

AREDS2: Evidence-Based Risk Management for Your Vision
A single detail decides whether an “eye vitamin” purchase is smart—or just expensive: AREDS2 was built to lower progression risk, not to make vision feel better next week. If you have intermediate AMD, the loudest marketing claims (“restore,” “reverse,” “miracle”) are exactly the wrong measuring stick.
The clean, evidence-aligned definition: AREDS2 is a specific supplement formula (including lutein + zeaxanthin plus antioxidants and minerals) studied in higher-risk AMD to reduce the chance of progressing to advanced AMD over time. It’s risk management—quiet, unglamorous, and meaningful when it matches your stage.
The pain is modern and familiar: ten bottles, one anxious checkout, and a label that “sounds official” while hiding deal-breaking details like beta-carotene (a real issue for current/former smokers). Keep guessing, and you can waste months on the wrong formula—or delay the habits that actually protect your future vision. If smoking history is part of your story, use a dedicated guide for AREDS2 choices for current and former smokers before you buy anything that “looks official.”
This guide provides a calm, clear path to:
- • Match AMD stage to the only outcome AREDS2 was designed to affect.
- • Decode “AREDS2” labels and spot look-alikes fast.
- • Know what the study proved, what it didn’t, and when to call the clinic.
One step at a time. No hype. Just a decision you can defend.
Table of Contents
Safety / Disclaimer (read first)
Educational only. I can help you understand evidence and decisions, but I’m not diagnosing you or replacing your eye clinician.
- Don’t self-label “intermediate AMD.” The benefit of AREDS2 depends on stage and eye findings (your clinician’s notes matter).
- Supplements can interact with medications and health conditions. The U.S. FDA specifically advises people to talk to a health professional before using dietary supplements, especially when mixing with medicines.
- If you smoke or used to smoke: avoid formulas with beta-carotene. The National Eye Institute (NIH) explains that current and former smokers should use AREDS2 and avoid beta-carotene-containing AREDS formulas due to lung cancer risk signals.
My “buy nothing yet” rule: If you’re not sure what stage you have, pause the purchase and get the exact wording from your chart first. (I’ve watched people spend months on the wrong bottle because someone casually said “a little macular degeneration.” That phrase is wildly non-specific.) If you’re building your own “bring-to-the-visit” checklist, you may also like this annual eye-exam checklist for seniors to keep the appointment focused and useful.
Start here: what “work” actually means in intermediate AMD
“Work” = lower progression risk, not sharper vision
When people say, “Do lutein and zeaxanthin work?” they often mean: Will I see better next week? That’s a completely understandable hope—and also not what AREDS2 was built to prove.
In intermediate AMD, “work” means something less cinematic but more important: lowering the odds of progressing to advanced AMD over time. It’s risk management. Not a cure. Not a reset button. Not a new pair of eyeballs delivered by courier.
The outcome AREDS2 measured (and what it didn’t measure)
AREDS2 focused on whether a specific supplement formula changed the rate of progression to advanced (late) AMD in higher-risk people. It did not set out to prove “better day-to-day vision,” “no more blurry mornings,” or “I can read tiny menus again.” If your expectations are framed like symptom relief, you’ll feel disappointed even if the supplement is doing its real job quietly in the background.
The quiet truth: supplements are a risk-reduction tool, not treatment
Think of AREDS2 like a seatbelt. A seatbelt doesn’t prevent every accident. It doesn’t make your car faster. It also doesn’t feel like much—until the day it matters.
Anecdote #1: I once heard a caregiver describe supplement bottles as “hope you can hold.” That’s tender—and it’s also why marketing gets loud. Today we’re giving your hope a sturdier handle: what the evidence actually says you can reasonably expect.
- Expect slower progression risk, not a cure.
- Match the decision to your AMD stage.
- Judge success by consistency, not vibes.
Apply in 60 seconds: Write this on a sticky note: “AREDS2 = progression risk.” Put it where you store the bottle.
