician has given you a specific mask/setting plan due to complex medical factors.
Personal note: I delayed talking to an eye doctor because I thought “it’s just dryness.” When I finally went, the biggest benefit wasn’t a miracle drop. It was clarity—what was safe to experiment with, and what wasn’t.
If you’re debating whether what you’re feeling is “just getting older” or something that deserves faster evaluation, keep this bookmarked: is it just getting older, or a serious eye disease?
When to seek help: sleep clinician vs eye doctor (and what to bring)
Here’s the calm, practical split: your sleep clinician helps with pressure, leaks, mask fit, and adherence. Your eye clinician helps with eye-surface injury risk, blepharitis/MGD management, and ruling out problems that shouldn’t wait.
Urgent eye care triggers (pain, photophobia, discharge, vision change)
- Severe eye pain (not just “dry” discomfort)
- New or worsening light sensitivity
- Thick discharge, crusting that’s new, or signs of infection
- Blurred vision that doesn’t clear quickly after waking
Sleep team triggers (persistently high leak, intolerable pressure, poor sleep)
- Leak remains high after you try the ranked fixes
- You remove the mask during sleep without realizing it
- Pressure feels intolerable or you’re waking frequently
Bring these 3 items: symptom timeline, mask model/size, leak observations
Money Block — Quote-prep list (what to gather before your call)
- Mask model + size + how old the cushion is
- Humidity setting + whether you use a heated hose
- Two nights of notes: sleep position + when eyes felt worst
- If you have it: a leak report screenshot or the “large leak” flag count
Next step: Put these in your phone notes before you call—your appointment gets 3x more efficient.
The fastest path to a useful appointment: the one-minute script
Try: “I’m using CPAP consistently, but I’m waking with eye irritation that tracks with air leaking toward the inner eye corner. I tested the leak path while lying down. I’ve tried refitting and hose routing. Can we review leak rate, mask fit options, and a comfort plan while I protect my eyes?”
If you want a practical baseline for routine eye follow-up (especially if you’re in the “this keeps happening” camp), this helps: how often seniors should get dilated eye exams. And if you like checklists before appointments, keep this nearby: annual eye exam checklist for seniors.
Show me the nerdy details
Clinicians troubleshoot faster when the problem is stated as a measurable pattern: leak location + sleep position + what changes you’ve already tested. It reduces guesswork and helps differentiate fit issues from settings issues.
Buy vs skip (US): the no-regret gear list for eye leaks + MGD-prone lids
This is not a shopping spree. This is a “stop paying for random hope” section. If you’re short on time and want the highest-likelihood tools, start here.
Worth it: CPAP pillow, hose lift/clip, replacement cushions
- CPAP pillow: if pillow push is your leak trigger, this can be the easiest win.
- Hose lift/clip: reduces mask tilt and keeps the seal stable.
- Fresh cushion: if yours is worn/soft/warped, replacement can be night-and-day.
Maybe: mask liner (only if it doesn’t interfere with seal/vents)
Some people love liners for comfort. If you use one, verify it doesn’t shift the seal or cover venting. Comfort is great—unsafe airflow changes are not.
Skip: anything that blocks vents or puts irritants near eyes
If a “hack” involves covering vents, taping near the eyes, or adding sticky products around the eyelids, treat it as a red flag unless your clinician has explicitly cleared it.
Money Block — Decision card: When to change gear vs when to fix technique
| If this is true… | Do this first | Only then consider |
|---|---|---|
| Leak appears only on side-sleep nights | Pillow setup + hose routing | CPAP pillow or hose lift |
| Leak path is inner eye corner/bridge | Refit lying down + height/angle correction | Different cushion size or mask style |
| Mask suddenly leaks after months of stability | Cushion cleaning + inspect wear | New cushion or headgear |
Next step: Pick the row that matches you and test that “Do this first” step for two nights.
FAQ
Why does my CPAP mask leak into my eyes only when I sleep on my side?
Side sleeping often adds pillow pressure that nudges the mask frame and breaks the seal by millimeters. That small shift can funnel air upward toward the inner corner of the eye. Hose tug is the other common culprit—when you roll, the hose can tilt the mask.
Can CPAP air worsen dry eye or MGD?
It can, especially if air leaks toward the eyes. MGD involves tear film instability, and airflow can increase evaporation. The goal is to reduce direct exposure by fixing the leak path and supporting comfort (humidity, heated tube, eyelid hygiene as advised by your clinician).
