

Glaucoma Eye Drops Side Effects in Seniors: 7 Scary Signs I Missed Before We Switched
Glaucoma Eye Drops: Side Effects in Seniors
The first “glaucoma problem” that scared us wasn’t blurry vision—it was a near-fall on a quiet Tuesday morning, followed by a resting pulse that didn’t match how tired the body looked.
Glaucoma eye drops side effects in seniors are what happens when a medication meant for the eye behaves like a whole-body drug. It can drain through the tear duct, enter the bloodstream, and show up as dizziness, slow pulse, brain fog, breathing changes, or crushing fatigue—especially with beta-blocker drops like timolol or sedating agents like brimonidine.
When you keep chalking it up to “just aging,” you lose time—and sometimes safety. If you’ve ever wondered is it just getting older—or could it be serious eye disease showing up sideways? you already understand the trap.
This guide helps you sort urgent vs. annoying, spot dose-timing patterns, and walk into the next appointment with clean, usable data. We didn’t solve this with panic. We solved it with a timeline, pulse checks, and a regimen that fit a real human.
Here’s the fast clarity you’ve been missing:
- The seven signs that hide in plain sight.
- The 2-minute technique (nasolacrimal occlusion) that reduces systemic absorption.
- The switch plan that protects pressure control while reducing irritation.
Table of Contents
Reserved space to keep layout stable.
Why seniors get hit harder by glaucoma drops
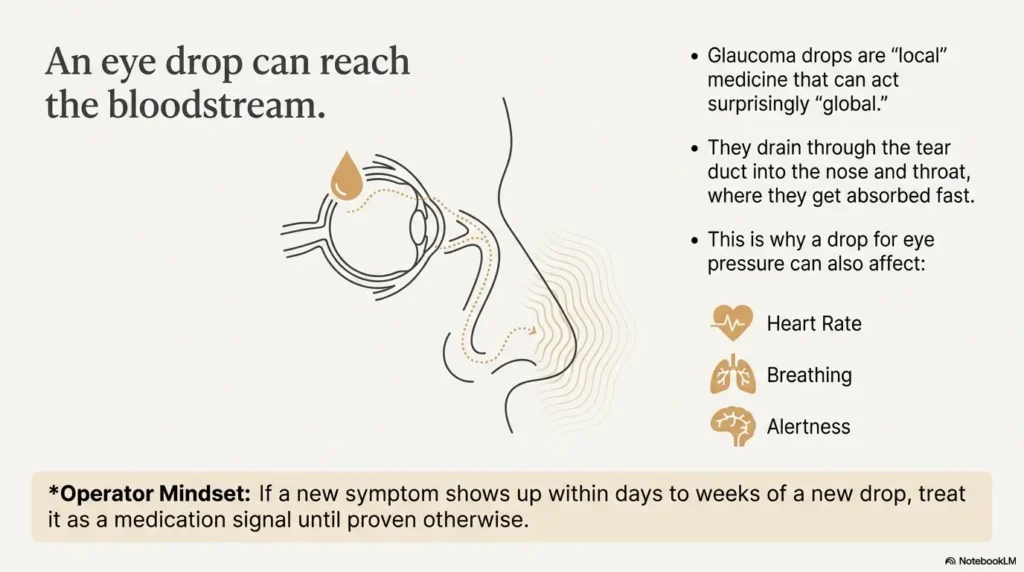
Glaucoma drops are “local” medicine that can act surprisingly “global.” In seniors, a few things stack the deck: thinner tear film, slower metabolism, more heart and lung conditions, and—most importantly—more other medications that can collide with the drop’s systemic effects.
Here’s the part I wish someone had said to me plainly: an eye drop can reach the bloodstream. It can drain through the tear duct into the nose and throat, where it gets absorbed fast. That’s why a drop designed to lower eye pressure can also nudge heart rate, blood pressure, breathing, alertness, and energy—especially in people who are already medically “busy.”
I learned this the embarrassing way. I kept treating the bottle like it was harmless because it was small. A “tiny” dose, I told myself. Then I watched a family member get unusually wiped out after starting a new regimen—and I still blamed the weather.
