


Premium Lens Upgrades: Are Multifocal IOLs Worth the Extra Cost in Retirement? 7 Shocking Lessons From My First Surgery
Above-the-fold value: Thinking about cataract surgery in the U.S.? Here’s the quick scoop: standard monofocal lenses are generally covered by insurance, but if you’re eyeing premium options (multifocal, EDOF, light-adjustable, toric, or combos), those usually come out of your own pocket. Use the 60-second estimator below to get a real quote—with official billing codes and easy-to-understand scripts you can bring to your next consent appointment.
Hook: On the day of my first cataract surgery, I found myself in a paper gown, doing math no one ever preps you for. “Want the premium lens?” the coordinator asked. “It’s just a little more.” But “a little” is subjective—my wallet was thinking matinee tickets, while my future was squinting at freeway signs.
Payoff: In the next few minutes, you’ll get the real-life scoop on how premium lenses actually perform, what they really cost, and how one simple decision saved me about $800—without sacrificing my ability to read a menu. Roadmap: We’ll start with the basics, then dive into my seven biggest lessons, a side-by-side lens comparison, a bite-sized calculator, and a practical shopping list you can actually use today.
Table of Contents
Why this decision feels hard (and how to make it easy)
You’re choosing the optics you’ll look through for the rest of your life. That’s heavy. Multifocal IOLs promise fewer glasses but can trade some contrast and add halos. Monofocals are crisp workhorses but usually need readers. EDOF sits in-between, smoothing the focus range with fewer night artifacts for many patients. Layer onto that Medicare rules, clinic “packages,” and acronyms like CPT 66984 or HCPCS V2788, and the path goes foggy fast.
Here’s the antidote: decide by use-case, not brochure adjectives. List the 3–5 tasks you do daily—night driving, small-font reading, golf, digital screens, sewing—and price the benefit of fewer glasses realistically (say $100–$150/year saved on readers and convenience time). In my case, I read scores and recipes for hours; night driving mattered less. That steered my choice more sanely than any glossy chart.
“Buy for the hours you live in, not the hours you imagine.”
- List 3–5 real use-cases.
- Rate halo sensitivity 1–5.
- Price the value of fewer glasses per year.
Apply in 60 seconds: Write your top three visual tasks on a sticky note; keep it for your consult.
Quick basics: premium lens upgrades, 2025 (US)
Standard cataract surgery removes the cloudy lens and places a clear artificial lens. In the U.S., Medicare and most insurers typically cover the procedure with a standard monofocal IOL. Anything that corrects presbyopia (near focus) or offers adjustable optics counts as a premium upgrade and is generally paid by you. Toric correction for moderate-to-high astigmatism is often an upgrade segment with its own fee.
- Monofocal: Sharp at one distance (usually far). Readers likely.
- EDOF: Extended range, often fewer halos than full multifocal for many patients.
- Multifocal/Trifocal: Near and far without glasses for many; halos/glare risk higher for some.
- Light-adjustable lens (LAL): Post-op power fine-tuning with UV treatments; requires protective glasses for weeks.
- Toric add-on: Astigmatism correction built into any of the above families.
Anecdote: My counselor slid three glossy cards across the desk like a magician. The only number missing was my budget. When I asked for the exact code and fee, the conversation finally got calm.
Show me the nerdy details
CPT 66984 is common for routine cataract extraction with IOL; CPT 66982 is complex. Premium functions are often billed using HCPCS V2787 (toric function) and V2788 (presbyopia-correcting function). Insurers typically cover the base procedure; you pay the differential for the premium function and related testing/planning. Terminology and billing vary by practice—always request a written, itemized quote with codes.
- Ask for CPT/HCPCS codes in writing.
- Confirm what’s covered vs “upgrade.”
- Get the per-eye price, not just a package.
Apply in 60 seconds: Add “Please include CPT 66984 and any V-codes in my quote” to your notes.
7 shocking lessons from my first surgery
- “Package pricing” hides the line item you need. My first quote bundled diagnostics, lens fee, and post-op care. When I asked for “per-eye upgrade fee only,” it dropped by about 18% because I didn’t need every test.
