


Blurry vision from topiramate doesn’t usually arrive politely.
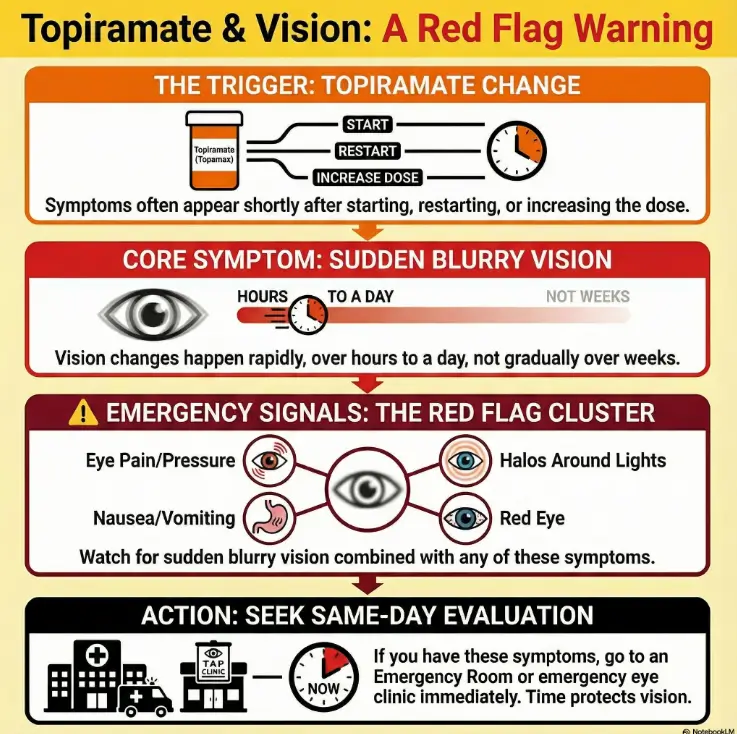
If you started, restarted, or recently increased topiramate (Topamax) and your vision turned fuzzy within hours or a day, it’s easy to mislabel it as screen fatigue and digital eye strain, dry eye, or “just a migraine day.” The problem is that this particular timing can match an uncommon but time-sensitive pattern.
This post helps you decide—fast—whether to go in today, what red-flag clusters matter most, and the exact sentence that gets the right checks (including eye pressure) without sounding dramatic. I’ll keep it practical: a 60-second triage, a plain-English mechanism, and a ready-to-use script.
Read this before you “sleep it off.”
Table of Contents
Safety / Disclaimer (read this first)
This article is general information, not medical advice. Sudden decreased vision—with or without eye pain—can be an emergency. Medication-related eye emergencies are uncommon, but when they happen, the safest move is same-day evaluation (often emergency eye clinic or ER). If you have severe eye pain, halos, nausea/vomiting, or rapidly worsening vision, do not wait for a routine appointment.
- Fast onset matters more than intensity.
- Eye pain + headache can be misleading—treat the vision change as primary.
- Same-day evaluation protects vision.
Apply in 60 seconds: If you’re reading this because symptoms started today, decide your destination (ER or emergency eye clinic) before you decide your theory.
Topiramate blurry vision: the 60-second ER triage
Intent: Decide.
Reader payoff: Know whether to go now or call today in under a minute.
Here’s the truth I wish more medication pages said out loud: the question isn’t “Is it common?” The question is “If this is the rare bad one, what does waiting cost?” With vision, waiting can cost a lot.
Go now: sudden decreased vision ± eye pain/redness (don’t negotiate)
- Vision got blurry quickly (hours to a day), especially in both eyes.
- There’s eye pain, brow pain, or the eye feels “pressurized.”
- You notice halos around lights, foggy vision, or a sudden “my glasses are wrong” feeling.
- You have nausea/vomiting or strong light sensitivity with the vision change.
- Your eye looks red, and the discomfort is escalating.
Call today: milder changes—but new and fast
- New blur that’s clearly different from your baseline and started recently.
- No major pain, but the change is persistent and getting worse.
