
What Happens During a Glaucoma Test? 9 Scary Moments I Didn’t Expect (and the Ultimate Step-by-Step Fix)
The Glaucoma Workup:
From Panic to Pattern-Finding
The weirdest part of my first glaucoma workup wasn’t the machines. It was the quiet handoffs—room to room—where nobody tells you what the next step will feel like.
If you’ve ever left an eye appointment thinking you “messed up” the test (too jumpy for the air puff, too tired for the visual field, too blurry after dilation), you’re not alone. Keep guessing, and you risk wasted visits, noisy results, and a plan built on confusion instead of clean data.
A glaucoma test is usually a bundled set of measurements that check eye pressure (IOP), optic nerve health, and vision function—often including dilation, corneal thickness (pachymetry), OCT imaging, and sometimes gonioscopy to assess the drainage angle. It’s not pass/fail; it’s pattern-finding over time (especially when you’re sorting glaucoma vs normal aging changes).
This guide shows what happens during a glaucoma test—step by step—so you can prep in minutes, stay steady during the visual field test, and walk out with one clear next step (plus fewer cost surprises).
Here’s the 5-minute plan. Then the 9 moments that spike panic. Then the calm script that fixes the whole day.
Table of Contents
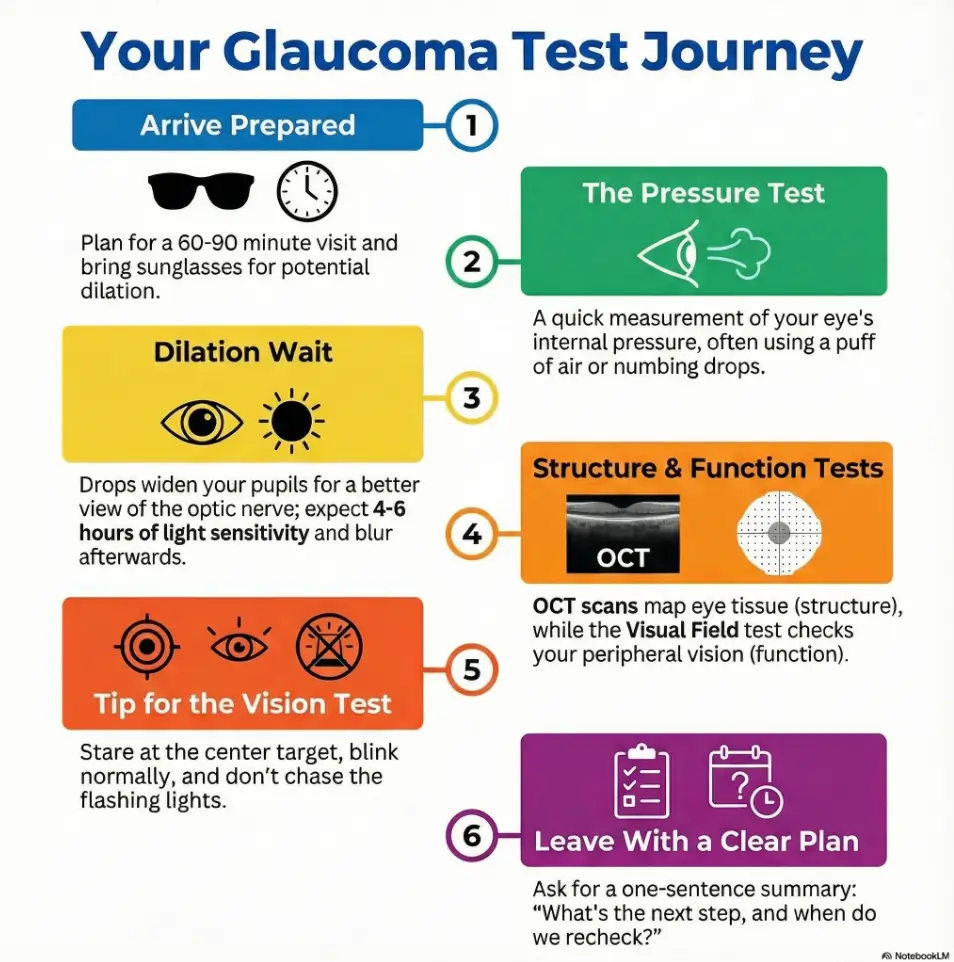
Before you go: the 5-minute plan that prevents 3 avoidable surprises
I walked into my first glaucoma test like it was a simple “eye check.” I walked out like I’d been through a tiny, polite obstacle course.
