
Monofocal vs Multifocal vs Toric IOL: Which Cataract Lens Is Best for Seniors? – 7 Shocking Lessons from My Mom’s Cataract Surgery at 74
It Felt Like Car Shopping—Except Way More Stressful.
The morning we had to pick my mom’s cataract lens, a nurse handed us a glossy, high-end brochure that honestly looked like it belonged at a Lexus dealership. Monofocal. Multifocal. Toric. Optional laser upgrade. Financing available. All we were missing was a sales guy offering us leather seats and a sunroof.
We had about 15 minutes to make a decision that could either be “fully covered and fine” or “sharper vision with fewer glasses—but also several thousand dollars out of pocket.” No pressure, right?
This guide is here to make that whole process way less overwhelming. I’ll walk you through what each lens option actually means for day-to-day life—like whether your mom can still knit, read her favorite recipes, or recognize your face without squinting.
We’ll talk money (including how Medicare fits in), break down some sneaky upsells, and I’ll share how we almost ended up spending an extra $4,000 just because we didn’t know what to ask. Think of this as your calm, clear-headed battle plan.
Table of Contents
My mom’s 74-year-old eyes and the lens decision nobody explained
My mom’s cataract story did not start in the operating room. It started in the parking lot, with her squinting at the curb and saying, “I can’t tell if that’s the sidewalk or a shadow.”
By the time she finally saw the cataract surgeon, her “gray fog” was bad enough that night driving felt like a video game on hard mode. The surgeon was kind and competent, but the lens conversation went like this:
- “Monofocal is covered.”
- “Multifocal makes you less dependent on glasses.”
- “Toric is for astigmatism.”
- “Premium lenses cost more; we’ll show you the payment plan.”
That was it. No real explanation of how they’d change her day: reading pill bottles, walking down stairs, watching grandkids play soccer under harsh stadium lights.
So we did what most families do: panicked, opened Google in the waiting room, and tried to decode a decade of eye-surgery jargon in 10 minutes.
- Most seniors can safely choose between several lens types.
- The best lens depends on lifestyle, eye health, and budget.
- You’ll make a better choice if you walk in with a simple framework.
Apply in 60 seconds: Write down your top 3 visual priorities (e.g., night driving, reading, computer) before the consult.