What AREDS2 actually proved (plain English, no hype)
The core benefit: progression-risk reduction in the right group
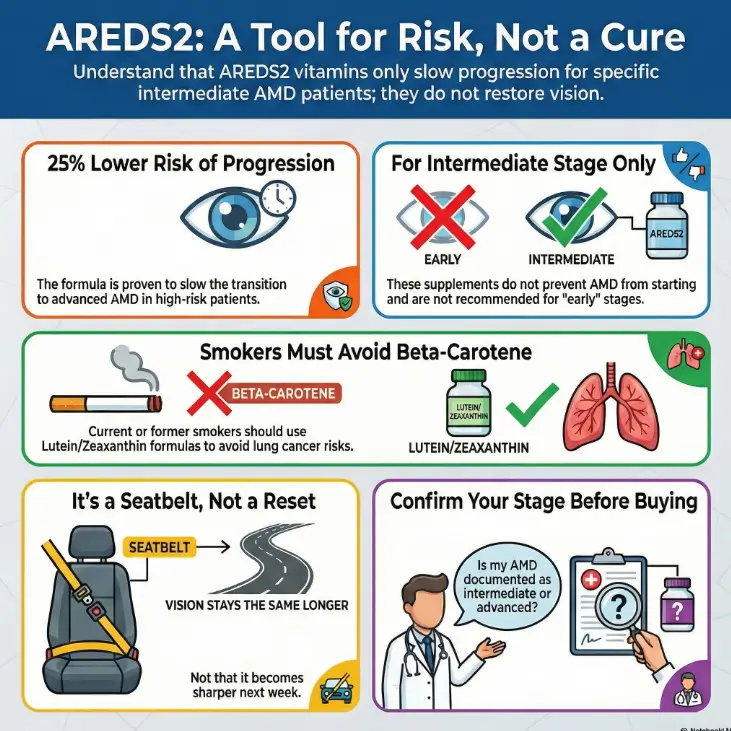
The National Eye Institute (part of the NIH) summarizes the big point clearly: for people with intermediate AMD (and certain high-risk situations, like advanced AMD in one eye), taking the AREDS/AREDS2 supplement formula reduces the risk of progression to advanced AMD. The NEI’s public explanation commonly describes this as about a 25% reduction in progression risk in the studied group.
What it did not prove: prevention, cure, vision restoration
AREDS2 did not show that these supplements prevent AMD from starting. It did not show that they “reverse” AMD. And it didn’t promise that your vision becomes crisp again just because the label looks official.
If someone tells you, “It cures dry AMD,” that’s not optimism—that’s misinformation wearing a confident hat.
Curiosity gap: why people swear it “helped” anyway (and why that’s complicated)
So why do you hear stories like: “I started lutein and suddenly my eyes felt better”? A few possibilities can be true at once:
- Regression to the mean: symptoms fluctuate; a good week happens after a bad one.
- Behavior bundling: starting a supplement often triggers better habits (lighting, sunglasses, diet).
- Dry eye overlap: “blur” isn’t always AMD progression; sometimes it’s tear film issues—especially if you notice end-of-day discomfort like
3 p.m. burning eyes.
Show me the nerdy details
AREDS2 was designed as a large randomized clinical trial and later followed in long-term observational follow-ups. The endpoint people care about here is progression to late/advanced AMD. That’s why it’s possible for a supplement to “work” statistically while you feel no daily change—because the measured outcome is about risk over time, not immediate acuity or comfort. In other words: the trial is playing chess, not TikTok.
Anecdote #2: I’ve watched people do an emotional audit in the pharmacy aisle: “This bottle costs less than my anxiety.” Fair. But the better question is, “Does this bottle match the studied formula for my stage?” That’s how you pay for help instead of paying for hope.
Short Story: The parking-lot decision (120–180 words) …
Short Story: I once met a reader who kept her AREDS2 bottle in the car for three days. Not because she forgot—because she couldn’t decide what it “meant.” Her dad had intermediate AMD, and she’d watched him go from casual jokes about “old eyes” to quiet fear in the span of a year. The bottle felt like a promise she didn’t want to break.