Here’s the truth: a glaucoma workup is usually a bundle of tests. Some are fast (under 2 minutes). Some take 10–15 minutes and demand focus. And if you’re dilated, your vision can be off for 4–6 hours, which is a fun surprise if you planned to drive or stare at spreadsheets after.
My 5-minute pre-visit plan:
- Bring the actual drops you use (or a phone photo of the label). Names blur together under stress—especially if you’ve ever had to sort glaucoma eye drops side effects in seniors from “just a weird day.”
- Wear easy-off layers. You’ll lean into machines; collars and scarves become enemies.
- Plan time like a grown-up: block 60–90 minutes if it’s a first-time workup.
- Skip caffeine 2–3 hours if it spikes your jitters. You’ll perform better in the visual field test.
- Bring sunglasses. I didn’t. I became a squinting vampire at noon.
- Block 60–90 minutes for a full workup
- Assume dilation may affect you 4–6 hours
- Bring your med list or bottle photo
Apply in 60 seconds: Screenshot your current drops and insurance card into one album named “Eye Visit.”
- Your insurance plan type (HMO/PPO), deductible status, and remaining out-of-pocket maximum
- Referral status (yes/no) and whether you’re in-network
- Which tests are likely today: eye pressure, visual field, OCT, photos, pachymetry
- If you need prior authorization for imaging in your plan (some do)
- Your schedule constraints: can you return for a second test day or must it be same-day?
Next step: Save this list and ask the clinic for a written estimate that includes the test names (or codes, if they provide them).
Scary Moment 1: The eye pressure test that feels like a jump-scare
I used to think “eye pressure test” meant one thing. It can mean air puff, a handheld device, or the classic method with numbing drops and a blue light. The first time, I flinched so hard I practically tried to blink my eyeball back into my skull.
What’s actually happening: they’re measuring intraocular pressure (IOP). It’s one risk signal for glaucoma, not the whole story.
Two things that made mine go smoother:
- Exhale during the moment. Your body reads “hold your breath” as “panic now.”
- Let your eyelids be heavy, not clenched. I didn’t know that tension can mess with the reading.
Time cost: usually 1–3 minutes. Emotional cost: temporarily 7 years off your lifespan if you’re jumpy like me.
- Yes if you have severe eye pain + nausea, sudden halos, sudden major vision loss, or a red painful eye with headache.
- Yes if one pupil is suddenly much larger and you feel “pressure” like a drum.
- No if it’s just mild blur after dilation or mild scratchy feeling after drops—those are common and usually temporary.
Next step: If any “Yes,” call an eye emergency service or urgent ophthalmology line and describe symptoms in one sentence—especially if you’ve been asking yourself “is it just getting older, or is this serious eye disease?”
Scary Moment 2: The bright slit lamp “interrogation light”
The slit lamp looks like a friendly microscope until the light hits your eye and you realize you’ve never practiced “staring politely” in your life.
This step lets the clinician examine the front of your eye—cornea, iris, lens—and often the optic nerve after dilation. It can feel intense because your face is locked into a chin rest, and the instructions come fast: “Look up. Now left. Don’t move.”
What helped me: I picked a tiny “anchor point” on the wall behind the doctor and pretended I was watching a calm concert conductor. (I needed the metaphor. I’m not ashamed.)
Typical time: 5–10 minutes, depending on how much they’re checking.
