


Post-Stroke Vision Loss: Stabilizing and Rebuilding Your Visual World
The cruel part isn’t just seeing less—it’s how quickly your brain starts treating everyday spaces like hazards: patterned floors, bright grocery aisles, a doorway that suddenly “moves.” After a stroke, that shift can feel like your world shrank overnight.
If you keep guessing, the stakes are real: more near-misses, more avoidance, and a rehab plan that quietly turns into burnout. This guide helps you stabilize first—then rebuild: what to ask for at the right appointment, how scanning strategies and prisms differ, and the home-and-errands tweaks that reduce fear quickly.
It’s built around a two-track method: evaluation + friction reduction, with a “minimum effective dose” rehab so tomorrow stays bigger. We address the patterns most people miss in week two and the simple reason “pushing through” often backfires.
- Get routed to the right clinician faster
- Reduce glare, chaos, and fall risk without overhauling your life
- Spot burnout early and redesign the rehab dose
Table of Contents
Safety / Disclaimer
This article is general education, not medical advice. New or worsening vision changes after stroke can be urgent. Seek emergency care for sudden vision loss, severe headache, new weakness/numbness, confusion, trouble speaking, or fainting. If you’re in a mental health crisis or thinking about self-harm, call/text 988 (US) or emergency services.
Quick sanity rule: If your symptoms feel sudden, scary, or “not like yesterday,” treat it as time-sensitive.
Who this is for / not for
This page is for you if post-stroke vision changes have collided with anxiety and the heavy, quiet fatigue of rehab. It’s also for caregivers—the people doing the invisible logistics: rides, reminders, reassurances, paperwork, and the emotional buffering.
- For you if: you’re dealing with visual field loss (like missing a side), visual neglect, double vision, blurry vision that comes and goes, light sensitivity, or reading that suddenly feels like a puzzle.
- For caregivers if: you’re “on call” all day and finding yourself snapping, zoning out, or feeling numb.
- Not for: sudden worsening, repeated falls, severe confusion, or crisis-level distress. Those need urgent, in-person evaluation.
- You don’t have to “earn” help by suffering longer.
- Better routing often beats harder effort.
- Stability is not giving up; it’s the platform for recovery.
Apply in 60 seconds: Write one sentence: “The hardest moment of my day is ______.” That’s your starting point.
Spot the pattern: the vision clue most people miss in week 2
Here’s the sneaky part: after a stroke, “vision” problems aren’t always about eyesight. Often, they’re about how the brain scans, filters, and interprets what’s already coming in.
A familiar moment: you’re walking down a hallway, and you keep brushing one shoulder against the wall. It feels clumsy. You blame yourself. But it might be a field cut or neglect—two different problems that need different strategies.
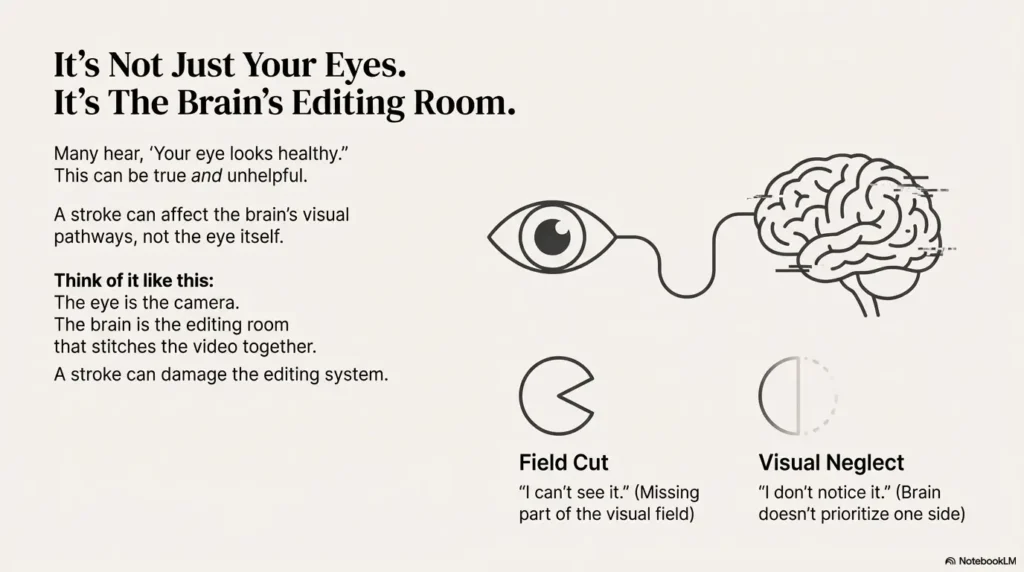
Field cut vs neglect: “I can’t see it” vs “I don’t notice it”
- Field cut (like hemianopia): you’re missing part of the visual field. You can try to look there, but it may still be blank unless you scan.