On the third day, she sat in a grocery store parking lot, turned the label over, and realized something oddly calming: the label didn’t say “restore vision.” It said “support.” She bought it, but she also wrote down three questions for the next clinic visit: “What stage exactly?” “Is this the right formula for his smoking history?” “What should we watch for between visits?” The bottle stopped being a talisman and became a tool.
Lutein + zeaxanthin: the part everyone talks about—what’s true?
The headline nuance: “no extra benefit” vs “better swap” (how both can be accurate)
This is where the internet gets messy. You’ll see two headlines that sound like they’re fighting:
- “Adding lutein + zeaxanthin didn’t add extra benefit.”
- “Lutein + zeaxanthin is better than beta-carotene.”
Both ideas can coexist because they’re answering slightly different questions. In AREDS2, lutein + zeaxanthin served as an effective replacement for beta-carotene—especially important for safety—and long-term follow-up analyses have supported that lutein/zeaxanthin is a sensible substitute, including in people with a smoking history where beta-carotene is a concern.
Why L/Z replaced beta-carotene (safety + signal)
The NEI’s public guidance highlights a major safety point: current and former smokers should avoid beta-carotene because of lung cancer risk signals seen in related research and follow-up findings. AREDS2 shifted the formula away from beta-carotene and toward lutein + zeaxanthin to keep the protective intent while improving the risk profile for many people.
Curiosity gap: if L/Z is “macular pigment,” why doesn’t everyone benefit equally?
Because bodies are annoying like that. Absorption varies. Diet varies. Genetics and baseline nutrient status vary. And the trial’s outcome isn’t “How yellow is your macula pigment?” It’s “Do you progress to late AMD at a different rate?” The answer can be meaningful at a population level and still feel subtle at the individual level.
Anecdote #3: A friend once told me, “I can’t tell if it’s doing anything, which makes me want to stop.” That feeling is the enemy of every prevention strategy ever invented. If you only keep what gives immediate feedback, you’ll accidentally fire the things that protect you quietly.
Who this is for / not for
Likely “for”: intermediate AMD, or advanced AMD in one eye (higher-risk category)
AREDS2 is primarily aimed at people in higher-risk categories—most commonly intermediate AMD in one or both eyes, or those with advanced AMD in one eye who want to reduce risk to the other eye. This is the “right neighborhood” where the evidence has meaning.
Likely “not for”: no AMD, early/minimal findings, or “just in case” shoppers
If you have no AMD—or early changes only—AREDS2 is not a universal “everyone should take this” move. The NEI’s public explanations emphasize that AREDS/AREDS2 supplements do not prevent AMD onset. If your goal is prevention, the better levers are often lifestyle and risk-factor management (smoking, blood pressure, diet patterns, UV/blue-light exposure management where appropriate), guided by your clinician.
The decision hinge: your stage, not your supplement optimism
This is the most expensive mistake I see: making the decision based on fear instead of stage. Stage is boring. Stage is also the only thing that makes the bottle make sense.
- Intermediate AMD: usually “yes, discuss and likely use.”
- No/early AMD: often “no, not for prevention.”
- Unsure stage: “pause purchase, confirm chart wording.”
Apply in 60 seconds: Message your clinic portal: “Can you tell me the exact AMD stage documented in my chart?”
Eligibility checklist (yes/no) — “Is AREDS2 even my lane?”
- Yes — My clinician documented intermediate AMD (or advanced AMD in one eye).
- Yes — I can take high-dose supplements safely given my meds/conditions (confirmed or planned discussion).
- Yes — If I smoke or used to, I’m avoiding beta-carotene formulas (see the beta-carotene warning for smokers/former smokers).
- No / Not sure — My stage is unclear, or I’m buying “just in case.”
Next step: If you checked any “Not sure,” don’t guess—confirm stage and formula with your eye clinician.
Formula decoding: what “AREDS2” means on a label (and what to ignore)
Must-have: “AREDS2” + ingredient match (avoid look-alikes)
“AREDS2” should mean the label matches the studied pattern: a specific combination of antioxidants + minerals, including lutein + zeaxanthin, with copper included because high-dose zinc can affect copper balance. Brands love to borrow the vibe—“eye health,” “vision support,” “lutein gummies”—without matching the studied formula.
