


The 200mg Rule: Stability for Your Vision
Table of Contents
Safety / Disclaimer (read first)
This article is educational—not medical advice. Eye pressure (IOP) is important, but it’s only one piece of glaucoma risk. Your optic nerve appearance, retinal nerve fiber layer imaging, and visual field results matter just as much (sometimes more). If you’re on prescription drops, do not change them based on caffeine alone. Use this plan as a conversation tool—something you can bring to your ophthalmologist or optometrist to personalize your routine.
Also: “glaucoma suspect” is a wide bucket. Some people are flagged because of borderline pressures, some because of family history, some because of optic nerve shape, and some because of corneal thickness that makes readings tricky. So the goal here isn’t to “win” against coffee. It’s to stop coffee from quietly interfering with measurements or amplifying a risk pattern you’re already watching.
- Keep caffeine steady (avoid surprise spikes).
- Don’t test your eye pressure right after coffee.
- Bring a simple “mg + timing” note to your appointment.
Apply in 60 seconds: Look at your mug. If it’s bigger than 8–10 oz, stop calling it “one cup.”
Who this is for / not for
For you if…
- You’re 65+ and labeled glaucoma suspect, ocular hypertension, or “watching pressures.”
- You want a safe coffee limit that is practical—not a life lecture.
- You have an upcoming visit and you don’t want caffeine to mess with the numbers.
Not for you if…
- You have diagnosed glaucoma with progression, complex meds, or recent surgery—your clinician’s plan comes first.
- You’re having emergency symptoms (scroll to “When to seek help”).
A quick, human moment: a lot of readers tell me the hardest part isn’t even coffee. It’s the uncertainty. You can live with “do X.” What breaks you is “maybe X, maybe not.” This is why we’re building a rule that works even when you’re tired, busy, and not in the mood to negotiate with your latte.
- Yes → You’re being monitored for IOP, optic nerve, or visual fields.
- Yes → You drink caffeine at least 3 days/week.
- Yes → Your eye appointments are usually in the morning.
- No → You have severe side effects from caffeine (palpitations, panic, insomnia).
- No → You recently had eye surgery or new severe symptoms.
Next step: If you answered “yes” to the first three, use the timing rule in the next section before your next IOP check.
Safe limit: start with a “two-number rule” (mg + timing)
The mg anchor: a practical daily ceiling
Let’s start with a number you can actually use: ~200 mg/day as a cautious baseline for glaucoma suspects, especially after 65. Not because 201 mg is dangerous and 199 mg is holy—but because it nudges you toward moderation without mystery. Many adults tolerate more, but the whole point of being “suspect” is that you’re managing uncertainty. A tighter range reduces noise.
Here’s the uncomfortable truth: studies show caffeine can create a small, temporary IOP rise in some people. Not everyone. Not always. Often it fades. But if you’re the kind of person whose eye pressure already trends higher, or you’re being evaluated at the margins, you don’t want a “maybe” factor on top.
The timing anchor: protect your measurement window
This is the part that matters more than most people realize: timing. If you drink coffee right before an IOP check, you might nudge the number upward—enough to create unnecessary stress, repeat testing, or a medication discussion that’s based on a distorted snapshot.
A practical timing rule: avoid caffeine for a few hours before IOP testing unless your clinic tells you otherwise. Some offices prefer “keep your routine the same,” especially for consistency across visits. Others prefer “avoid caffeine.” The safe move is to ask once, then follow that office’s rule every time so your results are comparable—and if you want to know what your clinic is actually measuring, it helps to review what happens during a glaucoma test so you can align your routine to the testing method.
Show me the nerdy details
IOP is not a single fixed number. It can vary across the day, across visits, and with factors like hydration, body position, stress, and measurement technique. Caffeine’s effect—when it shows up—tends to be short-lived and varies by individual sensitivity. That’s why timing can matter more than your lifetime coffee identity (“I’m a coffee person”).
A small confession from the “regular humans club”: if you’re like most people, you don’t drink coffee because you love caffeine math. You drink it because mornings are hard. So we’ll keep this plan gentle: you’re not quitting joy; you’re removing spikes and protecting test-day accuracy.
- Option A: 0–1 coffee/day → Choose this if your pressures are borderline, you’re newly labeled “suspect,” or you’re anxious about test-day variability.
- Option B: 1–2 coffees/day (split) → Choose this if you tolerate caffeine well and want steadier energy without spikes.