- You recently started, restarted, or increased topiramate.
Let’s be honest… if it changed overnight, it isn’t “screen fatigue.”
One of my most humbling moments as an adult was realizing how creative I can get when I want to avoid an ER. I once convinced myself a sharp eye ache was “seasonal allergies with ambition.” That’s the brain protecting your schedule, not your eyesight.
- Yes/No: Did the vision change happen within a day?
- Yes/No: Any eye pain, halos, nausea, or redness?
- Yes/No: Did you start/restart/increase topiramate recently?
Apply in 60 seconds: If you answered “yes” to the first plus any other, choose same-day evaluation and bring your medication list.
Acute myopia + secondary angle-closure: what the FDA actually warns about
Intent: Answer.
Reader payoff: Understand the named syndrome and why clinicians treat it like an emergency.
When people say “Topamax can cause eye problems,” it’s usually tossed into a long side-effect soup. But there’s a specific, clinician-recognized pattern associated with topiramate: acute myopia (a sudden shift toward nearsightedness) with secondary angle-closure glaucoma.
The warning in plain English
- Acute myopia: your focus shifts quickly—sometimes you can suddenly see up close better, but distance gets blurry.
- Secondary angle-closure glaucoma: internal eye pressure can rise because fluid can’t drain normally.
This is not the same thing as “I’m due for an eye exam.” It’s a “your anatomy temporarily changed” situation. And that’s why evaluation is time-sensitive.
Core symptom cluster
- Sudden decreased vision
- Eye pain (sometimes with redness)
- Headache/brow ache that doesn’t behave like your usual headache
- Halos/foggy vision
- Nausea/vomiting in the mix
Typical timing: early in the course
Many medication-related eye events show up soon after starting or after a dose change. That timing clue is one reason clinicians take “I started this recently” seriously—when you clearly state it.
Quick personal note: I keep a tiny note in my phone titled “New med start date.” It has saved me more than once, because in a stressful moment your brain drops basic facts like it’s juggling hot potatoes.
Show me the nerdy details
Angle-closure in this context is described as “secondary” because it’s triggered by a medication-related anatomical shift, rather than a long-standing narrow-angle anatomy. Clinicians may talk about a forward shift of structures inside the eye that reduces drainage space, raising pressure. You don’t need to memorize the mechanism to act—timing and symptoms are enough to justify urgent evaluation.
The “migraine vs glaucoma” trap: same head, different emergency
Intent: Troubleshoot.
Reader payoff: Avoid the most common misread that delays care.
If you’re taking topiramate for migraine, you already live with head pain. That’s the trap: when an eye-related emergency produces headache + nausea, your brain may label it “just another migraine.”
Compare table: migraine flare vs eye-emergency signals
Visual tells: halos/foggy vision vs typical patterns
“Halos around lights” isn’t a poetic metaphor—it’s a real, specific symptom people describe when pressure or corneal clarity is affected. If you’re seeing rings and your vision is cloudy, treat that as a data point, not just discomfort.
Body tells: nausea that tracks with eye pain
Nausea alone can be migraine, flu, or life. But nausea paired with a fast vision shift and eye pain is a different constellation. Constellations matter.
Here’s what no one tells you… angle-closure can feel like a migraine that won’t behave.
I’ve watched a friend (a tough, competent person who never complains) keep insisting “it’s just my migraine” while squinting at streetlights like they were exploding. The moment they said “the lights have rings,” everything changed. Words can change care.
- When A: Fast blur + halos/eye pain → choose same-day emergency eye evaluation.
- When B: Familiar migraine pattern without new persistent blur → follow your usual migraine plan, but stay alert.
- Time trade-off: You can lose hours by “waiting to see,” and those hours may matter.
Apply in 60 seconds: Say out loud: “This is new. This is fast. This is vision.” Then act accordingly.
When to seek help: the red-flag clusters that shouldn’t wait
Intent: Checklist.
Reader payoff: A clear “if X + Y, go now” list for patients and caregivers.