Quick comparison: monofocal vs multifocal vs toric for seniors
Before we get deep in the weeds, here’s the big picture. Think of intraocular lenses (IOLs) as tiny, clear implants that replace the cloudy natural lens during cataract surgery. Different IOLs trade off sharpness, range of focus, side effects, and cost.
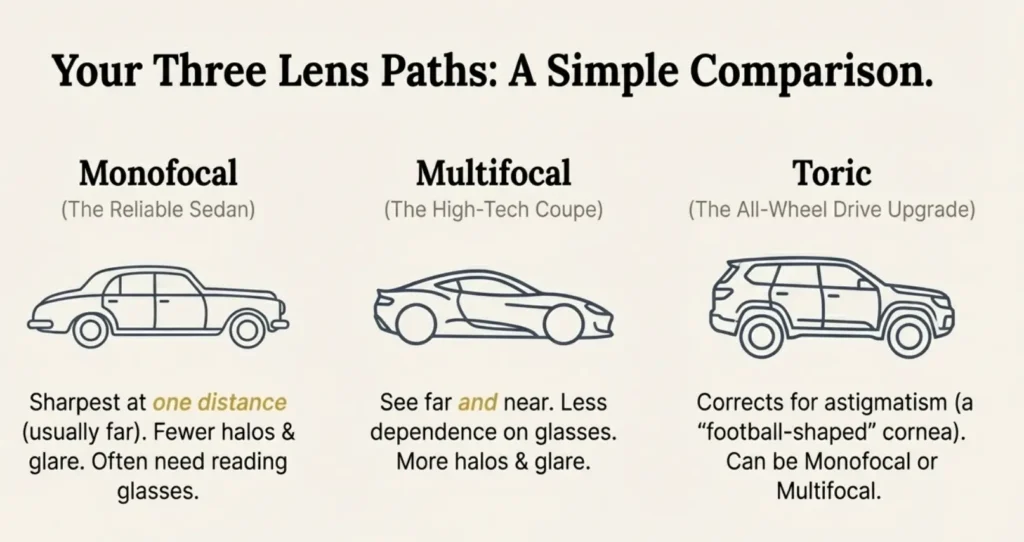
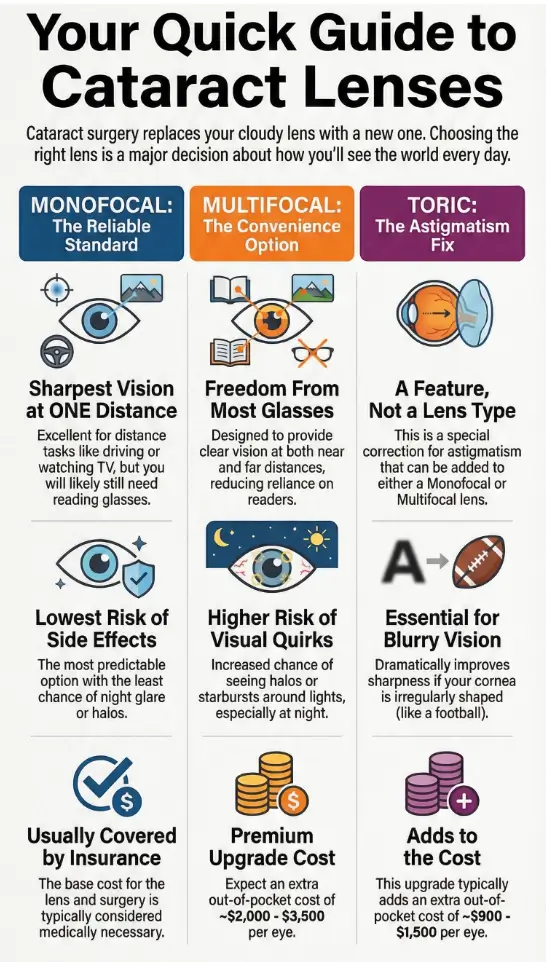
Infographic: Three Lens Paths for Seniors
Monofocal
- Sharpest at one distance (usually far).
- Most common, usually covered as “standard.”
- Often still need glasses for near tasks.
Multifocal
- Multiple focal zones for far and near.
- Less dependence on readers.
- More halos, glare, and adaptation time.
Toric
- Specially shaped for astigmatism.
- Sharper vision if cornea is “football-shaped.”
- Can be monofocal or multifocal.
Simple rule of thumb: monofocal = simplest/cheapest; multifocal = more freedom from glasses; toric = better if the cornea has moderate astigmatism.
For my mom, that “football-shaped cornea” line turned out to be crucial. She had enough astigmatism that skipping a toric option meant sharpness would always be limited, no matter how fancy the lens brochure looked.
Monofocal IOLs: the “standard” lens that’s still a workhorse
If cataract lenses were cars, the monofocal would be the reliable sedan that actually starts in winter. A monofocal IOL is designed to give you the clearest vision at one primary distance—usually far (driving, TV, walking around).
Most seniors who choose monofocal lenses still wear glasses for reading or computer work. That sounds like a downside, but here’s the quiet upside: monofocal lenses generally have fewer halos, less glare, and more predictable night vision than many multifocal designs.
With my mom, the surgeon’s first recommendation was “basic monofocal, set for distance.” She would still need cheap readers from the pharmacy, but distance vision for walking, driving, and stairs would be crisp and simple.
- Great fit if: night driving matters, you’re okay with readers, and budget is tight.
- Less ideal if: you hate wearing glasses or do a ton of reading and close work without them.
“I don’t mind glasses, I just don’t want to be scared of headlights anymore,” my mom said. That one sentence pushed us strongly toward a monofocal or toric-monofocal lens.
- Best for seniors who prioritize distance clarity and night safety.
- Low risk of visual side effects compared with many multifocals.