- Option C: energy drink / “pre-workout” → Avoid as a default if you’re a suspect; the delivery pattern is often spiky and the label can be misleading.
Neutral action: Pick A or B for the next 7 days, then evaluate sleep and appointment-day numbers.
Why glaucoma suspects react differently (and the part genetics may play)
The open loop: why “coffee is fine” isn’t always fine
You’ll hear two loud opinions online: “Coffee is totally safe!” and “Coffee will ruin your eyes!” Both are oversimplified. The more honest answer is quieter: average effects can look small, while subgroups (people with higher baseline IOP, higher risk profiles, or certain biological sensitivities) can react differently.
If you’re a glaucoma suspect, you’re already living in the land of “subgroup.” You might have thin corneas that make readings look lower than they truly are. Or a strong family history. Or an optic nerve that your doctor wants to watch closely. In that context, “moderate” matters more than it does for someone with rock-solid low pressures and no risk markers—and it can help to compare your situation against glaucoma vs normal aging so “normal for age” doesn’t get confused with “safe to ignore.”
The “high intake” zone to be cautious with
Where caution becomes more reasonable is at high daily caffeine intake—especially if it’s delivered in a tight window. This isn’t about moralizing your morning. It’s about avoiding patterns that can create a repeatable, avoidable physiologic “bump.”
If you want a simple boundary: treat very high daily caffeine (multiple strong coffees plus additional sources) as a “red zone” for glaucoma suspects unless your clinician has told you your pressures and optic nerve are stable and you’re consistent across visits.
This is also where genetics gets talked about, sometimes too confidently. Some research suggests that people with a higher genetic predisposition to elevated IOP may show stronger associations with high caffeine intake. The practical takeaway is not “get a genetics test.” It’s: don’t assume population averages apply perfectly to you.
One more lived-human note (from the inbox, not the ivory tower): people who do best long-term usually don’t “quit.” They standardize. Same drink, same timing, same routine before visits. That consistency is a form of kindness—especially when you’re dealing with a condition measured in millimeters and years. If your clinician is watching pressures but your numbers aren’t sky-high, you may hear about normal-tension glaucoma after 60 as a reminder that “pressure” is only one part of the story.
Coffee math that actually works (so you don’t undercount)
“Just drink one cup” is the kind of advice that sounds helpful until you meet a modern mug. Coffee math matters because caffeine content varies wildly by brew method, bean, roast, and volume. Two people can both say “one coffee” and be hundreds of milligrams apart.
Quick conversions (labels you’ll actually see)
- Small brewed coffee is often treated as roughly ~1 serving, but “small” can mean 8 oz or 12 oz depending on where you buy it.
- Espresso shots feel tiny but can add up fast—especially if your “one drink” is actually a double or triple.
- Decaf isn’t zero. If you’re very sensitive, decaf can still matter—especially if you drink it late.
A tiny story from reader reality: one person told me they “cut down to one coffee,” but it was a 20 oz travel mug refilled once. That wasn’t a character flaw. It was a measurement problem. Fix the measurement and the anxiety drops by half.
The container is the hidden variable.
Count each caffeine event like you’d count pills.
This is a rough estimate using typical values. It won’t be perfect—but it will expose “hidden doubles.”
Estimated total: 95 mg/day
In the “cautious baseline” zone for many glaucoma suspects.
Neutral action: If your number surprises you, swap one item for half-caf or decaf for a week and re-check sleep + appointment consistency.
The hidden caffeine sources that “steal” your limit
If you’re tracking caffeine for eye pressure, the usual suspects are obvious: coffee, espresso, tea. The sneaky sources are the ones that feel “small” and therefore uncounted—cola, chocolate, “energy” waters, and some pain or cold products that add stimulants. You don’t need paranoia; you need awareness. If you’re flirting with that 200 mg/day baseline, hidden sources are often the reason you’re over it without realizing.
Operator tip: don’t try to count everything forever. Count carefully for 3 days, learn your pattern, then switch to a simpler rule (like “two caffeine events max per day”). If you like tracking on paper, a printable symptom diary for seniors can make the log feel less like homework and more like a calm record you can hand to your clinician.