Show me the nerdy details
Slit lamp biomicroscopy uses a narrow beam of light and magnification to inspect ocular structures in layers. It’s also a common setup for applanation tonometry and for evaluating the optic nerve head after dilation.
Micro-humor truth: this is the part where you learn you have a dominant eye… because one side is dramatically worse at “hold still.” Mine tries to freestyle.
Scary Moment 3: Dilation—when your day quietly changes for 4–6 hours
Nobody told me dilation would turn my afternoon into a soft-focus film. I had planned to “pop back to work.” Reader, I could not read my own phone without holding it like a lighthouse.
What dilation does: it opens the pupil so the clinician can see the back of your eye—optic nerve, retina—more clearly. This is often essential in glaucoma assessment, and it overlaps with what you’d get in dilated eye exams for seniors.
What it feels like: light sensitivity, blur up close, sometimes a weird “big-eyed” sensation. Not pain. Just annoyance.
Numbers that matter:
- Blur and light sensitivity can last 4–6 hours (sometimes less, sometimes more).
- Expect a 10–20 minute wait for drops to fully kick in.
- Bring sunglasses
- Don’t schedule high-stakes driving right after
- Plan 10–20 minutes for the drops to work
Apply in 60 seconds: Put sunglasses in the bag you actually carry (not the “organized” bag you admire from afar).
Scary Moment 4: Corneal thickness numbers that can change the story
This was the first moment I realized glaucoma testing is not one single reading—it’s interpretation. They measured my corneal thickness and suddenly the conversation shifted from “pressure number” to “pressure number plus context.”
Why it matters: corneal thickness can influence IOP measurement. Two people can show the same pressure reading and have different real-world risk profiles depending on corneal properties and optic nerve findings.
What it feels like: usually quick—sometimes a light touch, sometimes a device close to the eye. For most people it’s under 2 minutes.
My small embarrassment: I asked, “Is thicker better?” like we were shopping for winter socks. The clinician smiled in a way that said, “You’re not the first.”
Scannable truth:
- IOP is a signal, not a verdict.
- Thickness is a context tool, not a scary test.
- Your risk picture comes from patterns over time (including risk factors like family history of eye disease).
Scary Moment 5: Gonioscopy—yes, that lens touches your eye
“We’re going to place a special lens on your eye.” That sentence sounds like a dare.
This checks the drainage angle—basically, the anatomy where fluid leaves the eye. This matters because glaucoma risk and treatment can vary depending on whether your angle is open, narrow, or blocked.
What it feels like: you’ll typically get numbing drops, then a lens gently contacts the eye. It’s weird, not painful. The weirdness is mostly psychological—your brain is screaming, “EYE CONTACT IS NOT SUPPOSED TO BE LITERAL.”
Time: often 2–5 minutes.
- Tier 1: screening-style visit only; minimal testing; lowest out-of-pocket
- Tier 2: pressure + optic nerve exam + dilation; adds time and temporary blur
- Tier 3: adds visual field or OCT (often the “real data day”)
- Tier 4: adds repeated tests (reliability check) or specialist interpretation
- Tier 5: adds treatment planning, laser discussion, or medication changes
Next step: Save this map and ask which tier your visit is likely to be before you arrive—especially if you’re navigating high-risk glaucoma rules on Medicare.