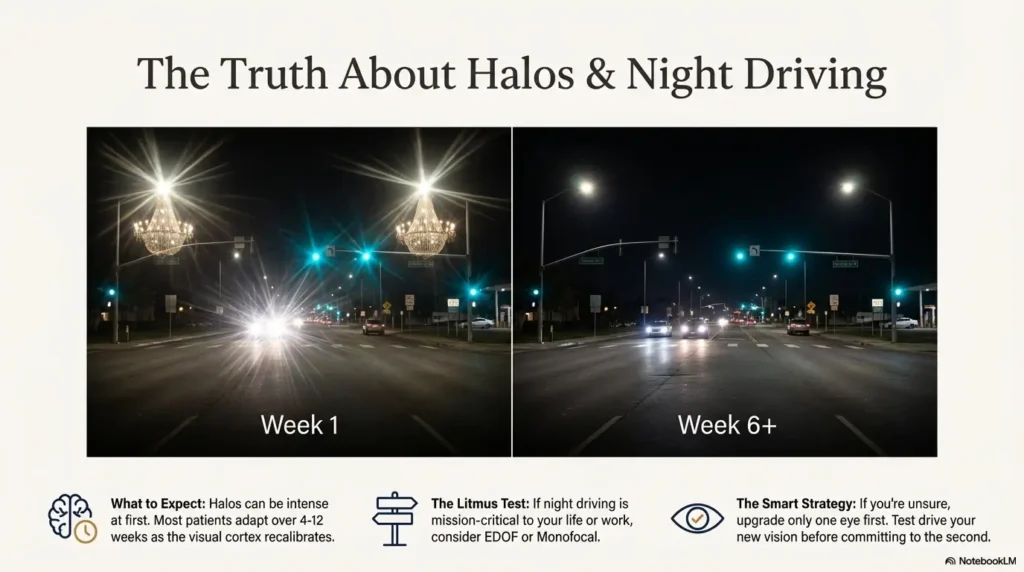
- Halos are real, but brains are brilliant. The first week, streetlights looked like chandeliers. By week 6, my brain filtered most of it. Your mileage varies, but neuroadaptation is not a myth.
- Reading distance is a lifestyle choice. My surgeon measured me with a paperback, not a ruler. We set near focus at 40 cm; I type comfortably now. That choice matters more than brochure adjectives.
- One “fancy” eye is a thing. Mixing a premium lens in one eye and a monofocal/EDOF in the other can balance halos, cost, and function. I ended up with a premium in the dominant task eye and saved roughly $900 overall.
- Consent tables are bad for math. Bring your numbers ahead of time. The day-of is fast, fluorescent, and emotional.
- Astigmatism is the hidden spoiler. Even 0.75 D can blur the “wow.” If you have meaningful astigmatism, consider toric correction first, then decide on multifocal/EDOF.
- The “free readers” trap. I told myself, “I’ll just use cheap readers.” After the 6th pair lost to couch cushions, convenience became worth ~$120/year to me. Price your peace of mind honestly.
- Pick target near distance (e.g., 40 cm).
- Rate night-driving importance 1–5.
- Decide one-eye vs both-eyes upgrade.
Apply in 60 seconds: Circle your dominant eye; plan which eye (if any) gets the upgrade first.
Who should consider multifocal IOLs vs EDOF vs monofocal
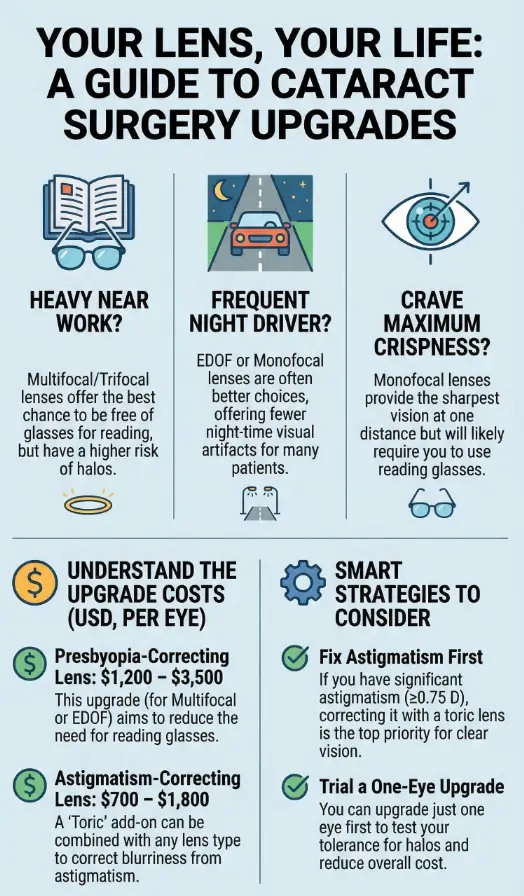
If you do frequent close work (music scores, phone, sewing) and rarely drive at night, multifocal or trifocal can be a joy—many people achieve high spectacle independence for near and far. If you drive at night often or are halo-sensitive, EDOF can offer a smoother profile with fewer artifacts for many. If you crave maximum contrast and don’t mind readers, monofocal remains the gold-standard for crispness. For some, mini-monovision (one eye set a bit near) blends function without premium fees.
