


Day five is when people get “efficient”—and accidentally make their eye angrier.
A cap rolls, a bottle tip grazes a lash, drops get stacked too close together, and suddenly the grit turns into a week-long story.
If you’re using preservative-free (PF) artificial tears after cataract surgery, the confusing part isn’t picking a brand—it’s choosing a package you can keep clean while you’re tired, anxious, and juggling prescription drops. (If you’re still in the early recovery window and wondering what’s “normal,” this pairs well with cataract surgery recovery after 65 so you can sanity-check your timeline.)
Keep guessing and you risk the two problems that drag recovery out: contamination moments (tiny, repeatable) and the washout loop (tears diluting medicated drops).
PF tears are lubricating eye drops made without preservatives, often favored during healing because the surface can be extra reactive—especially when you’re dosing frequently. The tradeoff is that packaging and handling matter more.
This guide is built around the real-life failure points: hygiene, timing, dexterity, and cost-per-day—not marketing claims. Stay with me. Here’s what changes everything.
One clean routine beats one perfect product.
- Choose the safer format for your hands and environment
- Slot tears into a drop schedule without sabotaging your meds
- Calculate cost-per-day so you stop buying “hope” in boxes
Table of Contents
PF tears first: why preservative-free matters post-cataract
Post-op eyes can be dramatic. Not “you’re being dramatic”—I mean the tissues are literally in a more reactive state. A tear that felt totally fine before surgery can suddenly sting, blur, or leave you feeling like you poured lemon water into your eyeball. (Ask me how I know: I once got cocky, tried a new drop the day after a procedure, and spent 20 minutes negotiating with my reflection like it was a hostile witness.)
PF vs “gentle preservative”: the label trap that fools careful people
Preservative-free means the product is formulated without certain preservatives that can irritate some people—especially with frequent use. That doesn’t automatically mean “better for everyone,” but it can matter when your eye is healing or when you’re dosing multiple times a day. The trap is that some products sound “mild” or “sensitive,” and your brain translates that into “same thing.” It’s not the same thing.
- Preserved drops can be fine for occasional use, but frequent dosing can increase irritation for some people.
- PF drops are often chosen when you’re sensitive, using tears often, or layering multiple post-op drops.
- Packaging matters because preservatives help prevent microbial growth. Remove preservatives and you must manage contamination differently.
The healing window: why “fine before surgery” can sting now
After cataract surgery, you may have dryness from a few overlapping reasons: surface disruption, temporary inflammation, medication effects, and the simple fact that your eye is adjusting. You don’t need perfect certainty; you need a routine that reduces irritation opportunities. In practice, PF tears can be a gentler baseline while everything settles.
- Healing eyes often tolerate “simple” better than “strong.”
- Frequent dosing + preservatives can be a bad combo for some people.
- Packaging becomes part of safety when preservatives are removed.
Apply in 60 seconds: Check your bottle/vial label for “preservative-free” and decide your format before you buy a second product.
Curiosity gap: If it’s OTC, why do some surgeons still care which tears you pick?
Because “OTC” doesn’t mean “interchangeable.” Surgeons aren’t worried you’ll accidentally buy the wrong brand and explode your eyeball. They’re worried about the boring stuff that causes real misery: contamination, washout of prescription drops, and irritation that makes you rub your eye when you shouldn’t. A good surgeon cares about your behavior loop, not your shopping cart.