Practical rule: Don’t buy based on front-label claims. Flip it. Read ingredients. Compare to what your clinician recommends.
Beta-carotene warning: the label detail former smokers miss
This one matters enough to repeat: if you are a current or former smoker, avoid formulas that include beta-carotene. The NEI explicitly flags this in its public AREDS2 guidance, and the ophthalmology community has discussed this risk concern for years. If you’re thinking, “But I quit 20 years ago, does it still count?”—that’s exactly the type of question to take to your clinician. If you want a quick, bottle-in-hand checklist for this exact scenario, use this AREDS2 label-decoding guide for smokers and former smokers.
Omega-3 add-ons: what AREDS2 found (and why brands still sell it)
Omega-3s are important nutrients for general health, and dietary patterns rich in fish are often associated with eye-health discussions. But the NEI’s summary of AREDS2 findings notes that omega-3 supplementation did not show an added effect on AMD progression in the AREDS2 context. This is one reason you’ll see “plus omega-3” products marketed as extra—while the core evidence for progression risk is tied to the AREDS2 pattern, not bonus ingredients.
Let’s be honest—marketing is not evidence.
If a label makes you feel like you’re failing if you don’t buy it, that’s not medical guidance. That’s copywriting. (As someone who writes for a living, I say this with both respect and suspicion.)
Decision card — When A vs B
| Option | When it fits | Trade-off |
|---|---|---|
| AREDS2 formula | You have intermediate AMD (or advanced in one eye) and want evidence-based risk reduction. | Daily habit + possible GI side effects; must check interactions. |
| Lutein/zeaxanthin alone | You’re not eligible for AREDS2, or you’re targeting general nutrition (with clinician guidance). | Not the same evidence base for progression risk in intermediate AMD. |
| Food-first (plus monitoring) | You’re early/no AMD or supplement use is complicated by meds/conditions. | Adherence is the hard part; benefits are slower and less “bottled.” |
Neutral action: Choose the option that matches your stage and your ability to be consistent for 6–12 months.
What AREDS2 didn’t settle (the honest “unknowns” section)
Does it help everyone with intermediate AMD, or only certain subgroups?
AREDS2 gives strong “big picture” guidance, but real humans have details: diet patterns, genetics, other eye conditions, and varying baseline nutrient levels. That’s why two people can be equally “intermediate” and still experience different trajectories. This isn’t a failure of science—it’s the reality of biology.
Can diet “replace” supplements? (evidence vs real-life adherence)
In theory, you can build an eye-supportive diet rich in leafy greens and other nutrient-dense foods. In practice, adherence is the boss fight. If your week includes travel, caregiving, or just being tired, it’s hard to eat like a textbook. If you want a structured, low-friction way to start, this AREDS2 diet meal plan pairs well with the “food-first” lane—especially when you’re not yet sure you’re eligible for the high-dose formula.
Anecdote #4: I’ve seen people set a perfect “greens plan” on Sunday and then meet Wednesday like a wall. Supplements can be a consistency tool—if you’re the right stage and it’s safe for you. Food still matters, but it’s not always a reliable delivery system on chaotic weeks.
Curiosity gap: are we measuring the right thing—eyesight today vs risk years later?
It’s fair to wonder: “If I can’t feel it working, how do I stay motivated?” Here’s one approach: measure what you can control (consistency, follow-up visits, home monitoring) and let the long-term outcome be what it is—probability, not promise. If you prefer a concrete “shopping list” version of food-first, keep an AREDS2-friendly grocery list on your phone so you don’t have to reinvent willpower in the produce aisle.
- Don’t chase sensations as proof.
- Use routines and reminders, not willpower.
- Keep appointments—progression is tracked over time.
Apply in 60 seconds: Put the bottle next to something you never skip (coffee, toothbrush, meds).