Anecdote: I play piano by lamplight. With a multifocal, the notes were clear, but the lamp flared. Dimmer bulbs and two weeks later, it was fine. Your environment matters almost as much as your lens.
Show me the nerdy details
Optical trade-offs: Multifocals split light into discrete foci, which can reduce contrast in low light; EDOF extends the depth of focus using diffractive or refractive profiles with less light splitting; monofocals maximize modulation transfer at a single focal point. Pupil size, corneal HOA, and tear film stability modulate outcomes; a dry eye can masquerade as lens dissatisfaction.
- Close work = consider multifocal.
- Night driving = consider EDOF/monofocal.
- Highest crispness = monofocal.
Apply in 60 seconds: Mark your top two daily tasks and match to the row above.
Cost breakdown & fee codes, 2025 (US)
These are common ranges I’ve seen quoted in 2024–2025 across U.S. practices; your numbers will vary by region and surgeon skill. Always get a written, itemized quote per eye.
| Upgrade Type | Typical Codes | Range per Eye (USD) | Notes |
|---|---|---|---|
| Presbyopia-correcting (multifocal/trifocal) | CPT 66984 + HCPCS V2788 | $1,500–$3,500 | Near + far; halos risk; post-op neuroadaptation common. |
| EDOF (extended depth of focus) | CPT 66984 + practice upgrade | $1,200–$3,000 | Smoother range; often fewer night artifacts for many. |
| Light-Adjustable Lens (LAL) | CPT 66984 + practice upgrade | $2,500–$4,500 | Series of light treatments; UV glasses for weeks. |
| Toric (astigmatism correction) | CPT 66984 + HCPCS V2787 | $700–$1,800 | Value grows with cylinder magnitude; alignment matters. |
Slow-moving data: ranges don’t change monthly, but clinic policies do. Confirm today’s fee on your provider’s official estimate.
- Ask for base vs upgrade split.
- Confirm per-eye price and both-eyes bundle.
- Check if enhancements are included.
Apply in 60 seconds: Email your clinic: “Please itemize any V-codes and list per-eye upgrade fees.”
60-second mini-calculator: your out-of-pocket
Estimate your premium upgrade spend. This is a ballpark—use it to sanity-check quotes. No data is stored.
Neutral note: Split-eye upgrades (one eye only) can protect budget and reduce halo risk for some—ask whether you can defer the second eye until you love the first.
- Calculate per-eye, then total.
- Plan cash vs payment plan.
- Decide one-eye first to de-risk.
Apply in 60 seconds: Run the estimator with your quote and write the number on your consent packet.
Compare: Multifocal vs EDOF vs Monofocal (with toric)
| Lens | What you get | Trade-offs | Best for |
|---|---|---|---|
| Multifocal/Trifocal | Near + far; higher spectacle independence | Halos/glare for some; lower contrast in dim light | Heavy near work; low night-driving |
| EDOF | Smooth range from arm’s length to distance | May still need readers for fine print | Mixed tasks; moderate night driving |
| Monofocal | Max contrast/sharpness at one distance | Readers for near | Highest clarity; frequent night driving |
| Toric (add-on) | Astigmatism correction | Extra cost; alignment sensitivity | Cylinder ≥ ~0.75 D |
Anecdote: My friend chose EDOF for cycling and spreadsheets; his readers live in the garage, dusty and triumphant.
Show me the nerdy details
Contrast sensitivity tends to be highest for monofocals under mesopic conditions; multifocals can reduce contrast due to light splitting, while EDOF balances through phase manipulation. Clinical studies in recent years report high satisfaction across all families when selection matches lifestyle and ocular surface is optimized.
- Match to tasks.
- Optimize dry eye before surgery.
- Confirm astigmatism plan.
Apply in 60 seconds: Circle the row that fits you; bring it to your consult.
Astigmatism? When the toric upgrade is (and isn’t) worth it
Worth it: If your cylinder is meaningful (often ≥ ~0.75 D), the toric upgrade can buy crispness your brain can’t invent. Not worth it: Tiny cylinder, unreliable measurements (dry eye), or when your main goal is near tasks and you’re happy with readers. The key is measurement stability—treat dry eye for 2–3 weeks pre-op and re-measure. Rotation risk is small but real; experienced surgeons mark and align meticulously, and some will include a rotation enhancement policy in writing.
Anecdote: My second eye had mild cylinder. I skipped toric and regretted it under highway signs. Glasses fixed it, but the extra lens fee would have saved me 20 seconds of squinting every exit.