Operator mindset: If a new symptom shows up within days to weeks of a new drop, treat it as a medication signal until proven otherwise.
Show me the nerdy details
Topical ophthalmic drugs can be systemically absorbed via the nasolacrimal drainage pathway. This is why techniques like eyelid closure or nasolacrimal occlusion after instillation are commonly recommended to reduce systemic exposure, especially for agents with cardiopulmonary or CNS effects.
The 7 scary signs we missed (and what they can mean)
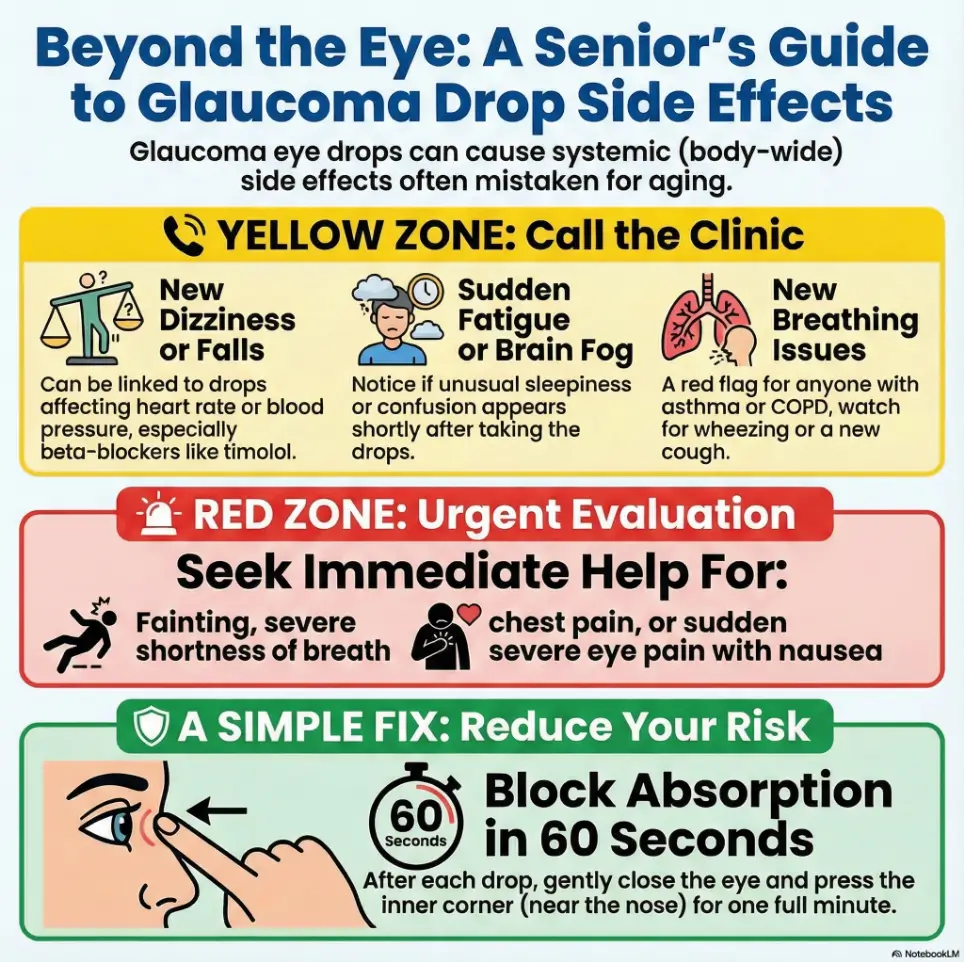
These are the signs that made us pause, re-check timing, and ultimately talk to the ophthalmologist about changing the plan. None of them automatically mean “stop your drops,” but they do mean “don’t shrug.”
- Slow pulse or “my heart feels quieter” — can happen with beta-blocker drops like timolol, especially if paired with other heart-rate–lowering meds.
- Dizziness, faintness, or new falls — sometimes a blood pressure or heart-rate issue in disguise.
- Confusion, unusual sleepiness, or mental fog — can be medication-related, especially in frail seniors.
- Breathing changes, wheeze, tight chest, or a cough that won’t quit — a red flag in people with asthma or COPD when using beta-blocker drops.