- Adding a toric version can significantly boost sharpness if astigmatism is present.
Apply in 60 seconds: Ask: “If we choose monofocal, what distance will you target, and will I still need glasses for the others?”
Multifocal IOLs: more freedom from readers, more visual quirks
Multifocal IOLs were designed for the person who says, “I just want to wake up, see the clock, read my phone, and not hunt for my glasses like a detective.” These lenses have different zones built into them so light focuses at multiple distances—typically far and near, sometimes intermediate.
When they work well and the eye is otherwise healthy, many people can do 70–90% of daily tasks without glasses. That’s huge. But there are trade-offs:
- Halos and glare: Those pretty rings on the lens can mean real rings around headlights, especially in the first months.
- Reduced contrast: Black text on gray backgrounds may feel a bit “washed out.”
- Personality match: Perfectionists and very night-sensitive drivers often hate the adaptation period.
My mom was tempted by multifocals—who doesn’t want fewer glasses? But once the surgeon gently asked, “How anxious do you get about night glare when you drive?”, she laughed and said, “On a scale of 1 to 10? About a 12.” That was our sign.
Show me the nerdy details
Multifocal IOLs split incoming light into multiple focal points. That’s why you can see at more than one distance—but it also means less light dedicated to each point. In practice, healthy eyes can adapt and “ignore” some of the ghost images, but any pre-existing macular disease, corneal issues, or dry eye can make halos and contrast loss feel worse. Many surgeons screen very carefully before recommending them.
Cost reality check: multifocals are usually considered “premium” IOLs, so the extra lens fee is often not covered by Medicare or standard insurance. Out-of-pocket costs of around $2,000–$3,500 per eye are typical in the US in 2025, on top of the base surgery that insurance covers.
- Fantastic for the right eyes and personalities.
- Risky if you already struggle with glare or have retinal issues.
- Think “fewer glasses,” not “zero glasses forever.”
Apply in 60 seconds: Ask your surgeon, “Would you put a multifocal in an eye like mine? Why or why not?”
Toric IOLs: when astigmatism secretly decides your lens
Toric IOLs are like monofocal or multifocal lenses that also wear a tiny invisible “contact lens” for astigmatism correction. If the front of the eye (the cornea) is more football-shaped than basketball-shaped, light doesn’t focus evenly. Toric lenses add a precise curve to counteract that.
Modern guidelines suggest considering toric lenses when corneal astigmatism is around 1.0 diopter or more, with especially strong evidence when it’s higher than about 2.0 diopters. Many recent studies show toric IOLs give more precise and stable astigmatism correction than just making extra corneal incisions or relying on glasses afterward.
For my mom, this was the real twist: she didn’t just have cataracts; she had enough astigmatism that a basic monofocal would still leave her dependent on glasses for sharp distance vision. Once we saw her measurements, the toric option suddenly went from “upsell” to “actually makes sense.”
- Monofocal toric: Clear distance vision with less astigmatism blur, usually still need readers.
- Multifocal toric: More glasses independence but with all the usual multifocal trade-offs.
Show me the nerdy details
Toric lenses must be aligned at a specific axis. Every 10 degrees of rotation error can knock out roughly a third of the astigmatism correction. Modern surgical planning tools and intraoperative alignment systems help keep that rotation low, but if a lens rotates significantly after surgery, a repositioning procedure may be needed. Your surgeon will factor this risk into the recommendation.
- Toric lenses can dramatically sharpen distance vision for the right eyes.
- They add cost but may reduce lifelong dependence on astigmatism glasses.
- The cornea’s shape, not marketing, should drive this decision.
Apply in 60 seconds: Ask, “How much corneal astigmatism do I have in each eye, and what happens if we don’t correct it with a toric lens?”
Costs, Medicare, and insurance fine print in 2025
Here’s the part that made my mom’s jaw drop.
Standard cataract surgery with a basic monofocal lens is usually considered medically necessary. In the US, Medicare and many private insurers typically cover the bulk of that “base” procedure—removing the cloudy lens and implanting a conventional monofocal IOL—leaving you with deductibles and coinsurance, often about 20% of the Medicare-approved amount.