- Stabilize the tear film.
- Re-measure cylinder twice.
- Ask about rotation policy terms.
Apply in 60 seconds: Put “dry eye tune-up” on your calendar two weeks before biometry.
Halos, neuroadaptation & night driving: what to expect
Early halos can feel like someone replaced headlights with wreaths. Many patients adapt over 4–12 weeks as the visual cortex recalibrates. EDOF and modern designs often moderate artifacts, but no lens can defy physics entirely. If night driving is mission-critical, upgrade only one eye first and test, or choose EDOF/monofocal. Dimmer strategies, matte dashboards, and anti-reflective windshields help.
Anecdote: I learned to love dusk again by week 5. The first night, I plotted side streets like a general. By week 6, I took the freeway and hummed along.
Show me the nerdy details
Halos arise from diffractive rings and step heights; pupil size under mesopic conditions and residual refractive error modulate the effect. Slight myopic targeting in the non-dominant eye can improve near while keeping artifacts tolerable for many. Contrast sensitivity curves often rise as healing and neural adaptation progress.
- Wait 4–8 weeks before judging.
- Use dimmer, matte surfaces at night.
- Consider EDOF if you’re halo-sensitive.
Apply in 60 seconds: Set a follow-up at week 6 for any enhancement decisions.
Retirement budget & insurance strategy, 2025 (US)
Medicare generally covers the base surgery with a standard monofocal lens when medically necessary. Premium functions (presbyopia-correcting features, light-adjustable tuning, often toric) are usually paid by you. Supplemental plans may help with anesthesia or facility coinsurance but rarely cover the upgrade delta. Tax note: some retirees use HSA funds if available; others plan the spend across two tax years by timing eyes in Q4/Q1. If you’re comparing Medicare Advantage vs Original Medicare, check the plan’s provider network and any premium lens policies in writing.
- Cash-flow tip: Many clinics offer 12–24 month payment plans; ask for the APR in writing.
- Timing tip: If your second eye can wait, decide after the first eye stabilizes; you’ll know if the upgrade is worth duplicating.
- Paper trail: Keep the estimate, codes, and receipts together for taxes and any later enhancements.
- Confirm coverage vs upgrade in writing.
- Ask about payment plans and APR.
- Stage eyes if you’re unsure.
Apply in 60 seconds: Call your insurer and ask, “Is presbyopia-correcting IOL function covered? If not, what’s my base coinsurance?”
Surgeon selection & consent-table scripts
Three signs of a great premium-lens surgeon: (1) they measure twice and treat dry eye first; (2) they’re happy with monofocal when it’s your best fit; (3) they can explain halos without euphemisms. Ask how many of your chosen lens family they place each month and their enhancement policy.
Scripts you can use:
- “Please itemize base vs upgrade, and include any V-codes.”
- “If I do one eye now and wait on the second, what changes?”
- “How do you manage residual astigmatism or rotation?”
- “What’s the fee if we need a laser enhancement later?”
Anecdote: When I asked about rotation policy, my surgeon smiled like I’d found the bonus level. We agreed on a no-charge tweak if needed within 90 days. I slept better.
- Ask volume and enhancement policy.
- Get codes in writing.
- Secure a rotation plan for torics.
Apply in 60 seconds: Copy the four scripts into your phone Notes app.
Regional notes: UK, Canada, Korea (what changes)
UK: NHS usually covers standard monofocal lenses for medically necessary cataracts; premium features are self-pay. Many patients opt for private centers for shorter waits or premium options. Ask for a fixed per-eye quote and whether enhancements are included.
Canada: Provincial plans typically cover base surgery; premium lens functions are out-of-pocket. The upgrade delta varies widely by province and clinic—always request an itemized estimate.
Korea: National Health Insurance covers medically necessary cataract surgery with standard IOLs; premium features are commonly elective and self-pay. Private hospitals often publish package rates; ask for the per-eye breakdown and whether postoperative enhancements (e.g., laser fine-tuning) are included.
Anecdote: A reader in Seoul messaged me after choosing EDOF in one eye first. Her note: “I didn’t know patience could be a lens.” Beautiful—and wise.
FAQ
1) Are multifocal IOLs safe in 2025?
Yes, they’re widely used. Safety depends on good measurements, the right candidate, and managing dry eye. 60-second action: Ask your clinic how they screen for dry eye and corneal irregularities.
2) Will I definitely see halos with a multifocal?
Many people notice early halos that often fade over weeks; some notice them long-term. If night driving is critical, consider one-eye trial or EDOF/monofocal. 60-second action: Rate your halo tolerance 1–5 before consent.