Vials vs bottles: the real trade—sterility vs friction
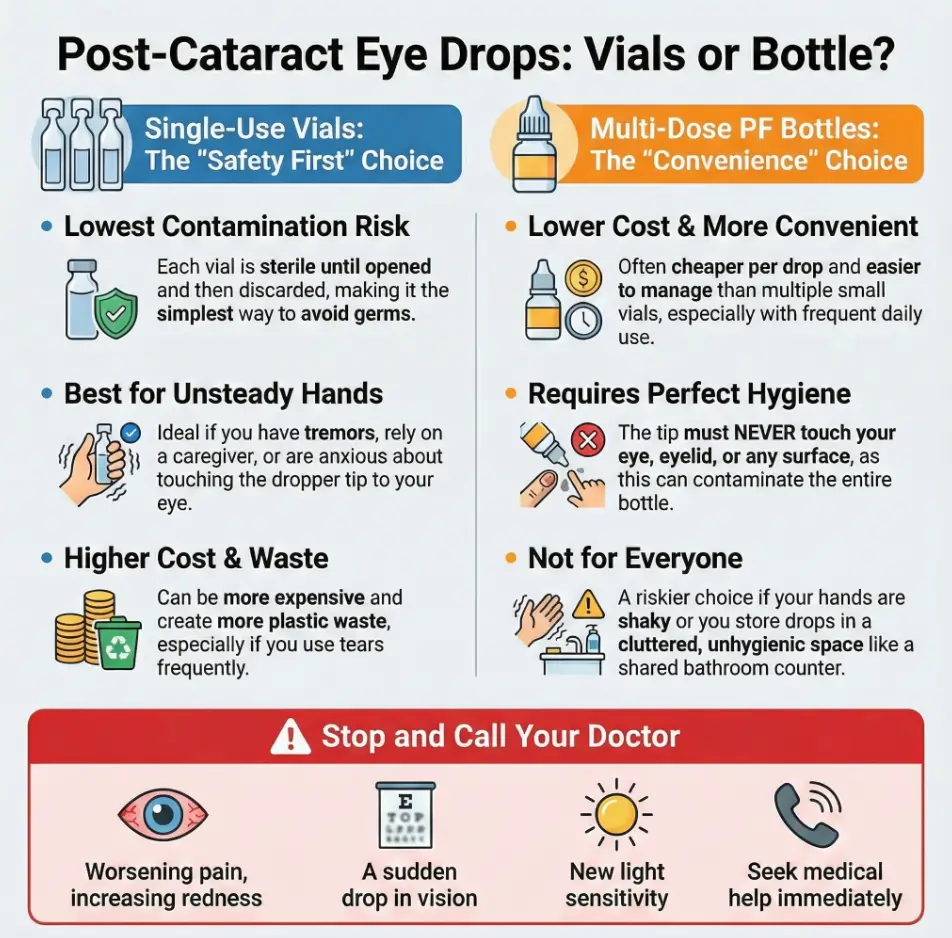
Let’s name the core decision honestly: single-use vials reduce contamination opportunities, but they add friction (opening, storing, traveling, waste, cost). PF multi-dose bottles reduce friction, but they require more discipline and rely on the bottle’s design to stay clean after opening.
Single-use vials: lowest contamination pathway (and the costs you feel later)
Vials are straightforward: open → drop → discard. Fewer steps means fewer chances to touch a tip, recap a contaminated opening, or store an opened container in a steamy bathroom. For high-anxiety moments (first week post-op, caregiver dosing, shaky hands), that simplicity is a feature.
PF multi-dose bottles: convenience—if the delivery system stays clean
Multi-dose PF systems try to solve a hard problem: deliver drops repeatedly without preservatives while minimizing contamination. If you can keep the tip from touching anything—and you store it properly—these can be a very workable solution, especially if you’re dosing often and cost matters.
Curiosity gap: Why do some PF bottles still have “discard after X days” rules?
Because “PF” removes chemical protection, so the product depends on packaging integrity and your handling. Some bottles have a recommended discard window after opening to reduce the chance that contamination (or degraded sterility) becomes an issue over time. It’s not a scare tactic; it’s risk management for real-world humans.
| Decision factor | Single-use PF vials | PF multi-dose bottles |
|---|---|---|
| Contamination risk | Lowest (one-and-done) | Low if handled perfectly; higher if tip contact happens |
| Ease for caregivers | Often easier (less tip discipline) | Requires careful no-touch technique |
| Cost per day | Often higher at frequent dosing | Often lower per drop |
| Travel/bedside | Great (grab a few; no worries) | Fine, but protect from heat + contamination |
| Waste | More packaging waste | Less packaging waste |

Single-use vials: the hygiene wins—and the two gotchas
Single-use vials feel like the “safe” answer, and often they are. But two gotchas cause most of the post-op frustration: (1) people try to reuse them, and (2) people assume the leftover liquid means they’re “supposed” to stretch it.