Premium lenses (multifocal, accommodating, many toric options) are often treated as an upgrade. The extra cost of the lens technology and associated work-up is usually out-of-pocket. In practical terms, recent estimates suggest:
- Average total cataract surgery cost can run around $3,500–$7,000 per eye in the US if you had to pay it all yourself.
- Insurance/Medicare commonly covers most of that for standard monofocal surgery.
- Premium IOL upgrades (multifocal or toric) often add roughly $1,000–$3,000 per eye out-of-pocket, sometimes more in high-end centers.
If you’re outside the US, the patterns are similar but the numbers differ. For example, in countries with strong public coverage, the standard monofocal lens may be nearly fully covered, while premium multifocal or toric surcharges are paid directly by the patient or via private insurance top-ups.
In my mom’s case, the clinic handed us two numbers on a printed sheet:
- Monofocal basic: small deductible + 20% coinsurance for surgery.
- Premium toric-multifocal package: base costs covered as above, plus almost $4,000 per eye as an “elective upgrade.”
We realized we weren’t just picking a lens. We were deciding whether to buy a used car’s worth of vision upgrade—twice.
- Standard monofocal IOLs: usually covered as part of necessary surgery.
- Premium IOLs: lens surcharge is typically out-of-pocket.
- Small differences in plan and facility can change costs by thousands.
Apply in 60 seconds: Call your insurer and ask, “What do you cover for standard cataract surgery, and what parts of a premium IOL are not covered?”
Money Block 1: 60-second eligibility checklist
This quick checklist won’t replace a surgeon, but it helps you walk into the consult with a realistic range instead of a blank slate.
60-second IOL Eligibility Snapshot
- Astigmatism (from your measurements):
- 0–0.75 D → Toric lens less critical; glasses may handle it.
- ≥1.0 D → Toric lens worth discussing seriously.
- Retina and macula health:
- Known macular degeneration, diabetic retinopathy, or scarring? Multifocal might not be ideal.
- Night-driving sensitivity:
- Already bothered by glare/halos? Lean toward monofocal or monofocal toric.
- Glasses tolerance:
- Happy with readers? Monofocal (or toric monofocal) often enough.
- Hate glasses and often misplace them? Multifocal may be worth the trade-offs.
- Budget reality per eye (after insurance):
- Comfortable extra: $0–$700 → Basic monofocal with or without toric, depending on coverage.
- Comfortable extra: $1,000–$3,000 → More room for premium lenses, if medically suitable.
Next step: Mark each item “Yes/No/Unsure” and bring the list to your consult. Eligibility first, quotes second—you’ll save 20–30 minutes of confusion.
Save this: Screenshot or print this checklist and confirm all medical details with your eye doctor’s written report.
Money Block 2 & 3: Fee table + mini cost calculator
Use this section to sanity-check any quote you’re given. Numbers will vary by country, surgeon, and facility, but this gives you a realistic ballpark.
| Lens type (per eye) | Typical out-of-pocket if no insurance | Common behavior with Medicare/private insurance |
|---|---|---|
| Standard monofocal IOL + surgery | About $3,500–$7,000 | Often ~80% (or more) of base cost covered; patient pays deductible + coinsurance. |
| Toric IOL upgrade | Adds roughly $900–$1,500 to base cost | Base surgery covered; toric surcharge often out-of-pocket. |
| Multifocal IOL upgrade | Adds roughly $2,000–$3,500 to base cost | Base surgery covered; multifocal surcharge generally out-of-pocket. |
| Multifocal toric IOL | Total commonly $4,000–$6,000 per eye extra | Most of this premium portion is self-pay unless you have special coverage. |
These are broad 2023–2025 ballparks from public cost surveys and clinic disclosures; your actual figures may differ substantially.
Mini IOL Cost Calculator (rough estimate)
Use this just to get a feel for the ballpark before you talk to billing. It doesn’t store or send any data.
Save this estimate and confirm every number with your provider’s official written quote and your insurer’s benefits explanation.