- Extreme fatigue that feels “heavier than normal” — especially if it tracks with dosing time.
- Depressed mood, vivid dreams, or irritability — sometimes a CNS effect that gets mislabeled as stress.
- Red, burning, gritty eyes that make the person “avoid the bottle” — often an ocular surface problem that ruins adherence and results.
- Watch timing: new symptom within days–weeks matters
- Track pulse, falls, and fatigue patterns
- Bring the full med list to the eye appointment
Apply in 60 seconds: Write down the drop name, dose time, and the first day the symptom appeared.
Urgent exceptions: sudden severe shortness of breath, fainting, chest pain, one-sided weakness, sudden vision loss, or a painfully red eye with nausea can be emergencies. Don’t “blog your way” through those—get urgent care. If you’re stuck in the “maybe it’s nothing” loop, glaucoma vs normal aging can help you frame what belongs in the “don’t shrug” category.
Slow pulse, dizziness, and falls after beta-blocker drops in 2025 (US/Korea)
If there’s one scenario that deserves extra respect in seniors, it’s this: a beta-blocker glaucoma drop plus a body that already runs slow.
Non-selective beta-blocker drops like timolol are well-known for lowering intraocular pressure. But they can also lower resting pulse and affect breathing in susceptible people because they may be absorbed systemically. In older adults, that can translate into a very un-glamorous chain: slower pulse → lightheadedness → a stumble → a fall → weeks of recovery.
I hate how ordinary it looked. “Just a little dizzy.” “Just tired.” It was only when we took a pulse—twice, at two different times of day—that we saw the pattern. And yes, I felt ridiculous for not doing it sooner. But that’s the point: these side effects are sneaky because they masquerade as normal aging.
- What to check today: Resting pulse and blood pressure before the morning dose and 1–2 hours after.
- What to bring to the doctor: A list of all heart meds (beta blockers, calcium channel blockers, digoxin, some antiarrhythmics), plus any history of fainting.
- What not to do: Don’t stop abruptly without medical advice if the drop is controlling pressure—call the eye clinic and explain the symptoms.
Show me the nerdy details
Because beta-blockers can have systemic cardiopulmonary effects, labels commonly warn about bradycardia, conduction problems, and bronchospasm in at-risk patients. The risk can rise when combined with other medications that also lower heart rate or blood pressure.
Fatigue, confusion, and mood changes that look like “just aging”
This is where families get gaslit by normal life. Seniors get tired. Seniors get forgetful. And yet: medications can amplify those exact symptoms—and glaucoma drops are not magically exempt.
Alpha agonist drops like brimonidine can cause sleepiness, fatigue, and reduced alertness in some people. Beta-blocker drops have also been associated with fatigue and, in some cases, mental cloudiness—effects that can land harder in older adults who already have thin margins for sleep and energy.
Our “tell” was timing. The fog didn’t feel random. It clustered around dose windows, like a curtain dropping. I remember thinking, half-joking, “It’s like someone dimmed the lights in the brain.” And then feeling guilty for even thinking it—because glaucoma is serious, and you don’t want to blame the treatment. But you’re allowed to notice reality.
Small test that saves time: Track “alertness 0–10” for 3 days. It takes 30 seconds a day, and it gives your doctor usable signal.
- Look for dose-timing patterns
- Ask if a preservative-free or different class is reasonable
- Bring sleep meds and antihistamines into the conversation
Apply in 60 seconds: Write one sentence: “The fog starts about __ minutes after the __ dose.”
Breathing changes, wheeze, and “mystery cough” in seniors with COPD/asthma
If your parent has asthma, COPD, or even “winter bronchitis that keeps coming back,” a beta-blocker glaucoma drop deserves careful handling. Some people do fine. Others don’t. The danger is that symptoms can look like a cold—until they don’t.
I still remember the moment we connected the dots: a tight chest that showed up without fever, without obvious infection, and kept repeating on the same schedule. It wasn’t dramatic. It was just… persistent. And in older adults, “persistent” is often the real alarm.
- Watch for: Wheeze, shortness of breath, chest tightness, new night cough, reduced exercise tolerance.