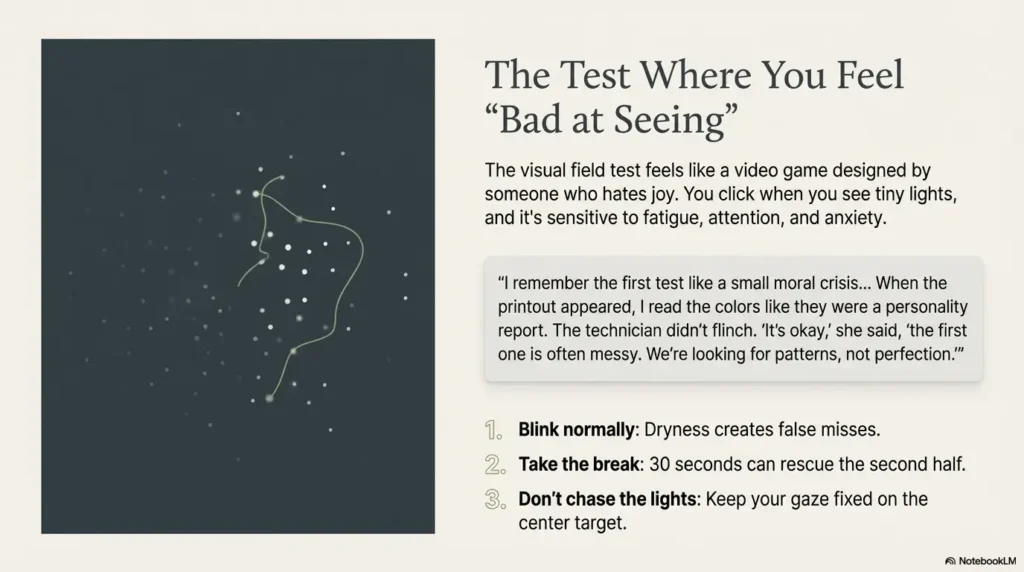
Scary Moment 6: The visual field test where you feel “bad at seeing”
This is the one that made me sweat. You sit at a bowl-shaped machine, stare at a central target, and click when you see tiny lights. It feels like a video game designed by someone who hates joy.
What’s actually happening: they’re mapping your peripheral vision—one of the key functional measures in glaucoma. The test is sensitive to fatigue, attention, dry eye, and anxiety. Which is comforting. (Kidding. But it’s important.)
Typical time: about 5–10 minutes per eye. If you’re tested both eyes, add setup time and short breaks.
Three “operator” tips that improved my results:
- Blink normally. Dryness creates false misses.
- Take the break if they offer it—30 seconds can rescue the second half.
- Don’t chase the lights. Keep your gaze on the center target; your brain will want to hunt.
Short Story: The day I thought I “failed” the glaucoma test (120–180 words)
I remember the first visual field test like a small moral crisis. The room was dim, the machine hummed, and I tried to be a “good patient” the way people try to be a “good listener” at a concert—too much effort, too much self-awareness. Halfway through, I started guessing. I clicked when I wasn’t sure. Then I panicked and stopped clicking. My shoulders crept up to my ears. When the printout appeared, I read the colors like they were a personality report.
The technician didn’t flinch. “It’s okay,” she said, “the first one is often messy. We’re looking for patterns, not perfection.” That sentence changed my whole posture. On the second try, I blinked, breathed, and treated it like a steady metronome. The result wasn’t magical. It was just honest—and that’s what they needed.
Show me the nerdy details
Automated perimetry often includes reliability indicators such as fixation losses and false positives. Clinics frequently repeat the test when reliability is low or when results don’t match other findings.
- Expect 5–10 minutes per eye
- Blink normally to reduce false misses
- Ask for a short break if fatigue hits
Apply in 60 seconds: Before the test starts, ask: “Can you remind me if I’m moving my eyes?”
Scary Moment 7: OCT scans and the panic of the word “thinning”
OCT is the step that feels the most “modern.” You stare at a target, the machine scans, and then—sometimes—someone says the word “thinning.” That word lands like a stone.
What OCT does: it measures layers of retinal tissue and the optic nerve region. It’s structural data. Helpful, but not destiny. Many things can affect readings: anatomy differences, signal strength, eye movement, and even how dry your eye is that day.
Time: often 2–6 minutes, depending on the device and how cooperative your blink reflex is.
My tiny lived lesson: I tried to “help” by not blinking. My eyes watered. The scan got worse. The machine did not applaud my sacrifice.
Show me the nerdy details
OCT creates cross-sectional images and thickness maps. Clinicians often review signal quality and trend analysis across multiple visits rather than relying on one snapshot.