How to talk to your surgeon without feeling railroaded
Surgeons are under time pressure. Clinics have billing targets. You have a human being you love sitting next to you, who just wants to see clearly again. No wonder this conversation often feels like speed-dating with a credit card on file.
Here’s the script I wish we’d had before my mom’s consult:
- “If this were your eye at 74, which lens would you choose and why?”
- “How much astigmatism do I have, and how much would a toric lens change my uncorrected vision?”
- “What problems make you hesitate to recommend multifocal lenses in patients like me?”
- “Can you show me an itemized quote that separates covered services from upgrades?”
When we finally asked those questions, the tone of the room changed. The surgeon slowed down. He drew little diagrams of my mom’s cornea. He crossed out the multifocal option himself and said, “For you, I’d do a toric monofocal in the first eye and see how you feel.”
- Ask for plain-language explanations of each option.
- Insist on separating medical necessity from convenience upgrades.
- Take notes or record (with permission) so you don’t forget details.
Apply in 60 seconds: Copy these 4 questions to your phone notes and read them out loud at the consult.
7 shocking lessons from my mom’s cataract surgery at 74
Here’s where the title of this article comes from. These are the seven points that genuinely surprised us.
- “Covered” does not mean “free.”
Medicare covered the bulk of the base surgery, but coinsurance, deductibles, pre-op tests, and post-op drops still meant hundreds of dollars out-of-pocket per eye. The premium lens quote was on top of that, not instead of it. - The “basic” lens was already life-changing.
Even with a monofocal toric, my mom went from foggy vision and fear of night driving to reading street signs again. She cried in the recovery room—not because she had a fancy lens, but because she could see my face clearly for the first time in years. - Glare and halos were not just marketing fine print.
We met another patient in the waiting room who’d had multifocals. She loved reading without glasses but was still struggling with starbursts around headlights months later. That conversation mattered more than any brochure. - Astigmatism calls a lot of the shots.
Once we saw my mom’s corneal map, it was obvious: skipping toric correction would have meant a permanent “smear” to distant objects. The toric premium suddenly looked less like a luxury and more like paying to unlock the lens she thought she was buying. - The clinic’s “default” was not our best choice.
The first quote we were handed assumed basic monofocal in both eyes. No one had explained toric vs non-toric until we asked. The moment we pushed, the surgeon agreed toric was clearly better for her measurements. - We didn’t need to decide everything at once.
Doing one eye first and waiting changed everything. After loving the toric monofocal result in the first eye, my mom felt comfortable skipping a multifocal in the second. “Give me the same thing again,” she said. - Follow-up care mattered as much as lens choice.
The surgeon’s team checked her pressure, dry eye status, and healing repeatedly. A well-managed monofocal with careful follow-up beat any hypothetical “perfect” premium lens with rushed aftercare.
Short Story: The day after my mom’s first eye surgery, she stood by the kitchen window just… staring. I asked if something was wrong. She laughed and said, “I can see individual leaves again.” Then she walked to the bathroom mirror, looked at her own face, and went quiet. “I didn’t realize how much I’d stopped looking closely,” she whispered.
For years, she’d been living in a soft-focus version of her own life—skipping nighttime events, telling herself she was just tired, letting dust and details blur together. The lens choice felt abstract when we signed the consent forms, but suddenly it was the difference between recognizing her neighbors’ faces across the street or just guessing by their walk. That was the moment I understood: this wasn’t eye surgery; it was a reset button on how she inhabited the world.
- Basic lenses can still deliver profound, emotional wins.
- Your questions can change the default recommendation.
- Healing, follow-up, and realistic expectations matter as much as tech.
Apply in 60 seconds: Pick one of these seven lessons that resonates most and build your consult questions around it.
FAQ
1. Is monofocal, multifocal, or toric “best” for most seniors?
There is no universal “best.” For many seniors, a monofocal lens (sometimes with a toric upgrade if astigmatism is moderate) gives the best mix of sharpness, safety, and affordability. Multifocals can be fantastic for carefully selected eyes that tolerate halos and don’t have retinal disease. The right choice depends on eye health, lifestyle priorities, and budget. 60-second action: Write down your top three daily activities (e.g., night driving, reading, computer) and ask which lens matches those most closely.