Don’t recap it: what “single-use” is protecting you from
Recapping creates a false sense of safety. The opening and tip can pick up microbes from fingers, countertops, or accidental contact with lashes. Even if you recap carefully, you’ve turned a one-time sterile unit into a tiny storage container in a world that is not sterile. Post-cataract is not the moment to gamble on “probably fine.”
The “extra liquid” mystery: why vials look overfilled
Many vials contain more liquid than you’ll use in a single dose. That doesn’t mean you’re meant to stretch the vial for hours. It often means manufacturing ensures you can get the intended number of drops reliably. Your job is not to extract maximum value from one vial; your job is to protect a healing eye.
Let’s be honest… your hands aren’t sterile (a quick pre-drop routine)
If you do nothing else, do this: wash hands, dry with a clean towel, and keep the vial tip away from everything—including your lashes. I tell people to imagine the vial tip is a tiny microphone that records whatever it touches. You don’t want your lashes “on the record.”
- Wash hands (20 seconds is enough when you actually do it).
- Open vial without touching the dropper tip area.
- Instill drops without tip contact.
- Discard immediately.
PF multi-dose bottles: what “safe design” actually means
PF multi-dose bottles can be a genuinely smart choice—especially if you’re dosing often and the cost is adding up. But you have to be honest about two things: your technique and your environment. In the real world, most “contamination” isn’t a dramatic event; it’s a tiny lapse that repeats.
Not all MDPF is equal: design features that reduce backflow and touch-risk
Some multi-dose PF systems are engineered to reduce contamination risk with features like valves, filters, or one-way delivery pathways. This doesn’t make them magic; it makes them less fragile in normal use. When you’re shopping, don’t just look for “PF.” Look for language that suggests the bottle is designed to keep the contents protected after opening.
Show me the nerdy details
Preservatives suppress microbial growth in many multi-use liquids. When a product is preservative-free but multi-dose, it typically relies on packaging engineering (valves/filters/air management) to reduce the chance that contaminated air or fluid travels back into the bottle. The goal isn’t “zero risk”; it’s reducing contamination pathways in repeated use.
Tip discipline: “no contact” sounds easy—until you try it
This is where people fail quietly. You think you’re not touching anything, but then your hand wobbles, you blink, your lashes exist, gravity laughs, and the tip makes a tiny kiss with your eyelid. If you’re someone with tremor, arthritis, long nails, or just post-op nerves, the bottle may not be the best early choice.
Curiosity gap: If the formula is identical, why does packaging change outcomes?
Because your eye doesn’t only respond to ingredients. It responds to irritation, contamination, and the stress loop of “why is this still uncomfortable?” Packaging changes how reliably you can deliver drops cleanly. In post-op life, reliability is comfort.
- Great option if you’re steady-handed and consistent.
- Riskier if you tend to touch tips or store bottles in chaotic places.
- Early post-op, “simple” often beats “efficient.”
Apply in 60 seconds: Be brutally honest: if you’ve ever touched a dropper tip to your eye, start with vials (at least short-term).

Contamination moments: where germs actually enter (and how to block them)
Here’s the comforting truth: you don’t need to fear everything. You need to fear three moments. Most contamination happens through contact—tip contact, cap contact, or “set it down somewhere” contact.
The lash touch, the countertop tap, the cap interior (the usual suspects)
- Lashes/eyelid contact: It happens when you’re aiming and blinking. This is the #1 offender.
- Countertop contact: Bathroom counters are… not a sterile field.