- Especially important if: There’s a history of asthma, COPD, or smoking-related lung disease.
- What to ask: Whether a different drug class (for example, a prostaglandin analog) is appropriate, or whether the drop choice should change given respiratory history.
Eligibility checklist: Are you higher-risk for systemic side effects?
- Yes/No: Asthma or COPD history
- Yes/No: Resting pulse often below 60
- Yes/No: Past fainting, unexplained falls, or heart block
- Yes/No: Using other heart-rate–lowering meds
- Yes/No: New fatigue/confusion after starting the drop
Next step: If you answered “Yes” to any item, call the eye clinic and ask for a medication review focused on systemic side effects.
Save this checklist and confirm the current guidance with your clinician or the medication label.
Red, gritty eyes: preservatives, dry eye, and the quiet adherence killer
Not all “side effects” are dramatic. Some are just miserable enough to make a senior quietly stop using the drops. That’s the adherence cliff—where eye pressure rises because the bottle becomes the enemy.
Burning, stinging, gritty sensation, tearing, and blurred vision can come from the medication itself, from the acidity of some formulations, or from preservatives that irritate the ocular surface over time. Benzalkonium chloride is a common preservative in glaucoma medications and has been studied for its potential to contribute to ocular surface issues with chronic exposure. In real life, it shows up as the complaint you hear over breakfast: “My eye feels like sand.”
My mistake was treating that complaint like whining. I thought, “It’s a necessary inconvenience.” But if the sensation is strong enough, people skip doses. Then you’re paying for a treatment that isn’t actually happening.
- Practical fixes: Ask about preservative-free options, changing the dosing schedule, or adding preservative-free lubricating drops (with spacing so they don’t wash out the glaucoma med).
- Operator tip: If you use multiple drops, separate them by 5–10 minutes so each medication has a chance to work.
- Reality check: A “red eye” can also be allergy, infection, or a separate eye condition—if pain is severe or vision changes suddenly, get checked urgently.
- Preservatives can matter over months and years
- Spacing drops prevents “washout”
- Comfort improves adherence, which protects vision
Apply in 60 seconds: Ask: “Is there a preservative-free version of this medication or a different class with fewer surface side effects?”
Coverage tier map: Regimen intensity from Tier 1 to Tier 5
One drop nightly. Lowest friction. Often easiest for seniors.
One drop twice daily. Add a simple reminder system.
Two drops daily. Spacing rules start to matter.
Three+ instillations/day. Higher odds of missed doses.
Multiple meds + side effects. Consider simplifying or alternatives.
Save this map and confirm the simplest effective tier with your ophthalmologist.
How to cut systemic absorption in 2 minutes (technique beats willpower)
This is the “tiny move” that can change the whole experience: after you put the drop in, gently close the eyelids and/or press the inner corner of the eye (near the nose) to reduce drainage into the tear duct. Research over the years has shown this can meaningfully reduce systemic absorption for some drops, including timolol, and it can also improve local effectiveness. The point isn’t perfection—it’s consistency.
When we finally did this correctly, we felt like we’d discovered a cheat code that had been sitting in plain sight. I was annoyed. Then relieved. Then annoyed again. (This is my emotional range as a caregiver: two chords and a drumbeat.)
- Step 1: Instill one drop (more is not better; it mostly spills out).
- Step 2: Close the eye gently, don’t squeeze.
- Step 3: Press the inner corner lightly for 60 seconds.
- Step 4: If you have a second drop, wait 5–10 minutes.
Mini calculator: What does this regimen really cost in time?
This is not about money. It’s about friction. Lower friction usually means better adherence.
Save this estimate and confirm the simplest effective regimen with your clinician.
Infographic: Side effect triage map (seniors on glaucoma drops)
Mild stinging for 10–30 seconds, mild redness, mild taste in mouth.
Do: improve technique, space drops, track symptoms.
New fatigue, brain fog, dizziness, rash around eyes, worsening dry eye, repeated missed doses.
Do: request med review and alternatives.
Fainting, severe shortness of breath, chest pain, sudden severe eye pain with nausea, sudden vision loss.