- Visual neglect: the information may be there, but your brain doesn’t prioritize it. You may forget a whole side exists until you’re reminded.
Double vision vs blurry vision: the 10-second self-check
- If you cover one eye and the “double” becomes single, it’s often an eye alignment/coordination issue (still needs proper evaluation).
- If covering one eye doesn’t change it much, it may be blur, visual processing strain, or something else worth assessing.
Reading feels impossible: scanning, tracking, or fatigue?
Reading after stroke can fail for boring reasons: your eyes don’t track smoothly; your brain loses your place; the line “slides”; or fatigue makes the letters “swim.” The fix is rarely “try harder.” It’s usually change the setup and train the right skill in small doses. If you’re trying to make reading workable again, you may also benefit from practical low-vision reading strategies like giant print options for low-vision readers (even if your condition isn’t macular degeneration—the format solutions often translate).
Open loop we’ll close later: If recovery is “possible,” why does it still feel stuck?
Why it happens: when the eyes are “fine” but vision isn’t
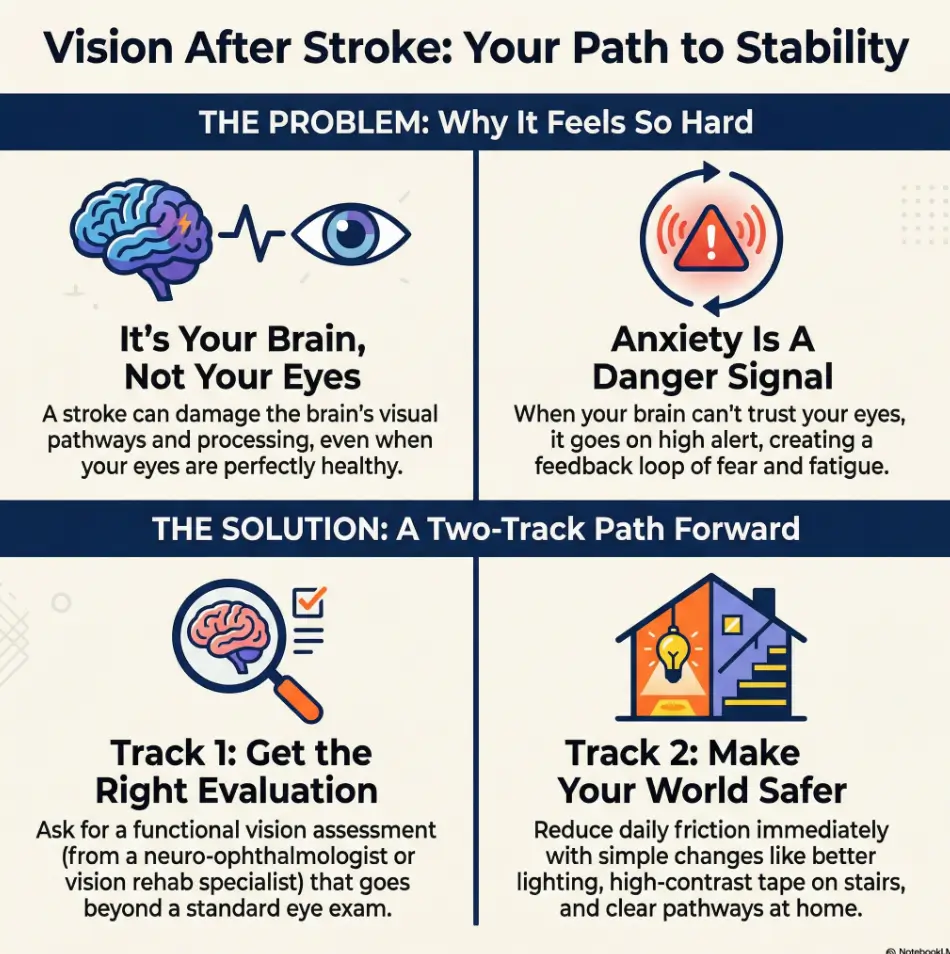
Many people hear some version of: “Your eye looks healthy.” That can be true and unhelpful. A stroke can affect the brain’s visual pathways, eye movement control, attention, and spatial processing. So you can have a normal-looking eye and still have a very real, very disruptive visual problem.