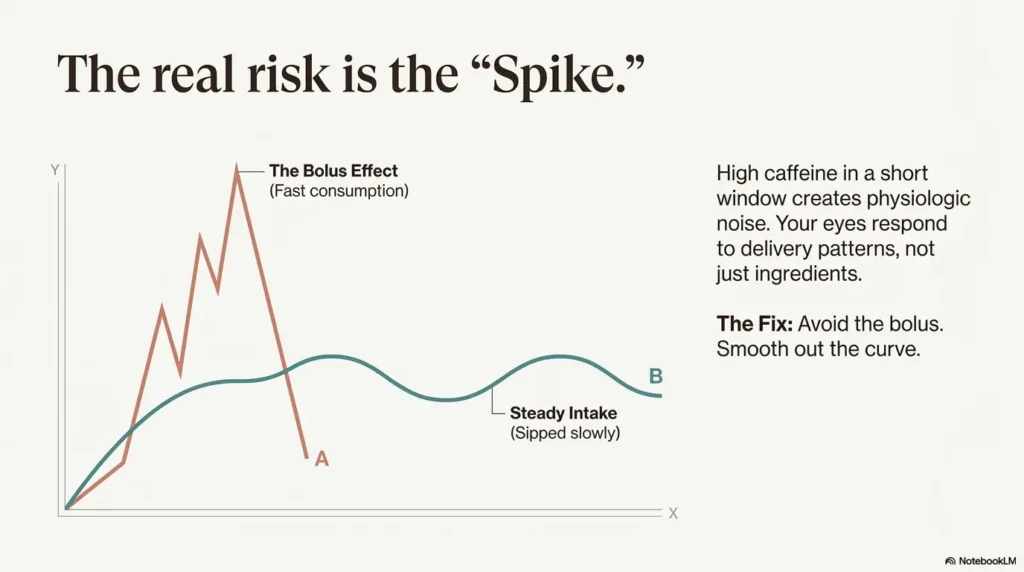
The real risk isn’t coffee—it’s the pattern of caffeine delivery
Smooth dose vs. spike dose
If you take one idea from this entire article, make it this: spikes are the problem long before “moderate coffee” is the problem. A big caffeine load in a short window is more likely to produce noticeable short-term physiologic effects—jittery heart, shallow sleep, anxious edge—and for some people, a measurable IOP bump.
This is why many glaucoma suspects do fine with one normal coffee (especially with food), but feel weird after a strong energy drink or a double-shot on an empty stomach. Your eyes don’t read branding. They respond to delivery.
Let’s be honest…
Many “I only drink one coffee” routines are actually 16–24 oz and consumed like water because you’re trying to be functional. No shame. But if you’re a glaucoma suspect, your best move is to make your caffeine boring: measured, predictable, and not fused to appointment mornings.
- Your usual caffeine schedule (time + drink type).
- Your mug size (8 oz vs 16 oz vs 20 oz).
- Whether you had caffeine before your last IOP check.
- Sleep quality (good/okay/bad) the night before testing.
- Any symptoms: palpitations, anxiety, headaches, insomnia.
Neutral action: Write this on a sticky note in under 2 minutes and bring it to your next visit.
Common mistakes (the avoidable ones)
Mistake #1: Chugging coffee right before your eye-pressure check
This one is brutally common. You’re rushing, you’re nervous, you’re in a chilly waiting room, and coffee feels like emotional support. Then you get a slightly higher IOP reading and spend the rest of the day spiraling. Even if the caffeine effect is modest, you don’t want accidental inflation when the whole point of monitoring is to detect real change.
Mistake #2: Treating “decaf” as caffeine-free
Decaf is lower, not zero. For most people, decaf won’t matter much. For caffeine-sensitive people—especially those who get insomnia from “tiny” stimulants—it can still count. If you’re doing the “3-day threshold” test later in this article, treat decaf as a variable, not a loophole.
Mistake #3: Switching to energy drinks “because they feel lighter”
Energy drinks can concentrate caffeine into a fast spike. Some also include other stimulants that make you feel “wired” even when the label doesn’t look outrageous at first glance. If you’re a glaucoma suspect trying to keep things stable and measurable, this is the exact opposite of what you want.
A small, sympathetic aside: I’ve watched people become stricter about coffee while ignoring sleep, stress, and dehydration—things that can also make you feel terrible and show up as noisy readings. Don’t get trapped in “coffee is the only lever.” It’s just the easiest lever to measure. (If screen time is part of your late-day fatigue spiral, it can also help to review digital eye strain in seniors so your “less caffeine” plan doesn’t accidentally become “more squinting and headaches.”)