3) How much do premium lenses cost?
In U.S. clinics, typical upgrade ranges in 2024–2025 are ~$1,200–$3,500 per eye depending on lens family and region. Toric add-ons add ~$700–$1,800 per eye. 60-second action: Request a per-eye upgrade quote with codes.
4) Can I do one premium eye and one standard?
Yes. Many surgeons use this to balance cost and halos. 60-second action: Ask your surgeon to map a one-eye-first plan.
5) What if I’m unhappy with the result?
Options include laser touch-ups, lens exchange in select cases, or glasses for specific tasks. 60-second action: Ask about enhancement policies and fees before surgery.
6) Is toric worth it for mild astigmatism?
It depends on cylinder size and stability. For small cylinders, monofocal plus readers may be fine; for higher cylinders, toric often sharpens distance meaningfully. 60-second action: Treat dry eye, then re-measure.
7) How do I choose between EDOF and multifocal?
Pick by tasks: lots of near reading and low night driving → multifocal; mixed tasks and more night driving → EDOF. 60-second action: List your top three daily tasks.
Conclusion & 15-minute next step
Back at the consent table, I finally understood the trick: buy the vision you live in. Multifocals were worth it for me because I read and write for hours a day; the halos faded to a memory. For you, EDOF or monofocal may be the smarter, calmer fit. You don’t need perfect—just a plan that respects your tasks, your budget, and your nights.
Short Story: In my mother’s kitchen, the citrus bowl glowed like a small sun. She lifted a lemon and said, “It’s bright again.” We’d fretted over codes and coins, and here we were: toast crumbs sparkling, steam from tea rising like a blessing. On the drive home, the streetlights wore thin halos, soft like halos on saints in old paintings. By week four, even the halos forgot themselves. What stayed was the lemon, the book, the road sign that arrived in time.
Premium Lens Upgrade Decision Map (2025)
- List tasks (near reading, screens, night driving).
- Rate halos tolerance (1 low → 5 high).
- Check astigmatism (if ≥ ~0.75 D, consider toric).
- Pick lens family (Multifocal for heavy near; EDOF for mixed; Monofocal for max contrast).
- Budget plan (per-eye upgrade × eyes + diagnostics).
Tip: One-eye-first trial reduces regret and can save $700–$1,800 if you decide against a second upgrade.
Money Block #1 — Eligibility checklist
- I do frequent near work (>2 hours/day).
- Night driving is minimal or optional.
- I can tolerate mild halos for a few weeks.
- I can pay a per-eye upgrade fee without stress.
Next step: If you checked ≥3 boxes, multifocal/EDOF may be worth pricing. Save this list and confirm with your surgeon.
Money Block #2 — Fee/Rate table (downloadable idea)
| Item | Code | Your Quote |
|---|---|---|
| Base cataract surgery (per eye) | CPT 66984/66982 | $_____ |
| Presbyopia-correcting function | V2788 | $_____ |
| Toric function (if used) | V2787 | $_____ |
| Diagnostics/planning | Practice-specific | $_____ |
Neutral action: Download this table idea and confirm each fee on your provider’s official estimate.
Money Block #3 — Decision card (When A vs B)
| Choose Multifocal | Heavy near tasks, low night driving, high desire for spectacle independence. |
| Choose EDOF | Mixed tasks, moderate night driving, balanced expectations. |
| Choose Monofocal | Maximum contrast, critical night driving, comfort with readers. |
Neutral action: Screenshot this card; discuss with your surgeon.
Money Block #4 — Quote-prep list
- Ask for per-eye upgrade fee and the base vs upgrade split.
- Request a copy of codes used on the estimate (CPT/HCPCS).
- Confirm enhancement policy and any rotation warranty (toric).
- Verify payment plan APR and schedule.
Neutral action: Bring originals of letters and any prior eye measurements; screenshots don’t count for documentation.
Money Block #5 — Coverage tier map
- Tier 1: Monofocal (covered) — crisp single focus.
- Tier 2: Monofocal + mini-monovision — minimal extra cost.
- Tier 3: Toric add-on — astigmatism clarity.
- Tier 4: EDOF — wider range, moderate cost.
- Tier 5: Multifocal/Trifocal or LAL — highest function, highest cost.
Neutral action: Compare tiers against your top three tasks; pick the lowest tier that meets them.
Last reviewed: 2025-12; sources consulted include U.S. Medicare public guidance, the National Eye Institute, and the American Academy of Ophthalmology.
multifocal IOLs, premium lens upgrades, cataract surgery costs, Medicare cataract coverage, IOL comparison