The brain’s visual pathway (plain English, no neuroscience lecture)
Think of your eye as a camera and your brain as the editing room. A stroke can damage the editing system: how the “video” is stitched together, what gets highlighted, and how your gaze moves. That’s why symptoms can show up as missing areas, scanning difficulties, trouble judging distance, or getting overwhelmed by busy environments.
Why both eyes can feel affected even with one-sided stroke
A field cut often affects the same side of vision in both eyes (because the wiring crosses and recombines). That’s confusing, and it can feel like the world is “tilted” or incomplete—especially in new places.
Open loop: If recovery is “possible,” why does it still feel stuck?
Because “possible” isn’t the same as “automatic.” The brain tends to protect you by avoiding strain. Avoidance makes sense, but it also reduces practice. The middle path is safe, structured exposure—not forcing, not hiding—so your system learns without panicking.
Anxiety loop: when your brain stops trusting your eyes
Anxiety after stroke isn’t always “worry thoughts.” Sometimes it’s your body yelling: Something is off; watch out. Vision changes can trigger that alarm—especially when you’ve had a serious health event. Your nervous system remembers.
Bright stores, patterned floors, crowds: why these settings spike fear
- Visual overload: too many edges, signs, reflections, and movement.
- Glare + contrast: harsh lighting makes scanning harder and fatigue faster.
- Unpredictability: people step into your blind side; your brain hates surprises now.
Let’s be honest—this doesn’t feel like “stress,” it feels like danger.
That sensation is the loop: vision feels unreliable → your brain goes hypervigilant → you tense and scan harder → fatigue rises → symptoms feel worse → your brain trusts your eyes even less. It’s a brutal feedback system. The fix starts with reducing load, not increasing toughness.
The “body-first” calm stack: sleep, glare, screen brightness, sensory load
- Sleep: even a small deficit can make visual processing feel jagged.
- Glare control: hats, tinted lenses (clinician-guided), softer room lighting. For home tasks, small upgrades like glare-free under-cabinet lighting choices can reduce “visual chaos” more than people expect.
- Screens: lower brightness, increase text size, reduce motion, use dark mode if it helps. If your phone still feels too bright, this guide on making an iPhone screen dimmer than the minimum can be a surprisingly big comfort win.
- Sensory breaks: short rests before you hit the wall (not after).
Micro-reset (2 minutes): breathe → orient → anchor
- Breathe: slow exhale (longer out than in) for 4–6 cycles.
- Orient: name 3 stable objects you can see (chair, doorframe, lamp).
- Anchor: put one hand on a solid surface and feel its temperature/texture for 10 seconds.
- Reduce glare and chaos before you demand courage.
- Short, planned exits beat white-knuckling.
- Your nervous system learns safety through repetition.
Apply in 60 seconds: Pick one “hard place” (store, hallway, stairs) and name one friction you can remove today.