Do: urgent care or emergency services.
This is guidance for decision-making, not a diagnosis. When in doubt, choose safety.
Switching without losing pressure control: the practical options
Switching drops can feel like gambling with vision. That fear is real. But side effects can also sabotage vision if they cause skipped doses or falls that derail everything. The goal is not “tough it out.” The goal is the simplest regimen the patient can actually follow.
Common adjustment paths your ophthalmologist may consider:
- Change the drug class: for example, moving from a beta-blocker to a prostaglandin analog if appropriate.
- Change the formulation: gel-forming options, different concentration, or different dosing schedule.
- Reduce preservative load: preservative-free or lower-preservative versions, especially when ocular surface symptoms dominate.
- Simplify the routine: combination drops may reduce the number of daily instillations (not always possible, but sometimes a game changer).
I once tried to “be helpful” by suggesting a complicated schedule that would make an airline pilot sweat. The doctor gently simplified it in 30 seconds. That’s your reminder: complex plans fail quietly at home.
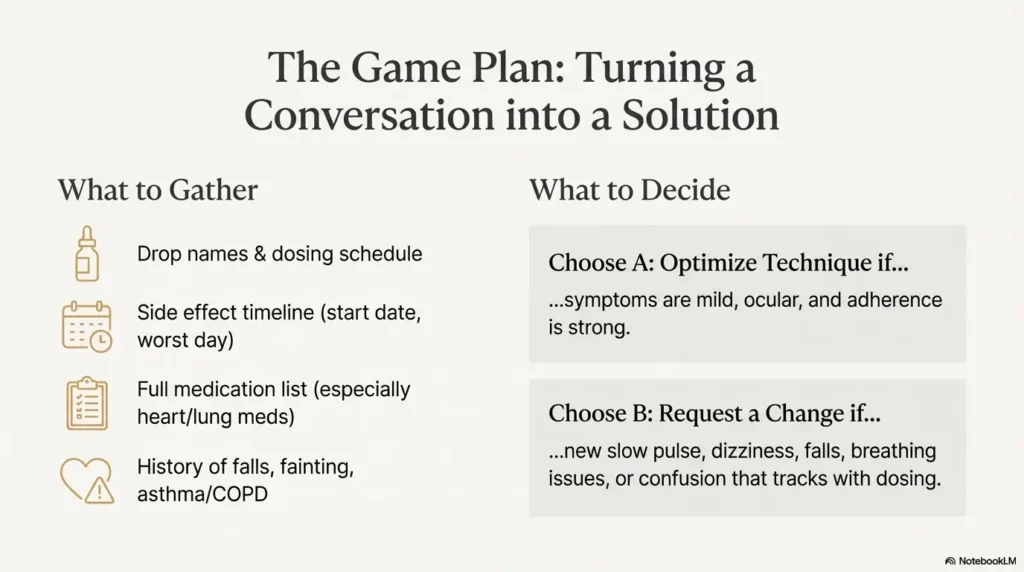
Decision card: When to ask for a switch vs when to optimize technique
- Symptoms are mild and mostly ocular
- No falls, fainting, or breathing issues
- Adherence is still strong
Time/cost trade-off: 1–2 minutes per dose, but fewer systemic effects risk.
- New slow pulse, dizziness, or falls
- Breathing symptoms in asthma/COPD
- Confusion/fatigue that tracks with dosing
Time/cost trade-off: more coordination now, less risk later.
Save this card and confirm the best path with your clinician before changing anything.
Cost, coverage tiers, and prior authorization in 2025
Here’s the money truth: side effects can create “hidden costs.” A fall. A missed week of work for the caregiver. A cancelled follow-up. Even if the medication itself is covered, the downstream cost can be brutal.
In the US, glaucoma drops can land differently depending on Medicare Part D formularies, step therapy, and prior authorization rules. A “preferred” generic can be easy, while a newer branded option may require extra paperwork. The fastest way to reduce delays is to walk in prepared with the exact drug name, the reason for the change, and what’s already been tried. If you’re navigating eligibility questions, high-risk for glaucoma on Medicare can help you understand how “risk” gets framed in coverage conversations.