The “3-day personal threshold” test (glaucoma-suspect friendly)
Day 1–3 protocol (simple, realistic)
This is not a biohacker experiment. It’s a gentle calibration—something you can do while living your life.
- Day 1: Keep your usual caffeine routine, but write down timing and drink type.
- Day 2: Cap at ~200 mg/day (or your closest equivalent) and split into 2 smaller “events.”
- Day 3: Do the same cap, but shift caffeine earlier (avoid late afternoon/evening).
Track three things only (keep it humane): sleep, anxiety/jitters, and headache. These often determine your real-world limit more than glaucoma does—because if caffeine wrecks sleep, stress rises, routines drift, and you end up doing weirder caffeine patterns to compensate.
Short Story: The morning the numbers jumped (120–180 words) …
Short Story: The morning the numbers jumped (120–180 words) … A reader once described a perfectly ordinary appointment morning: early alarm, quick shower, and “just one coffee” on the drive. The clinic was running behind, so the coffee got finished faster than usual—half on an empty stomach. The pressure reading came back a bit higher. Not a crisis number, but high enough to trigger that sinking feeling: Is this the start of something?
The rest of the visit turned into a blur of worry and half-heard instructions. The next week, they did the same appointment time but skipped caffeine until after the test. The number was lower and steadier. The point wasn’t that coffee “caused” glaucoma. The point was that coffee can add noise. When you’re monitoring a slow-moving condition, reducing noise is a kind of relief—and a kind of accuracy.
What to bring to your next appointment
Bring a one-line log: “Caffeine mg estimate + timing + symptoms”. If your office uses Goldmann applanation tonometry or a tonopen, the measurement is still a snapshot—so your job is to make snapshots comparable. If you’re also navigating Medicare coverage decisions, it may help to understand whether you’re considered high risk for glaucoma on Medicare and how that affects screening and follow-up expectations.
If your clinic also tracks visual fields (often on a Zeiss Humphrey Field Analyzer) or does OCT imaging, tell them whether caffeine affects your anxiety or shakiness. Field tests, especially, are vulnerable to “bad days,” and caffeine can either help focus or make you twitchy. That’s useful clinical context.
When to seek help (don’t wait on caffeine experiments)
Urgent / same-day care if you have
- Sudden severe eye pain
- Red eye with nausea/vomiting
- Sudden vision loss
- Halos around lights with intense headache
These can signal serious eye emergencies, including acute angle-closure glaucoma. This is not a “wait and see” situation, and it’s not a “try decaf and hope” situation.
Call your eye doctor soon if
- You notice new peripheral vision changes.
- Night driving glare suddenly feels worse.
- Your blood pressure meds or sleep patterns changed and your symptoms shifted.
A practical note for the 65+ crowd: dehydration, new meds, and poor sleep can sneak into your eye story. If you’re adjusting caffeine, do it gently and pay attention to overall stability—because stability is what your care team is chasing. For a broader frame, it can help to review age-related eye diseases after 60 so you can separate “urgent,” “soon,” and “routine monitoring” without panic.
FAQ
1) Does caffeine raise eye pressure in glaucoma suspects?
It can in some people, and when it does, the change is usually temporary. The most useful approach isn’t panic—it’s consistency: avoid large caffeine spikes and keep test-day conditions comparable.
2) How long does caffeine affect intraocular pressure?
The effect—when present—tends to be short-lived rather than a full-day event. This is why timing around your IOP measurement matters so much.
3) Is one cup of coffee safe if I’m a “glaucoma suspect”?
Often, yes—especially if it’s a normal-sized coffee and you’re not stacking other caffeine sources. If you want a cautious starting point, aim around ~200 mg/day and see how your sleep and appointments look.
4) Should I stop caffeine before my eye-pressure test?
Ask your clinic what they prefer. Many people choose to avoid caffeine for a few hours before testing to reduce measurement noise. The bigger goal is consistency across visits—same approach each time.
5) Does decaf coffee still affect eye pressure?
Decaf typically contains less caffeine, but not always zero. If you’re very caffeine-sensitive or doing a threshold test, treat decaf as “low caffeine” rather than “no caffeine.”
6) Do espresso shots raise IOP more than drip coffee?
Not because espresso is morally worse—because the delivery can be concentrated. A double or triple shot taken quickly can act more like a spike than a slow-sipped drip coffee.
7) Can caffeine worsen glaucoma progression, or is it just temporary IOP changes?