Short Story: The Grocery Aisle Contract (120–180 words) …
They hadn’t cried in the hospital. Not after the scans, not after the discharge paperwork, not even after the first missed step on the porch. But in the grocery store—under those white ceiling lights, with cereal boxes shouting in neon—the tears came fast. “I can’t do this,” they whispered, gripping the cart like it was a railing on a ship. The caregiver did what most of us do: tried to solve everything at once. “We’ll be quick.
We’ll just push through.” That made it worse. So they made a small contract instead: one aisle only, then a break in the car. They set the phone brightness low, wore a cap to cut glare, and used a simple rule—scan left-right at intersections like crossing a street. Ten minutes later, it wasn’t victory. It was something better: proof the day could be negotiated.
Rehab burnout decoded: are you tired—or is your plan quietly punishing you?
Rehab burnout looks like laziness from the outside. Inside, it feels like your brain is sandpapered. You don’t want encouragement. You want the world to stop touching you.
Burnout signals: avoidance, irritability, “I can’t do one more drill”
- Skipping therapy homework, then feeling guilty (which doesn’t help).
- Snapping at small questions: “Did you do your exercises?”
- Brain fog: reading a text twice and still not absorbing it.
- Sleep that doesn’t restore you.
Open loop: Why “more therapy” can produce less progress
Because fatigue changes the signal. When you’re depleted, you practice mistakes. Your nervous system gets threat-y. Your attention shrinks. It’s like learning piano while someone slams a door every 20 seconds. The brain can’t build clean patterns under constant alarm. If screens and reading are a big part of your day, you may also recognize “burnout” as plain old digital eye strain patterns layered on top of neuro-fatigue.
The “minimum effective dose” rule: shorter, steadier, recoverable
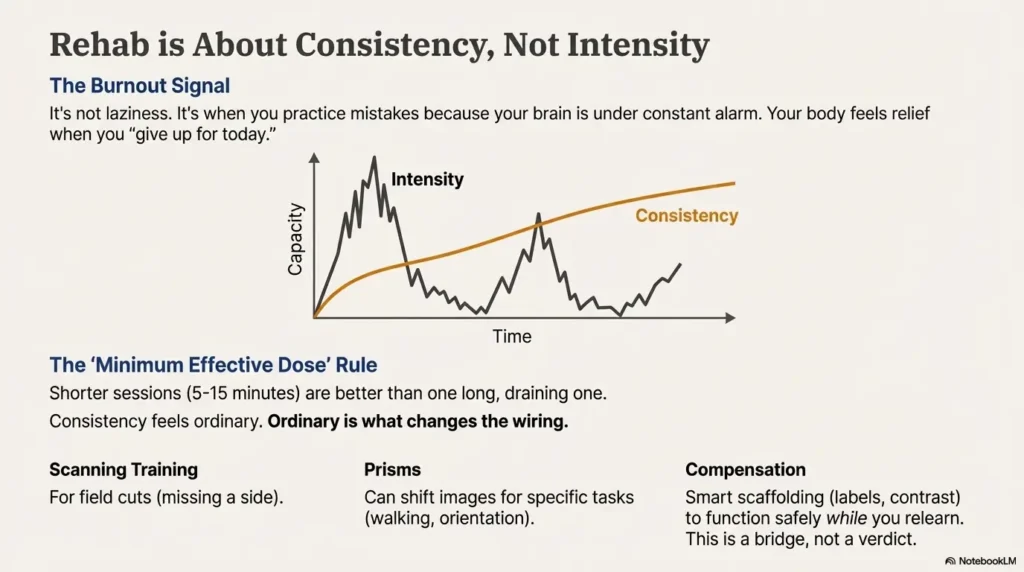
If rehab is a marathon, burnout is sprinting the first mile. A sustainable approach often looks boring: shorter sessions (5–15 minutes), more frequent breaks, and clear stopping rules. That’s not coddling. That’s training design.
Here’s what no one tells you about rehab: consistency beats intensity.