If diabetes is part of the picture, it’s also worth knowing how Medicare glaucoma screening for diabetics is typically handled, because screening, documentation, and follow-ups can shape the speed of care in real life.
Quote-prep list: what to gather before comparing coverage tiers
- Drop names: brand + generic, plus strength (example: 0.5%)
- Dosing schedule: times/day and which eye
- Side effect timeline: first day noticed + worst day
- Comorbidities: asthma/COPD, slow pulse, arrhythmia, depression, falls
- Coverage details: plan name, deductible status, preferred pharmacy
Neutral next step: Ask your provider for a written medication plan that includes the reason for any switch and the exact dosing.
Save this list and confirm today’s coverage rules on your plan’s official page.
And if you’re trying to make the appointment itself smoother, two practical anchors can help: a simple annual eye exam checklist for seniors and a quick reality check on how often seniors should get dilated eye exams—because missed monitoring is its own kind of risk.
Short Story: The week we finally switched
Short Story: We didn’t switch in one heroic moment. It happened in a slow, awkward week—Monday’s foggy breakfast, Tuesday’s “I’m fine” denial, Wednesday’s near-fall that made my stomach drop. I brought a notebook to the appointment (a printable symptom diary works even better) and felt dramatic doing it. Then the doctor started asking the exact questions my notes answered: when did the dizziness start, how often, any breathing issues, what other meds, what time are the drops used.
For the first time, the symptoms stopped being a vague cloud and became a timeline. The plan changed: technique improved, one medication changed, and we scheduled a pressure check soon—not in six months. That night, we did the new routine quietly, like changing the tempo of a song. The next morning wasn’t perfect, but it was clearer. And clarity, in caregiving, feels like oxygen.
FAQ
Can glaucoma eye drops really affect heart rate in seniors?
Yes, some classes can. Beta-blocker drops are the classic example: they’re applied to the eye but can be absorbed systemically and may lower heart rate in susceptible people. Apply in 60 seconds: take a resting pulse before the morning dose and again 1–2 hours after for two days.
Which glaucoma drops are most likely to cause fatigue or drowsiness?
Some people report fatigue with beta blockers and drowsiness or reduced alertness with alpha agonists such as brimonidine. Individual response varies. Apply in 60 seconds: write “fatigue 0–10” once daily for three days and bring it to your clinician.
What if the drops sting and my parent keeps skipping them?
Stinging can be a medication effect, a preservative effect, or an ocular surface issue. Skipping doses can raise eye pressure, so it’s worth addressing directly. Apply in 60 seconds: ask the clinic about preservative-free options or regimen simplification, and separate multiple drops by 5–10 minutes.
Is it safe to stop glaucoma drops if we suspect side effects?
Don’t stop abruptly without medical guidance unless an emergency is happening. Call the eye clinic, describe the symptoms, and ask for instructions the same day if possible. Apply in 60 seconds: leave a message that includes the exact drop name, last dose time, and the symptom that worries you most.
How can we reduce systemic side effects without switching medications?
Technique matters: gentle eyelid closure and pressing the inner corner of the eye after instillation can reduce drainage into the tear duct and lower systemic exposure. Apply in 60 seconds: set a timer for 60 seconds after each dose and use the inner-corner press consistently.
How do prior authorization and formularies affect a switch in the US?
A new medication may require proof that a preferred option was tried or that side effects occurred. Documentation helps. Apply in 60 seconds: request a written note from the clinic stating the side effect and the reason a change is medically necessary.
Conclusion: your 15-minute next step
Remember my hallway moment—the stumble that made my brain go cold? We didn’t solve it by panicking. We solved it by treating symptoms like data: timing, pulse checks, breathing notes, and a regimen that matched the person, not an ideal patient in a brochure.
Your next step doesn’t need to be dramatic. In the next 15 minutes, do this: write the drop names, dose times, and the first day each scary sign showed up. Then call the clinic and say one clear sentence: “We think the drops may be causing systemic side effects, and we need a medication review.” That sentence saved us weeks of guessing.
Last reviewed December 2025 using patient education from a major ophthalmology organization, medication safety labeling, and clinical safety summaries for common glaucoma drops.