Progression is complex and involves more than IOP alone. The more practical concern for most suspects is short-term measurement noise and whether caffeine disrupts sleep or stress—factors that can destabilize routines and follow-up care.
8) What’s a safer substitute—tea, half-caf, or decaf?
For many people, half-caf is the sweet spot: familiar ritual, less spike. Tea can be gentler for some, but it’s still caffeine. Decaf can help if you’re sensitive or you drink coffee late.
9) If I have ocular hypertension, is my caffeine limit different?
It might be. If your pressures are consistently high, your clinician may prioritize minimizing avoidable IOP bumps. A cautious baseline (~200 mg/day) plus a spike-avoidance rule is a reasonable starting plan to discuss.
Next step (one concrete action)
For the next 7 days, do this one simple thing: cap caffeine at about ~200 mg/day, avoid big boluses, and keep caffeine out of the few hours before any scheduled IOP or visual field testing (unless your clinic instructs otherwise). Then bring a one-line log to your next appointment: “estimated mg + timing + symptoms.”
- Choose a baseline cap you can actually sustain.
- Split caffeine into smaller events instead of spikes.
- Standardize test-day behavior so readings are comparable.
Apply in 60 seconds: Decide your rule for appointment mornings now (skip until after testing, or follow your clinic’s instruction), then stick to it every visit.
If you want an official benchmark for general caffeine intake, the U.S. Food and Drug Administration discusses common daily limits for adults and why sensitivity varies—useful context when you’re setting your personal cap.
And if you want a clean, patient-friendly overview of glaucoma—what it is, how it’s monitored, and why early detection matters—the National Eye Institute’s overview is a solid place to anchor your understanding.
Long-tail keywords (US phrasing, 12–20)
If you’re researching for yourself (or helping a parent), these are useful search phrases to save—especially when you want practical, appointment-relevant answers:
- safe coffee limit for glaucoma suspect
- caffeine intraocular pressure after 65
- does coffee raise eye pressure glaucoma suspect
- how much caffeine is safe with ocular hypertension
- should glaucoma suspects avoid caffeine
- caffeine before eye pressure test
- how long does caffeine raise IOP
- decaf coffee glaucoma suspect eye pressure
- espresso vs drip coffee eye pressure
- best caffeine amount for older adults with high eye pressure
- coffee and glaucoma risk genetics
- energy drinks and eye pressure glaucoma suspect
PAA questions (8–12)
These are excellent “ask your clinician” questions—because they force the conversation to become personal instead of generic:
- Does caffeine increase my eye pressure immediately—or only sometimes?
- Should I avoid caffeine before my specific IOP test method?
- How consistent do you want my routine across visits?
- Do my corneal thickness and optic nerve findings change how we interpret pressure?
- Is my glaucoma risk more about IOP, optic nerve appearance, or visual fields?
- If I switch to half-caf, how long until you’d expect readings to stabilize?
- Does my blood pressure treatment or sleep quality affect my glaucoma risk strategy?
- If I’m anxious during testing, how should I manage caffeine without harming sleep?
- Do you recommend home monitoring (like iCare HOME) for my case?
- What would count as meaningful change versus normal variability?
Differentiation map
| What most content does | What this guide does instead |
|---|---|
| Says “moderation” without a usable rule | Gives a mg + timing plan you can run this week |
| Treats “cups” like a standard unit | Forces mug math and exposes hidden doubles |
| Ignores appointment behavior | Protects the measurement window so numbers stay comparable |
| Overpromises (“coffee causes glaucoma” / “coffee is always safe”) | Uses risk-aware language and focuses on spikes + consistency |
| Generic lifestyle listicles | A suspect-specific system: avoid spikes, standardize visits, bring a log |
We should close the curiosity loop from the beginning: you came here asking for a “safe coffee limit” because you don’t want to accidentally hurt your eyes. The safest, most honest answer is a plan that reduces noise and avoids spikes—not a dramatic ban. Coffee isn’t automatically your enemy. Unmeasured, spiky caffeine patterns and test-day chaos are the bigger risk to clear monitoring.
If you have 15 minutes today, do the simplest version: measure your mug, decide your baseline cap, and set your appointment-morning rule. That’s it. You’ll walk into your next visit with less fear—and more control. If you’re already building a broader “stay consistent” routine, pairing this with an annual eye exam checklist for seniors can help you track what questions and tests matter most year to year.
Last reviewed: 2026-01.