Scannable reframe:
- Visual field = function (how you see)
- OCT = structure (what the tissue looks like)
- Glaucoma decisions = both, over time (including diagnoses like normal tension glaucoma after 60)
Scary Moment 8: The risk conversation that sounds like a verdict
This is where many people emotionally crash—not because of pain, but because language gets heavy. “Suspect.” “Damage.” “Progression.” Even if the clinician is calm, your brain may translate it into: I’m going blind soon.
What the clinician is usually trying to do: sort you into a risk bucket and decide what makes sense next: monitor, start drops, adjust drops, consider laser, or investigate other causes.
My rule now: I don’t leave the room without one sentence that tells me the plan. I literally ask for it. It’s my adult version of a receipt.
- Choose A: Monitor first if results are borderline, reliability was low, or the clinician wants a repeat test in 4–12 weeks. Time cost: another visit. Money cost: another copay or test fee. Benefit: cleaner baseline.
- Choose B: Treat now if pressure is consistently high, optic nerve looks clearly suspicious, or the clinician sees matching OCT + visual field patterns. Time cost: daily drops. Money cost: ongoing copays/out-of-pocket. Benefit: risk reduction earlier.
Next step: Save this card and ask: “What is the one data point that would change your recommendation?”
Small humor that helped me: I stopped saying “I’m sorry” when I asked questions. I’m not asking for a favor. I’m asking for my vision plan—and if your risk picture includes diabetes, it’s worth knowing how Medicare glaucoma screening works for diabetics.
Scary Moment 9: Cost, codes, and coverage tiers in 2025
Even if you’re emotionally steady, cost can still knock you sideways—especially when “it’s just a test” becomes multiple line items. If you’re comparing providers, insurance quotes, or coverage tiers, this is the section that saves time.
First: the honest truth. Costs vary by clinic, region, and plan. Your deductible, in-network status, and prior authorization rules can matter as much as the test itself.
US readers (quick localization): If you’re using Medicare or a commercial plan, ask whether imaging and functional testing are billed separately, and whether your plan requires a referral or prior authorization for certain diagnostics (and whether you qualify as high risk for glaucoma on Medicare).
UK readers (quick localization): If you’re in the NHS pathway, timing and follow-up intervals may be standardized, while private testing can be faster but comes with direct fees. Ask what’s included in the package: visual field, OCT, photos, and repeat testing if reliability is low.
Korea readers (quick localization): Many ophthalmology clinics offer same-day testing, but coverage can depend on medical necessity and how services are billed under national insurance. Ask for an itemized estimate and whether repeat tests are expected if today’s baseline is unreliable.
| Test | Code (often used in estimates) | Typical self-pay quote range (2025) | Notes to ask |
|---|---|---|---|
| Visual field test | 92083 | $80–$250 | One eye or both? Repeat if unreliable? |
| OCT (optic nerve) | 92133 | $120–$350 | Is it baseline + comparison report? |
| Fundus photos | 92250 | $60–$200 | Are photos required if OCT is done? |
| Pachymetry | 76514 | $20–$90 | One-time baseline or repeated? |
| Gonioscopy | 92020 | $40–$150 | Is it included in the exam fee? |
Next step: Save this table and confirm the current fee on the provider’s official page or written estimate.
- Clarify in-network vs out-of-network
- Ask about deductible and prior authorization
- Request a written estimate with test names (or codes)
Apply in 60 seconds: Send one message: “Can you list which glaucoma tests are planned today and whether dilation is likely?”
The ultimate step-by-step fix: a calm script for your next glaucoma test
This is the part I wish someone had handed me on a single card. Not a pamphlet. Not a lecture. A script.
Step-by-step, in order:
- Before you leave home (2 minutes): pack sunglasses, a med list, water, and a snack if you get shaky. Set a 90-minute buffer if it’s a full workup day.
- At check-in (30 seconds): ask, “Will I be dilated today?” If yes, decide now about driving.
- Before pressure testing (10 seconds): inhale, exhale, soften eyelids. Tell them if you’re a strong blinker—no shame.