Go now: red-flag symptom clusters
- Sudden decreased vision (even if the pain is mild)
- Eye pain or brow pain plus blurred vision
- Halos, foggy vision, or dramatic light sensitivity
- Nausea/vomiting with the vision change
- Red eye plus reduced vision
Call your prescriber today (still urgent, but you’re stable)
- New vision change without severe symptoms
- No major pain, no vomiting, but the blur is persistent
- You recently changed dose, restarted, or started topiramate
If you’re alone: a “get help safely” checklist
- Do not drive if your vision is compromised, especially at night (halos are a warning sign).
- Call a friend, rideshare, or local emergency services if you can’t safely navigate.
- Bring your medication bottles or a screenshot list.
- If you wear contacts, consider removing them if they add discomfort—don’t force it.
Small lived experience: I once tried to “be strong” and walk myself to urgent care with blurred vision. It was 12 minutes that felt like 45. Accept help early. It’s not dramatic; it’s efficient.
“Why me?” The mechanism in plain English (without hand-waving)
Intent: Answer.
Reader payoff: Understand why this can happen even without a glaucoma history.
Most people think glaucoma is a slow, quiet thing that shows up at an annual eye exam. That’s one kind. This is a different kind: a fast pressure problem triggered by a medication-related internal shift.
The short version: anatomy shifts forward → angle narrows → pressure can rise
Inside the eye, fluid drains through a tiny “angle” where structures meet. If internal anatomy shifts forward and crowds that drainage area, pressure can rise. That pressure rise can blur vision and cause pain.
Why it can happen even without prior glaucoma
This isn’t about “you ignored your eye health for years.” It can happen in people with no eye history because it’s triggered, not simply accumulated. (And if you’re someone who tracks risks carefully—like family history of eye disease—this is one of those scenarios where timing beats long-term trends.)
Curiosity gap: why some people get sudden myopia first
Some people notice “I suddenly can’t see far away” or “my prescription feels wrong” before the pain gets intense. That can feel oddly mundane—and that mundanity is the danger. Vision shifts can be the first siren.
Quick anecdote: my cousin once texted me, “I think my glasses are broken.” Turns out, it wasn’t the glasses. It was the timeline. The med change was the clue.
Show me the nerdy details
Clinicians may explain this as a medication-associated change in internal eye structures that reduces the drainage angle and can increase pressure. That’s why eye-pressure checks and a careful front-of-eye exam matter. If you’re evaluated, don’t be surprised if they emphasize “angle” and “pressure” rather than just “dryness.”
Common mistakes that cost time (and sometimes vision)
Intent: Mistakes.
Reader payoff: Stop the delay behaviors that quietly sabotage outcomes.
I’m going to list these with zero judgment because I’ve done versions of them myself. When you’re scared, you become incredibly polite to your own symptoms. Don’t.
Mistake #1: waiting for an optometry refraction appointment
“My glasses must be off” is a normal thought. But if the change is sudden, a routine refraction appointment can be the wrong kind of appointment on the wrong timeline. (If your situation is the slow, routine kind instead, an annual eye exam checklist can help you show up prepared—this post is for the fast, sudden kind.)
Mistake #2: driving yourself when halos/nausea start
Night driving with halos is like playing a video game where the screen glitches right when you need accuracy. If you’re nauseated or in pain, it gets worse. Get a ride.
Mistake #3: changing the medication plan without clinician direction (either way)
Some people keep taking it because they don’t want to “mess up treatment.” Others stop abruptly without calling because they panic. The safer move is: seek urgent evaluation and contact the prescribing clinician as part of that plan.
Personal note: I once stopped a medication on a Friday night and spent the weekend in a Google spiral. It didn’t help my symptoms; it just added anxiety. In emergencies, information is supposed to make you calmer—not noisier.
What to do right now: a script that gets you triaged correctly
Intent: Troubleshoot.
Reader payoff: Say the right words so the visit includes the right checks (especially eye pressure).
In US healthcare, the fastest route to the right evaluation is often the right sentence. Not because clinicians are careless—because triage is a sorting problem, and sorting needs labels.