- Cap interior contact: Touching the inside of the cap or leaving it face-up can seed contamination.
Shared bathroom storage: why “family rules” matter more post-op
If you have kids, roommates, or a partner who likes to “tidy,” your drops can be moved, opened, or placed in weird spots. I once watched a well-meaning relative put someone’s eye drops right next to a toothbrush cup—like it was a cute little family photo. Your post-op eye deserves better boundaries. (If you want a practical, low-drama setup, steal the idea of a dedicated “clean zone” from this best home setup after cataract surgery guide.)
- Store drops in a consistent, clean, dry place.
- Keep caps on immediately after use.
- Don’t share eye drops (even within a household).
Mini reset: what to do if you think you touched the tip
If a bottle tip touched lashes/skin, the cautious move—especially early post-op—is to stop using that bottle and switch to a fresh container (or vials) until you talk to your surgeon. For vials, discard immediately. For multi-dose, the risk depends on the system and your surgeon’s guidance, so don’t “logic” your way into reusing it while your eye is healing.
Show me the nerdy details
Microbes don’t need a dramatic event to matter. Repeated low-level contamination plus a sensitive surface can amplify irritation and inflammation. Post-surgical eyes may be more vulnerable to complications, so risk tolerance should be lower than usual during early recovery.
Timing rules: how PF tears fit around your post-op prescription drops
This is where many people accidentally sabotage themselves. They’re doing everything “right,” but the order and spacing of drops turns into a washout loop: tears dilute prescription drops, prescription drops sting more, and then you use more tears to soothe—repeat.
The washout problem: tears too close can dilute medicated drops
If you put artificial tears in immediately before or after a prescription drop, you can reduce how much of the medication stays on the surface long enough to do its job. The exact timing your surgeon wants can vary, but a common practical approach is leaving a buffer window between different drops.
The comfort rule: why “last drop wins” can backfire
If you end with a thick gel tear, it can coat the surface and affect how other drops spread. If you start with tears, your prescription drop may feel less irritating—but it may also be diluted if you don’t wait. The goal is not “no sting.” The goal is “effective meds + stable comfort.”
Here’s what no one tells you… timing beats brand most days
Most “this drop doesn’t work” stories are actually timing stories. I’ve watched people go through three products in a week, when the real fix was simply spacing and consistency. Your eye loves boring routines.
- Don’t stack drops back-to-back without a buffer.
- Keep your routine consistent for at least 48–72 hours before judging “results.”
- When unsure, follow your surgeon’s timing instructions over internet rules.
Apply in 60 seconds: Write a simple drop schedule on paper and tape it near where you dose.
Cost per drop: which package is cheaper for your routine
If you’re dosing 1–2 times a day, the cost difference may feel small. If you’re dosing 6–10 times a day (which some people do during rough stretches), the difference can feel very real—fast. This section is the “stop guessing” moment.
4x/day vs 8x/day: the break-even point that flips the answer
At higher frequency, multi-dose bottles often win on cost-per-drop. But if you’re early post-op and you’re anxious about contamination or you have shaky hands, vials can still be the “cheaper” option if they prevent a setback. Cost isn’t just price; it’s avoidable misery.
Waste reality: when vials are “expensive” and when they’re just precise
Vials feel wasteful because you discard leftover liquid. But if that discarding prevents contamination worries (and reduces the urge to rub your eye), it’s precision—not waste. The question is: are you paying for liquid, or paying for peace?
Travel + backup: why two formats sometimes beat one
A surprisingly good setup for some people: keep a multi-dose PF bottle at home (clean, consistent storage) and carry a few single-use vials for travel or bedside. That way your messy environments don’t touch your “main” bottle.
Tip: If you’re comparing vials vs bottle, run this twice with each package’s rough drops-per-package estimate from its label or product info.
Show me the nerdy details
“Drops per package” varies with bottle design, drop size, and how hard you squeeze (seriously). For a fair comparison, use your best estimate from product labeling or manufacturer info, then sanity-check with a real-world test over 2–3 days.