How do I stop leaks without tightening the straps?
Start with a lying-down refit, correct the mask height/angle, and balance strap tension evenly. Then stabilize the setup with hose routing and a pillow strategy. Tightening should be the last move—and only in tiny, symmetrical steps.
Is a full-face mask better for preventing eye leaks?
Sometimes, but not automatically. If your leak path is at the bridge area, a different full-face design might help—or it might add more surface area to leak. Choose based on your leak location and breathing pattern (mouth vs nose) rather than assuming one style is “best.”
How can I tell vent flow from a true leak?
Vents produce a consistent stream from a specific vent area and are normal. A true leak often feels like a hiss at the cushion edge and changes with position (especially side sleeping). Never block vents.
What humidity setting helps dry eyes with CPAP?
There isn’t one universal “best” setting. Start moderate and adjust slowly, one step every couple of nights. If you get condensation (rainout), a heated hose can help. Remember: humidity supports comfort; it doesn’t replace fixing an eye-directed leak.
How often should I replace my mask cushion to reduce leaks?
Replacement timing varies by model, wear, and supplier policies. If your cushion is soft, warped, or suddenly slipping despite cleaning, it’s reasonable to suspect wear. If you’re unsure, ask your DME or sleep clinic what replacement cadence applies to your specific setup.
Can mask liners interfere with therapy?
They can if they change the seal or cover venting. If you try one, re-run the leak-path test while lying down and confirm your vents are unobstructed.
When should I see an eye doctor for CPAP-related irritation?
Seek care promptly for severe pain, marked light sensitivity, thick discharge, or vision changes. If symptoms are persistent or worsening despite fixing the leak path, an eye clinician can help protect the ocular surface and manage blepharitis/MGD safely.
Next step: tonight’s 10-minute “one-change” protocol
If you’re tired and busy (and honestly, who isn’t), here’s the plan that keeps you from spiraling. It’s built to protect therapy consistency while you fix comfort. And yes, it’s designed for the version of you who will be half-asleep later.
Do the 60-second leak-path test, then apply one fix (not five)
- Run the tissue drift test around the bridge and inner eye corner.
- Name the leak path: “bridge,” “cheek,” “top edge,” “pillow push,” or “hose tug.”
- Pick one fix from the ranked list that matches that path.
Mark strap positions + hose route (so tomorrow isn’t a reset)
Use a tiny piece of tape on the strap (not on your skin) or a marker dot on the strap itself to remember your “good” setting. For the hose, pick a consistent route (above headboard, clip, or slack loop).
The “two-night rule”: what to track before changing anything else
- Did your eyes sting in the morning? (0–10)
- Did you feel air near the eyes at any point?
- Did you side-sleep most of the night?
- One change at a time.
- Two nights per change.
- Track a simple score so you don’t rely on memory.
Apply in 60 seconds: Write “Leak path: ____” in your phone notes before you turn out the light.
Short Story: The night I stopped “fixing everything” (120–180 words) …
I had one of those weeks where sleep feels like a rumor. I’d wake up, eyes burning, and spend the morning like a distracted raccoon—rubbing, blinking, squinting at screens, googling in a fog. One night I snapped and tried to fix everything at once: tighter straps, different pillow, higher humidity, different cushion, different hose route. It felt productive. It also made the next morning impossible to interpret. Was it better? Worse? I had no idea.
The next night I did something boring: I ran the tissue test, found the leak at the inner eye corner, and changed only the mask height while lying down. That was it. The next morning my eyes weren’t perfect, but they were calmer—like the inflammation dial had been turned down from an 8 to a 4. It was the first time I felt like the problem was solvable.
And if your mornings include a lot of screen squinting (hello, late-night research), it can help to recognize the overlap with digital eye strain in seniors—because discomfort stacks when you’re tired.
Conclusion: break the air-dry eye cycle in 15 minutes
Here’s the honest ending: this isn’t about having the “best” mask. It’s about stopping a specific airflow route that’s punishing your eyes. Once you locate the leak path, the fixes stop being random. And once the leak stops landing on your eyelids, MGD flares often become easier to manage—because you’re no longer re-triggering evaporation every night.
Use this tonight: identify your leak path, apply one fix, and track a simple morning score.
Your 15-minute next step: Tonight, lie down with CPAP running, run the tissue drift test around the inner eye corner, correct mask height/angle, and clip the hose to remove tug. If you do only those three, you’ve already broken the loop’s strongest link.
Last reviewed: 2025-12.