- Before visual field (20 seconds): ask for a quick coaching reminder: “Center target, blink normally, take a break if needed.”
- After OCT/photos (15 seconds): ask, “Is this baseline or are you comparing to older scans?” Baseline feels scary but it’s the start of clarity.
- At the plan conversation (60 seconds): ask for one sentence: “What are we doing next, and why?” Then ask one more: “When do we recheck?”
- Before you walk out (60 seconds): schedule the follow-up while you’re still there—4–12 weeks is common for repeats when the first data is noisy.
Next step: Save your estimate and confirm the test bundle with the clinic before you arrive.
Confirm dilation, meds, and time limits.
~3 min
Air puff or numbing + measurement.
~1–3 min
Drops + wait for full effect.
~10–20 min
OCT/photos + optic nerve look.
~5–15 min
Visual field test (focus + blinking).
~10–20 min
One-sentence next step + follow-up timing.
~5–10 min
Use it: If you’re overwhelmed, point to the step you’re on and ask what comes next. Clarity lowers anxiety fast.
- Ask early if dilation is planned
- Perform the visual field test like a steady metronome
- Leave with one sentence: next step + timing
Apply in 60 seconds: Write one question in your notes app: “What would change the plan?”
FAQ
1) How long does a glaucoma test appointment take?
For a first-time workup with imaging and visual field testing, plan for 60–90 minutes. If it’s a quick follow-up (pressure check + brief exam), it might be 15–30 minutes. 60-second action: call and ask, “Is this a full workup day with dilation and visual field?”
2) Does the glaucoma test hurt?
Most steps feel strange, bright, or annoying—not painful. Numbing drops can prevent discomfort during contact-based tests. 60-second action: tell the technician, “I blink hard—please coach me through it.”
3) Can I drive after a glaucoma test?
If you’re dilated, driving can be risky for 4–6 hours because of blur and light sensitivity. Some people feel fine; others don’t. 60-second action: ask at check-in whether dilation is planned and decide transportation early.
4) What if my visual field test is “bad” because I was nervous?
That happens. Visual field testing is sensitive to fatigue and anxiety, and clinicians often repeat it if reliability is low. One test is rarely the whole story. 60-second action: request a short break between eyes if you feel yourself spiraling.
5) What’s the difference between OCT results and the visual field results?
OCT is structural (tissue patterns). Visual field is functional (what you actually detect). Clinicians often compare both over time to confirm patterns. 60-second action: ask, “Is today’s OCT a baseline or a comparison to prior scans?”
6) How do I reduce out-of-pocket costs for glaucoma testing?
Ask for the planned test bundle in advance, confirm in-network status, and request a written estimate with test names or codes. Deductible and authorization rules can matter. 60-second action: send one message: “Please list the planned tests and whether any require authorization.”
7) What should I ask at the end of the appointment?
Ask for one clear plan sentence: what you’re doing next and when you’re rechecking. Then ask what data point would change the plan. 60-second action: write the next appointment date down before you leave the building—right next to your annual eye exam checklist for seniors if you keep one.
Last reviewed: 2025-12.
Conclusion: the next 15 minutes that matter
Remember the hook—the silence between steps? That silence isn’t a medical mystery. It’s just missing narration.
Now you have the narration: what each test is, what it usually feels like, and how to walk through it like someone who’s done it before—even if you haven’t.
Do this in the next 15 minutes:
- Write down three questions: “Will I be dilated?”, “Is this baseline or comparison?”, “What would change the plan?”
- Make an “Eye Visit” album with your drops, insurance card, and last prescription—and if you like structure, keep a simple printable symptom diary for seniors so you don’t rely on memory in the exam room.
- Send one message to the clinic asking for the planned test bundle and expected time.
If you only take one thing from this: glaucoma testing isn’t pass/fail. It’s a trend story. Your job is to show up prepared enough that the story is clear—and the plan is simple (and yes, that’s part of protecting your long game, the same way people think about blindness risk after 70 without letting fear run the show).