Intensity feels heroic. Consistency feels ordinary. Ordinary is what changes the wiring.
- Yes/No: Symptoms worsen with longer practice sessions.
- Yes/No: You avoid tasks you used to attempt, even small ones.
- Yes/No: After effort, anxiety spikes or sleep gets worse.
- Yes/No: You feel relief when you “give up for today.”
- Yes/No: You can do more on some days, then crash hard.
Neutral next step: If you answered “Yes” to 3+, try a 7-day lower-dose plan and track how you feel.
Right evaluation: don’t waste the appointment (what to ask for)
US healthcare can feel like a maze on a good day. After a stroke, with vision changes and anxiety, it can feel impossible. The goal of your next appointment isn’t to tell your whole story. It’s to get the right evaluation pathway.
Beyond a standard eye exam: “functional vision” and neuro-vision angles
A standard exam may focus on eye health and acuity. Post-stroke problems may need a functional and neurological lens: visual fields, eye movements, attention/neglect screening, reading/tracking function, and how symptoms show up in real life.
Who does what: neurology vs ophthalmology vs neuro-ophthalmology vs neuro-optometry
- Neurology: stroke follow-up, broader neurological symptoms, referral coordination.
- Ophthalmology: eye health, retina/optic nerve issues, some alignment problems.
- Neuro-ophthalmology: intersection of brain and vision; often ideal for complex post-stroke visual changes.
- Neuro-optometry / vision rehab specialists: functional assessment, targeted training/compensation strategies (availability varies).
Mistake to avoid: describing symptoms too vaguely (“my vision is off”)
Clinicians can’t route you from “off.” They can route you from specific scenarios. You’re not being dramatic; you’re being usable.
Bring this: 5 real-life examples that unlock better care
- “I bump into doorframes on my left/right.”
- “I miss food on one side of the plate.”
- “I feel panicky in bright stores or crowds.”
- “Reading lines jump or I lose my place after 2 minutes.”
- “Stairs feel unsafe; I misjudge the last step.”
💡 Read the official vision-after-stroke support guidance
Rehab options compared: scanning vs prisms vs vision therapy vs compensation
You’ll hear a lot of terms. Let’s make them less mysterious, and more decision-ready. None of these are magic. Many are helpful—when matched to the right problem.
Scanning training: the workhorse for field cuts
If you have a field cut, scanning strategies can be practical and powerful: deliberate left-right search patterns, “anchor points” on the page, and intersection routines for walking. It’s the visual version of learning to check mirrors—at first it’s effortful, then it becomes automatic.
Prisms: what they do (and what they don’t)
Prisms can shift images and may help in certain situations, but they’re not a universal fix. They can also feel odd at first. The key question to ask isn’t “Do prisms work?” It’s “Work for what task—walking, reading, orientation, double vision?”
Eye movement rehab + double vision: when exercises help
If double vision is part of the picture, the plan may involve alignment strategies, specific eye movement work, or other clinician-guided options. The caution here is simple: don’t DIY aggressive drills when symptoms flare hard. Small, correct practice beats big, messy practice.
Compensation: safety now, recovery later (using both wisely)
Compensation isn’t surrender. It’s smart scaffolding: using contrast, labels, consistent layout, and safer routes so you can function while your brain relearns. Think “training wheels,” not “permanent limitation.”
Open loop: How do you tell “helpful challenge” from “symptom flare”?
Helpful challenge usually produces tired-but-okay and steadier function over time. A flare produces spike-and-crash: anxiety surges, sleep worsens, and tomorrow is smaller. Your body is feedback. We’ll build a simple way to measure it in a minute.
Show me the nerdy details
When clinicians talk about “vision after stroke,” they’re often tracking function, not just acuity: visual fields, saccades (quick eye jumps), smooth pursuit (tracking), and attentional load. Training aims to reduce search time, errors, and fatigue. Progress is usually measured by real-world tasks (navigation, reading endurance, fewer collisions), not a single eye chart number.
- Choose A (Scanning-first) if you miss one side, bump into things, or feel lost in doorways.