One sentence that helps triage
“I’m on topiramate (Topamax), and I have sudden blurry vision. I’m worried about acute myopia with secondary angle-closure glaucoma.”
Bring this data (it changes the whole conversation)
- Start date (or restart date)
- Most recent dose change date
- Current dose and formulation (Topamax, generic topiramate, extended-release products)
- All other medications and supplements (a screenshot list is perfect)
- Whether symptoms are in one eye or both
If you’re told “it’s just dry eye”: respectful pushback
Try: “I understand. Because the change was sudden and I’m on topiramate, I’d feel safer if my eye pressure and angle were checked.” Calm, direct, hard to argue with.
Small lived experience: I’ve learned to say “I’d feel safer if…” instead of “You need to…” It keeps the conversation collaborative while still protecting you.
- Count the “red-flag points” below and act on the result.
- It’s not a diagnosis—just a decision nudge.
- Use it to choose urgency, not to self-treat.
Apply in 60 seconds: Run the quick score once, then stop scrolling and follow the next step it suggests.
Mini calculator: “Urgency score” (0–5)
Neutral next step: If the result says “same-day,” choose your destination and bring your medication list.
What clinicians may do (so you’re not blindsided)
Intent: Answer.
Reader payoff: Know what tests and decisions commonly happen in the first hour.
Emergency care is less scary when you can picture the steps. Here’s the usual rhythm—no promises, just the common playbook.
Checks: eye pressure and an exam of the front of the eye
- Visual acuity test (how well you can see)
- Pressure measurement
- Front-of-eye evaluation to assess the drainage angle area
- Assessment of redness, corneal clarity, pupil response
Immediate goal: reduce pressure and address the trigger pathway
Treatment decisions depend on what the exam shows. The point is: this is solvable faster when it’s recognized faster. (If you end up leaving with drops and a plan, it can help to know what glaucoma eye drops side effects can feel like—so you don’t mistake expected irritation for “something is wrong” or, just as dangerous, ignore a true change.)
Curiosity gap: how fast does vision improve?
Many people want a number. The honest answer is: it varies, and it depends on how quickly you’re evaluated and what the findings are. Your job is not to predict the timeline—your job is to shorten it by getting assessed promptly.
Personal note: I used to think going to the ER was “failing at coping.” Now I see it as hiring the right tool for the job. A fire extinguisher doesn’t mean you’re dramatic; it means you’re practical.
Show me the nerdy details
Clinicians may describe the situation as a medication-associated angle problem rather than primary glaucoma. That distinction can shape what treatments they choose and how they think about whether symptoms will resolve. If you hear terms like “secondary angle closure” or “acute myopic shift,” it’s essentially a shorthand for “this is tied to the medication and happened quickly.”
Who this is for / not for (so you don’t misapply the advice)
Intent: Decide.
Reader payoff: Know whether this guidance fits your situation or whether another path makes more sense.
For: recently started, restarted, or recently increased dose
If your symptoms started soon after a start/restart/dose increase, this page is for you. Timing is a legitimate clinical clue.
For: Topamax + extended-release forms + combo products
People encounter topiramate as brand Topamax, generic topiramate, and extended-release forms. Some people also see it in combination therapy contexts (for example, weight-related prescribing). The shared issue is the active ingredient and the timeline of change.
Not for: gradual months-long blur from stable refractive change/cataract
If your blur has crept in over months and you have no rapid change, this post is less relevant. You still deserve care—just a different urgency scale. (If you’re sorting out slow-change causes, starting with early cataract signs and a broader view of age-related eye diseases after 60 can help you ask better questions at a routine visit.)
Not for: trauma or chemical exposure
If something hit your eye or a chemical splashed, skip this logic and follow eye-injury emergency guidance immediately.
Small lived experience: I once tried to fit my symptoms into the “most likely” category because it felt comforting. It was the wrong instinct. The right instinct is: match urgency to the timeline and red flags, not to what feels emotionally convenient.
Next step: one concrete action
Intent: Decide.
Reader payoff: A single safe instruction that reduces delay.