Comfort mechanics: why PF tears can still burn after cataract surgery
Let’s remove the guilt right now: if PF tears burn, it doesn’t mean you did something wrong. It usually means the surface is dry, irritated, or reacting to something about the drop (viscosity, ingredients, temperature). Your job is to reduce variables, not to “tough it out.”
Watery vs gel vs ointment: blur tradeoffs and when thicker helps
Watery drops can feel refreshing but may not last long. Gel drops can last longer but blur more. Ointments can be very soothing at night but often blur significantly. Post-op, blur is emotionally spicy—because you’re already worried about vision—so choose thickness strategically (often: lighter during the day, thicker at night if your surgeon says it’s okay). If blur is impacting daily tasks, especially anything behind the wheel, pair this advice with driving after cataract surgery guidance so you’re not guessing with safety.
Temperature + surface dryness: tiny tweaks that reduce sting
If drops sting, try these low-risk tweaks: don’t store them in a hot car, avoid using them right after a fan/AC blast, and consider room-temperature dosing (extremes can feel harsher). Also: blink gently after dosing instead of squeezing your eyes shut like you’re wringing out a towel. Yes, I’ve done the towel thing. No, it didn’t help.
Switching too fast: why “testing brands” can keep you stuck
Trying three products in three days makes it hard to know what helped. If symptoms are mild, give a product and routine a consistent window (often 48–72 hours) before you declare it “bad.” If symptoms are severe, don’t “test” your way through pain—call your surgeon.
Common mistakes: 7 habits that prolong irritation post-op
This is the section that saves the most suffering per minute. These are not moral failures. They’re normal human behaviors—especially when you’re tired, anxious, and trying to juggle multiple drops like you’re working in an air-traffic tower.
Mistake #1: Tears immediately before/after medicated drops (washout loop)
If your prescription drops are part of healing and inflammation control, protect them with spacing. Stacked drops are a common reason people feel like “nothing is working.”
Mistake #2: “Just once” tip contact (then weeks of irritation stories)
One small tip touch doesn’t guarantee harm, but it increases risk—especially in the first weeks after surgery. The problem is that people rarely touch the tip once. They touch it once, then again, then again. Patterns are the enemy.
Mistake #3: Reusing single-use vials “because it’s PF”
PF doesn’t mean “safe to store open.” Single-use means single-use. Early post-op is not the time to play “but I was careful.”
Mistake #4: Using thick gels early, then blaming blur on surgery
Thicker drops can blur—sometimes a lot. If you use them right before driving or screen work, you’ll hate them and you’ll think something is wrong with your surgery. Choose thickness at the right time (often evening).
Mistake #5: Old opened bottles during the healing window
Even if you used it for months before surgery, an older bottle is not a great match for a newly healing eye. Fresh, clean, consistent wins.
Mistake #6: Storing drops in heat (car/glovebox)
Heat can degrade products and makes dosing harsher. If your drops live in your car, your eye is doing hard mode for no reason.
Mistake #7: Treating pain/redness as “just dryness”
Dryness can be uncomfortable, but worsening pain, increasing redness, discharge, or sudden vision changes deserve medical attention. Don’t normalize symptoms that are trending the wrong way. (If you’re a caregiver for an older adult, it can help to know the bigger picture of cataract surgery complications in seniors so you can spot “not just dryness” sooner.)
- Protect your prescription drops with spacing.
- Eliminate tip contact like it’s your job.
- Pick one routine and run it consistently for a few days.
Apply in 60 seconds: Choose one PF format and commit to a clean routine until your next check-in.
Choose your format: a 60-second decision tree (post-cataract edition)
Okay—decision time. Don’t overthink this. A good decision is one you can execute while sleepy, stressed, and in a bathroom with questionable lighting. Here’s the simplest way I know to choose without spiraling.
- Choose single-use vials if you: have shaky hands, rely on a caregiver, travel a lot, tend to touch tips, or feel anxious about contamination.