- Choose B (Double-vision pathway) if images split, closing one eye changes it, or headaches/eye strain spike fast.
- Choose “Compensation now” if safety is shaky or fatigue is dominating the week.
Neutral next step: Pick the one pathway that matches your most dangerous moment and start there.
Make life safer: the home + errands checklist that lowers fear fast
Here’s a truth that feels unfair: anxiety often improves when your environment stops ambushing you. Safety changes reduce near-misses. Fewer near-misses reduce the “danger” signal. That’s not psychology. That’s physics + nervous system. If you want a practical model for “home safety with low vision,” this home-safety checklist mindset (originally written for another condition) can still help you spot hazards fast.
One-room upgrade: light, contrast, clutter, clear paths
- Light: reduce glare; use softer, even lighting.
- Contrast: dark mat on light floor, or light mat on dark floor—pick one.
- Clutter: keep a clear path in your most-traveled route (bedroom → bathroom → kitchen).
- Consistency: put essentials in the same place every time (keys, meds, phone).
Stairs + bathrooms: the two zones to fix first
- Add contrast to stair edges (non-slip tape can help, but choose safe options).
- Use grab bars and non-slip mats where appropriate.
Night lighting: enough to see edges, not enough to glare. For a step-by-step approach, see
low-vision nighttime bathroom safety fixes.
Reading + screens: glare control, font rules, “stop before the spiral”
Reading is a high-load task. If you push past your limit, symptoms stack: strain → anxiety → frustration → shutdown. A simple rule helps: stop at 7/10, not 10/10. Stopping early keeps tomorrow bigger. If medication instructions or labels are part of your reading stress, options like large-print prescription labels can reduce daily friction more than another “try harder” session ever will.
Support map (US): where to find help—and what to do when it’s urgent
Support should not require a superhuman to access it. Here’s a practical map in US terms—starting with the “closest door” you can actually open.
Stroke support + community: stop doing this alone
- American Stroke Association: educational resources and community pathways.
- Hospital rehab programs: often have groups or social work navigation.
- Local support groups: if in-person is too much, ask for virtual options.
Vision rehab & low-vision support: what “OT” can mean here
Occupational therapy (OT) is often the practical bridge: scanning strategies, home setup, safe routines, task adaptation, and getting the right referral chain moving. Low-vision services can also help with tools and training when vision changes persist—especially when daily logistics like pills and schedules become stressful. If that’s part of your week, consider practical systems like low-vision medication management to reduce errors and anxiety at the same time.
Counseling for adjustment + anxiety: what to look for (low-burden, skills-based)
- Short, skills-based therapy (for panic, avoidance, sleep routines).
- Trauma-informed support (stroke can be traumatic).
- Caregiver support (because “I’m fine” is not a plan).
When it’s urgent: don’t negotiate with red flags
- Sudden vision loss or rapid worsening.
- New weakness/numbness, confusion, trouble speaking.
- Repeated falls or near-falls that are escalating.
- Thoughts of self-harm or feeling unsafe: call/text 988.
- 1-page symptom script (5 bullets + worst 2 scenarios)
- Medication list and major diagnoses
- Last discharge summary (if available)
- Fall/near-miss notes (date + what happened)
- One goal you care about (reading 10 minutes, safe stairs, grocery aisle)
Neutral next step: Put these in one folder (paper or phone) so you’re not re-explaining every time.
Common mistakes: the “helpful” habits that quietly backfire
These are common because they’re emotionally reasonable. They just don’t work long-term.
Mistake #1: “I’ll just push through” exposure
Forcing yourself into high-glare, high-chaos environments without supports can teach your brain one lesson: “This is dangerous.” It’s not bravery training. It’s threat conditioning. Better: controlled exposure with an exit plan.
Mistake #2: skipping vision-specific rehab because “eyes look normal”
A normal eye exam doesn’t rule out post-stroke functional vision issues. Don’t let “normal” end your investigation if daily life is clearly not normal.