Common mistakes (the money-wasting, outcome-killing list)
Mistake #1: taking AREDS2 for early AMD or prevention (low ROI)
Because AREDS2 isn’t designed as a “prevent AMD from starting” pill. The NEI explicitly states AREDS/AREDS2 do not prevent AMD onset. If you’re early/no AMD, your ROI is usually better in risk-factor management and regular eye care—starting with a schedule you’ll actually keep, like guidance on how often seniors should get dilated eye exams.
Mistake #2: buying “lutein gummies” and thinking it equals AREDS2
Lutein and zeaxanthin are part of the story—but AREDS2 is a formula. A product that contains one ingredient in a candy format is not the same as an evidence-backed progression-risk strategy. It might be fine as general nutrition for some people, but it’s not a substitute for “AREDS2-style” decision-making.
Mistake #3: ignoring the smoker/former-smoker beta-carotene issue
This is the mistake with the highest potential downside. If you have a smoking history, treat beta-carotene like a “do not casually assume” ingredient. Use AREDS2-style formulas and confirm with your clinician.
Mistake #4: expecting symptom relief (AREDS2 isn’t built for that)
If your goal is “my vision feels blurry by 3 p.m.,” that could involve lighting, contrast, dry eye, refraction changes, or other issues. AREDS2 doesn’t replace those evaluations. If you’re fighting glare at home, you may get faster day-to-day relief by improving your setup—start with glare-free under-cabinet lighting tips rather than expecting a supplement to solve contrast problems.
Mini calculator — What will this habit actually cost me?
This isn’t about being cheap. It’s about staying consistent.
Estimated cost: —
Neutral action: If the yearly cost makes you flinch, talk with your clinician about the best evidence-based option you can sustain.
Anecdote #5: The most common failure mode I see is not “wrong science.” It’s “right science, abandoned in month two.” A calculator like this makes the habit feel less mysterious—and therefore easier to keep.
“Do I need lutein/zeaxanthin alone?” (why the combo matters)
AREDS2 is a formula, not a single hero ingredient
It’s tempting to pick one “star” nutrient and build a whole plan around it. But AREDS2 is deliberately a blend. The design isn’t “maximize macular pigment at all costs.” It’s “combine antioxidants and minerals in a way that changed progression outcomes in a studied group.” That’s why the formula matters more than any single buzzword.
If you only change one thing: choose the evidence-based formulation
If your clinician has confirmed you’re in the stage group that benefits, the simplest high-leverage move is: use an AREDS2-matching formula and stick with it. If you’re not in that group—or if high-dose supplements are complicated for you—then the decision shifts to nutrition, monitoring, and eye-care follow-through.
Here’s what no one tells you—“more lutein” isn’t the same as “right outcome.”
You can “optimize” a number on a label and still miss the actual target. The target is progression risk, in the right population, with a safe formula.
- Lutein/zeaxanthin alone ≠ AREDS2.
- Front labels are not contracts.
- Consistency beats “perfect” ingredients.
Apply in 60 seconds: Take a photo of your bottle’s Supplement Facts panel and bring it to your next visit.
When to seek help (don’t wait on vitamins)
New distortion, wavy lines, central blur, or sudden vision change → urgent eye evaluation
If you notice new distortion (straight lines look wavy), a sudden central blur, a dark spot, or rapid changes in one eye, don’t “wait and see if vitamins fix it.” That’s a “call the eye clinic” moment. Advanced AMD changes can be time-sensitive. If you’re trying to understand the “dry vs wet” difference behind that urgency, this dry vs wet AMD explainer can help you frame the symptoms without spiraling.
One-eye changes can hide until they don’t (simple home monitoring habits)
Because your brain is a generous editor. If one eye is slipping, the other eye often covers quietly—until it can’t. A simple habit is checking each eye separately during a routine moment (morning coffee, bedtime). If you use an Amsler grid or a similar tool recommended by your clinician, follow their instructions.
If you’re unsure of your AMD stage: ask for the exact wording in your chart
This is not being difficult. This is being competent with your own health information.