- Choose PF multi-dose if you: have steady hands, can store drops cleanly, dose frequently, and want lower cost per drop.
- Pause and call your surgeon if you: have worsening pain, sudden vision changes, increasing redness/discharge, or escalating light sensitivity.
Neutral next action: Pick one path and write it down—your future self will thank you.
Choose single-use vials if you…
- Need the simplest hygiene loop (open → drop → discard).
- Are early post-op and easily spooked by symptoms.
- Have dexterity issues, tremor, arthritis, long nails, or a caregiver doing drops.
- Want a “travel pack” that doesn’t contaminate your main supply.
Choose PF multi-dose if you…
- Dose often and need cost-per-day to be reasonable.
- Can reliably keep the tip from touching lashes/skin.
- Have a clean, consistent storage spot (not a chaotic bathroom counter).
- Prefer one bottle over many tiny vials.
Choose neither—call if you…
- Have pain that’s worsening instead of improving.
- Notice sudden vision decline, new flashes/floaters, or a curtain-like shadow.
- See increasing redness, discharge, or swelling.
- Feel light sensitivity that’s escalating.

When to seek help: dryness vs a post-op problem you shouldn’t wait on
Dry eye after cataract surgery is common. But “common” isn’t the same as “ignore it.” The goal is to catch patterns early—especially if symptoms are trending worse.
Call urgently: pain that worsens, sudden vision drop, increasing redness/discharge, new light sensitivity
These are the “don’t wait it out” signs. If you’re thinking, “Maybe I’m overreacting,” consider this: the cost of a quick call is small. The cost of waiting can be large. You’re not being dramatic; you’re being protective.
Ask at follow-up: persistent foreign-body sensation, one product always triggers burning, dryness that spikes after finishing Rx drops
These patterns are common and often fixable—sometimes by adjusting the drop schedule, switching thickness, or evaluating whether you’re dealing with inflammation or surface dryness that needs a more targeted plan. Bring specifics (what you used, how often, and what happened).
On day five after a family member’s cataract surgery, we tried to be efficient. We kept one PF multi-dose bottle on the bathroom counter, so it was “easy.” Easy turned into sloppy: the cap rolled, the tip hovered too close to lashes, and the bottle got handled by three different people with three different levels of handwashing enthusiasm.
Nothing dramatic happened—no instant disaster—just a slow climb in irritation. The eye felt gritty, then burny, then “why is it worse today?” We switched to single-use vials for a week, moved everything to a clean tray, and wrote a simple drop schedule on paper. The irritation eased. The lesson wasn’t that bottles are bad. The lesson was that healing eyes punish messy systems. We didn’t need smarter products. We needed a cleaner routine.
FAQ
Many surgeons recommend PF tears during healing because post-op eyes can be more sensitive and because people often use tears more frequently during recovery. That said, follow your surgeon’s instructions—some patients need specific products or timing rules based on their eye surface and medication plan.
Single-use vials generally reduce contamination opportunities because they’re opened once and discarded. PF multi-dose bottles can be safe too, but they rely more on your technique (no tip contact) and consistent clean storage. Early post-op, many people choose vials simply because they’re easier to keep “clean by default.”
It’s generally safer to treat single-use vials as one-and-done, especially right after surgery. Reusing increases the chance of contamination from hands, surfaces, or accidental contact with lashes. If cost is the reason you want to reuse, consider a PF multi-dose system once your surgeon agrees it fits your risk level and routine.
Frequency depends on symptom severity and your surgeon’s plan. Some people use tears a few times a day; others use them more often during rough patches. If you’re using tears very frequently and still uncomfortable, that’s a signal to discuss it with your surgeon rather than endlessly increasing doses.
Spacing helps prevent one drop from washing out another. Your surgeon’s instructions come first because medication schedules vary. If you weren’t given guidance, a practical approach many clinicians use is leaving a buffer window between different drops—especially around prescription medications—so each has time to work.