2. Does Medicare fully cover multifocal or toric lenses?
Medicare generally helps cover standard cataract surgery with a conventional monofocal IOL, plus one pair of glasses or contacts afterward. Premium features—like multifocal optics or many toric upgrades—are usually billed as elective extras that you pay out-of-pocket. Some supplemental or private plans may help, but you cannot assume they do. 60-second action: Call your insurer and ask specifically, “Do you cover any part of premium or toric IOL upgrades, or just the standard monofocal lens?”
3. I’m terrified of glare and halos. Should I avoid multifocal lenses?
If you already dread night driving because of glare, or you’re very sensitive to visual imperfections, it’s worth being cautious. Multifocals are more likely to cause rings around lights, especially early on. Many people adapt over time, but some never love the effect. 60-second action: Tell your surgeon honestly, “I’m extremely sensitive to glare—would you still recommend a multifocal for me?” and listen carefully to their hesitation level.
4. How long can I safely wait before deciding on cataract surgery and lens type?
Mild cataracts that barely affect daily life can often be monitored, but once your vision interferes with driving, reading, or staying safe at home, most guidelines treat surgery as reasonable and often necessary. Waiting too long can make the cataract denser and surgery slightly more complex. 60-second action: Ask your eye doctor, “If I wait 6–12 months, does that meaningfully change the difficulty or risk of surgery for me?”
5. What if I regret my lens choice after surgery?
Minor regrets are common (“I wish I’d targeted intermediate instead of distance”), but major disasters are rare when the eyes are carefully evaluated. In some cases, residual issues can be improved with glasses, laser touch-ups, or even a secondary procedure. Full lens exchanges are possible but carry extra risks and are not casual decisions. 60-second action: Before surgery, ask, “If I’m unhappy with this lens, what are our backup options?”
6. How quickly will I see clearly after surgery, and how long does recovery take?
Many seniors notice clearer vision within a day or two, though it can feel slightly hazy or “too bright” at first. Over the next few weeks, colors typically look richer and details snap into focus as the eye heals and the brain adapts. Most people resume light activities within a few days, with full stabilization over several weeks. 60-second action: Put follow-up dates and drop schedules in a calendar before surgery day so you’re not guessing afterward.
7. Is there anything special seniors outside the US should know?
If you’re in a country with public health coverage, confirm which lens types are included in the standard package and which are considered premium. Some systems fully cover monofocal IOLs but require private insurance or direct payment for multifocal or toric surcharges. 60-second action: Ask your surgeon’s office for a written quote that clearly separates what the public system pays from what counts as a voluntary upgrade.
Conclusion: your 15-minute next step
If you’ve read this far, you’re already doing more homework than most families ever get the chance to do. That alone will change how your consult goes.
Here’s a simple, realistic plan you can follow in the next 15 minutes:
- Write down your (or your parent’s) three top priorities: night driving, reading without glasses, sharp TV, computer comfort, stairs, hobbies.
- Ask the clinic for the most recent eye measurements, including astigmatism in each eye.
- Print or screenshot:
- The eligibility checklist.
- The cost table.
- The four surgeon questions from earlier.
- Decide in advance what budget range per eye you’re genuinely comfortable with for any “upgrade.”
Once you’ve done that, the conversation with the surgeon stops being “Do you want the premium lens?” and becomes “Given my eyes, my lifestyle, and my budget, which lens would you choose—and why?” That’s a very different kind of medicine.
This guide is educational and cannot replace advice from your ophthalmologist or retina specialist. Always confirm lens choices, risks, and costs with your own care team.
Last reviewed: 2025-12, based on current guidance from major eye-care organizations and public insurance resources.
Monofocal vs Multifocal vs Toric IOL, cataract lens for seniors, Medicare cataract coverage, premium IOL cost 2025, toric IOL astigmatism