Mistake #3: waiting for spontaneous recovery as a plan
Some recovery happens with time. But function often improves most when time is paired with targeted practice and better setup. “Wait and see” can quietly become “avoid and shrink.”
Mistake #4: hiding symptoms to avoid being a burden
Hiding makes you look “fine,” which delays help. A short script is kinder to everyone than long suffering.
- Challenge is useful only when it’s recoverable.
- Specific symptoms get better referrals than vague distress.
- Compensation is a bridge, not a verdict.
Apply in 60 seconds: Write one “exit plan” for your hardest place (time limit + break spot + ride plan).
Next step: the 15-minute plan that turns chaos into a pathway
This is the part where you don’t need motivation. You need a small action that creates momentum.
Write a “symptom script” (5 bullets) + “impact list” (3 situations)
Symptom script: what happens, where, how often, what makes it worse.
If you want a printable format (especially helpful for caregivers), try a
printable symptom diary template
and bring it to appointments.
- Impact list: 3 tasks affected (stairs, reading, stores, driving, work screens).
Pick one call: the best available door
- Primary care (routing + referrals)
- Neurology follow-up
- Ophthalmology / neuro-ophthalmology clinic
- Rehab intake / OT
Ask for one thing: evaluation + referral routing (not “everything at once”)
Try: “I need a functional evaluation of my post-stroke vision issues and the right referral pathway. Here are five specific examples.” That sentence is surprisingly powerful.
This isn’t a diagnosis. It’s a simple way to decide whether your plan needs less load today.
Score: —
Neutral next step: Use the output to adjust your day (shorter sessions, more breaks, lower-glare environments).
FAQ
Can vision come back after a stroke, and how long does it take?
Sometimes vision improves over time, especially in the early months, but recovery varies widely. The most reliable approach is to pair time with targeted evaluation and practical training—so you’re not waiting in the dark (literally and emotionally).
What’s the difference between a visual field cut and visual neglect?
A field cut is missing part of the visual field; neglect is an attention/awareness issue where the brain doesn’t prioritize one side. They can look similar day-to-day, but the strategies and therapy targets can differ.
Why does post-stroke vision loss trigger anxiety or panic?
Because your brain uses vision to predict safety. When vision feels unreliable—especially after a major health event—your nervous system can flip into “protective mode.” The good news: predictability and small wins often calm it faster than willpower.
What kind of doctor should I see for vision problems after stroke?
Start with the best available door (primary care or neurology) for referral routing. If possible, neuro-ophthalmology is often well-suited for brain-vision overlap. OT and vision rehab specialists can be key for functional improvements.
Do prisms or vision therapy help after stroke?
They can help in specific scenarios, depending on the underlying issue (field loss, double vision, eye movement control). The “right answer” is usually task-based: what helps walking may not help reading. Ask what the intervention is designed to improve and how progress will be measured.
How do I cope with rehab burnout without “giving up”?
By redesigning the dose. Burnout often improves when you shorten sessions, add recovery, and target one task at a time. Consistency beats intensity—especially when fatigue and anxiety are part of the system.
When is a vision change after stroke an emergency?
Seek urgent care for sudden vision loss, rapid worsening, severe headache, fainting, new weakness/numbness, confusion, trouble speaking, or repeated falls. If you feel unsafe or in crisis, call/text 988.
Conclusion
Remember the open loop from earlier—why recovery can feel “stuck” even when it’s possible? Often it’s because your brain is protecting you. It avoids strain, it avoids surprise, it avoids danger. That protection is understandable. It’s also negotiable.
The path that works is rarely dramatic. It’s stability first: safer environments, clearer routing, small practice doses, and support that reduces the load you’re carrying. Then, quietly, capacity grows.
If you have 15 minutes today, do one thing: write the symptom script, pick one door to call, and ask for functional evaluation + referral routing. You don’t need the perfect plan. You need the first step that keeps tomorrow bigger.
💡 Read the official low-vision rehab guidance
💡 Read the official 988 crisis support guidance
Last reviewed: 2026-01.