Burning can come from a very dry surface, post-op sensitivity, inflammation, or simply a mismatch between the drop’s formulation and your eye’s needs. Try small tweaks first (consistent routine, clean technique, avoiding heat storage). If burning is severe, persistent, or worsening—call your surgeon.
Gel drops often last longer on the eye surface, which can help with dryness, but they can blur vision—sometimes enough to bother you during daytime tasks. Many people reserve thicker drops for evening or bedtime (if their surgeon approves), and use lighter drops during the day.
Rather than chasing a long “avoid” list, focus on choosing PF if you’re sensitive and avoiding products that repeatedly sting or trigger redness for you. If you have known allergies or you’re unsure which product is appropriate with your post-op meds, ask your surgeon for a specific recommendation.
It varies. Some people improve over weeks; others have symptoms that linger longer, especially if they had dry eye before surgery. What matters most is the trend: steady improvement is reassuring, while worsening symptoms deserve a prompt check-in.
Wash hands, avoid tip contact, recap immediately, store it clean and dry, and don’t share it. If you suspect the tip touched lashes/skin or the cap interior got contaminated, consider switching to a fresh container and contacting your surgeon for guidance—especially early post-op.
Next step: run a 3-day “clean dosing” trial (and bring data to your follow-up)
If you want the fastest path to feeling better, stop swapping products like you’re speed-dating eye drops. Do a short, clean trial. Not forever. Three days. Enough to spot patterns without turning your bathroom into a pharmacy-themed escape room.
Pick one format, follow strict no-touch dosing, and space tears away from Rx drops
- Choose one PF format (vials or multi-dose) for the trial.
- Wash hands before every dosing session.
- Use your surgeon’s schedule for prescription drops; don’t improvise.
- Keep a buffer between different drops when possible.
Log comfort + blur + “what changed today”—then adjust with your clinician
Keep it simple: morning / afternoon / night. Rate comfort (0–10), note blur (none / mild / annoying), and write one sentence about anything unusual (more screen time, windy day, missed a dose). That’s gold for your follow-up. If you want a ready-to-use format that’s easy for older adults (and caregivers) to stick with, use a printable symptom diary for seniors and keep it with your drops.
- Yes to “my hands are steady” → PF multi-dose may work well.
- Yes to “I’m anxious about contamination” → start with single-use vials.
- Yes to “someone else gives my drops” → vials often reduce mistakes.
- No to “I can keep a clean storage spot” → avoid multi-dose until you can.
Neutral next action: Choose the option you can execute flawlessly when you’re tired.
Conclusion: a clean routine beats a perfect product
Remember the curiosity loop from the top—why surgeons care about “OTC” tears? This is why: your routine is the treatment. PF tears are a tool, and packaging is a tool. The best choice is the one that helps you stay clean, consistent, and calm.
If you want a practical default: many people do well with single-use vials early post-op (lowest contamination friction), then consider a PF multi-dose system later if cost-per-day and convenience matter and your technique is solid. And if anything trends worse—pain, redness, light sensitivity, vision—don’t keep experimenting. Call.
If yes, lower your risk tolerance. “Simple” is a feature.
If no (or a caregiver is dosing), vials often prevent tip contact.
If yes, cost per day matters—run the mini calculator.
Worsening pain/redness/vision changes → call your surgeon.
- Your PF format (vial or multi-dose) and how often you dose.
- Your post-op prescription drop schedule (photo of the instructions is fine).
- What “burning” means for you (seconds vs minutes; mild vs severe).
- Whether tip contact happened (be honest; clinicians don’t judge—systems do).
Neutral next action: Save a 10-second note on your phone with these four items.
- Messy environment + high anxiety → single-use vials.
- Clean environment + steady technique + frequent dosing → PF multi-dose.
- Symptoms trending worse → call your surgeon.
Neutral next action: Pick one option and commit for 72 hours before judging it.
Last reviewed: 2025-12.