Anecdote #6: I once watched someone say, “I don’t want to bother the clinic.” And then they spent six months bothering themselves with 2 a.m. Google spirals. Clinics are for questions. Your brain is for living.
Next step (one concrete action)
Bring this 30-second script to your next eye visit
If you do nothing else, do this: bring a single, calm question set that forces clarity.
Quote-prep list — what to gather before comparing options
- Your exact chart wording: early vs intermediate vs advanced AMD.
- Whether you have advanced AMD in one eye.
- Your smoking history (current/former/never) for the beta-carotene decision.
- A list of your medications and major conditions (for interaction/safety screening).
- A photo of your current supplement label (if you already bought something).
Neutral action: Bring this list to the appointment so your decision is based on facts, not aisle confusion.
Ask: “Is my AMD intermediate (or advanced in one eye)? If yes, do you recommend AREDS2—and should I avoid beta-carotene based on my smoking history?”
FAQ
1) Do lutein and zeaxanthin work for intermediate AMD?
In the context that matters—progression risk—lutein and zeaxanthin are part of the AREDS2 formula used for people with intermediate AMD or similar higher-risk situations. The evidence base is strongest for the full AREDS2 formulation in the right stage group, not for lutein/zeaxanthin alone as a standalone “cure.”
2) What exactly did AREDS2 prove for dry AMD progression?
AREDS2 supports that a specific supplement formula can reduce the risk of progressing to advanced AMD in the studied, higher-risk groups (commonly described in public summaries as about a quarter reduction in progression risk). It did not prove prevention of AMD onset or vision restoration.
3) Can AREDS2 improve vision, or just slow worsening?
AREDS2 is best understood as a risk-reduction tool. Some people may report subjective changes, but the trial’s purpose and strongest evidence center on slowing progression risk—not reliably improving day-to-day acuity.
4) Should former smokers avoid beta-carotene in eye vitamins?
Yes—this is a key safety nuance. Public guidance from the National Eye Institute highlights that current and former smokers should use AREDS2 and avoid beta-carotene-containing formulas because of lung cancer risk signals associated with beta-carotene in this context. If you want a quick reference that’s built around this one risk hinge, see AREDS2 for smokers and former smokers.
5) Is it okay to take AREDS2 if I only have early AMD?
Often, AREDS2 is not positioned as a universal “early AMD prevention” supplement. The strongest evidence-based use is for intermediate AMD or higher-risk scenarios. If you’re early/no AMD, discuss whether the better focus is monitoring and lifestyle risk reduction instead.
6) Is omega-3 part of the AREDS2 benefit?
Omega-3s can be part of a healthy diet, but the NEI’s public AREDS2 summary indicates omega-3 supplementation did not provide an added AMD progression benefit in the AREDS2 trial framework. If you’re considering omega-3 for other health reasons, discuss dosing and interactions with your clinician.
7) How long does it take for AREDS2 to “work”?
Think in months to years, not days. AREDS2 is about changing probabilities over time. If you need a practical timeline: commit to a 90-day consistency trial for the habit itself (tolerability, routine), while your clinician tracks the eye findings over regular follow-ups.
8) What are common AREDS2 side effects or interactions to ask about?
People commonly ask about stomach upset, nausea, and interactions with medications or conditions. Because supplements can interact with medicines, it’s smart to review your medication list with a pharmacist or clinician—especially if you take blood thinners or have complex medical conditions.
Conclusion
Remember the hook question—“Is this worth it?” Here’s the clean answer: for the right people, AREDS2 is worth considering because it lowers progression risk. But it’s not a cure, not prevention, and not a guarantee of better vision next Tuesday. The “worth it” comes from matching stage + matching formula + staying consistent.
One final practical nudge: if you can do only one thing in the next 15 minutes, do this—open your patient portal (or call the clinic) and ask for your exact AMD stage. That single sentence turns a confusing supplement aisle into a decision you can defend. If your next step includes “how do I function better right now,” a low-vision consult can be life-changing— and you can start by learning what a low-vision specialist does for macular degeneration.
Last reviewed: 2026-01-22