If symptoms are sudden or severe: choose same-day evaluation (ER or emergency eye clinic). Use this one sentence at check-in:
“I’m on topiramate (Topamax) and I have sudden blurry vision. I’m worried about acute myopia with secondary angle-closure glaucoma.”
If symptoms are mild but new and fast, call your prescriber today and ask what they want you to do right now—and be ready to go in if symptoms worsen.
Infographic: the 3-step “Don’t-Delay” Flow
Step 1: Name it
“Sudden blurry vision on topiramate.”
Why it helps: triage needs a label.
Step 2: Check flags
Pain? Halos? Nausea? Redness? Fast onset?
Why it helps: clusters beat guesswork.
Step 3: Act today
Same-day evaluation if sudden/severe.
Why it helps: time protects vision.
Neutral next step: If you’re unsure, choose the safer path and get evaluated.
Short Story: A “normal side effect” that wasn’t (120–180 words) …
My friend started topiramate for migraines after a brutal month of missed work. The first week was mostly manageable—tingly fingers, a little appetite change, the usual “new med weirdness.” Then one evening, streetlights looked like they had glowing rings. She laughed it off and said, “Cute, my brain installed Instagram filters.” Ten minutes later she was nauseated, and her vision felt like someone rubbed petroleum jelly on her glasses.
She didn’t want to go in. It was late. She didn’t want to be “that person.” I asked one question: “Is this your normal migraine pattern?” She went quiet. That’s the sound of recognition. We went in. The visit wasn’t fun—but it was decisive. The next day she said the weirdest part was how close she came to waiting, simply because waiting would have been easier socially. “I’m glad you didn’t let me be polite,” she told me.
FAQ
Can Topamax cause sudden blurry vision even if I never had glaucoma?
Yes. Medication-related angle-closure patterns can occur even in people without a prior glaucoma diagnosis. The key clue is often sudden onset after starting or changing the medication.
How quickly can topiramate trigger angle-closure after starting?
When it happens, it’s often in the earlier phase of treatment (or after a restart/dose change). If your symptoms began soon after a change, that timing is worth stating clearly during triage.
What does “halos around lights” mean—and why is it a red flag?
People describe halos as rings or glare around lights, especially at night. In the context of sudden blur and eye discomfort, halos can signal an eye problem that deserves urgent evaluation.
Is topiramate blurry vision the same as dry eye or eye strain?
Sometimes eyes can feel dry on many medications, and screens can cause blur. The difference is the speed and the cluster. Overnight blur, halos, pain, redness, or nausea pushes you toward urgent care rather than “try drops and rest.” (If you’re sorting everyday dryness triggers separately, antihistamines can matter—see Claritin vs Zyrtec vs Allegra for dry eye—but that’s not a substitute for urgent evaluation when the timeline is sudden.)
Should I stop topiramate if my vision suddenly changes?
Don’t try to manage this alone. If the change is sudden or severe, get same-day evaluation and contact the prescribing clinician. In urgent medication safety scenarios, clinicians often want to know immediately and may advise changes based on your exam and risk profile.
ER vs urgent care vs eye doctor—where should I go first?
If symptoms are sudden, severe, or include pain/halos/nausea, the safest route is an ER or emergency eye clinic that can check eye pressure and evaluate urgently. Routine optometry is often not the right first stop for rapid symptom clusters.
Can this happen with generic topiramate or extended-release products?
Yes, because the active ingredient is the same. If you’re on an extended-release form, mention the exact product name and dose so your care team has the full context.
What should I tell triage so they check eye pressure promptly?
Use a direct, calm sentence: “I’m on topiramate (Topamax) and I have sudden blurry vision. I’m worried about acute myopia with secondary angle-closure glaucoma.”
Will my eyesight go back to normal after this is treated?
Outcomes vary based on how quickly you’re evaluated and what the exam shows. The most actionable truth is: earlier evaluation improves the odds of a better outcome.
Can this present as “sudden nearsightedness” without much pain?
It can. Sudden changes in prescription feeling—especially if fast and unusual—are worth taking seriously when paired with recent topiramate changes.

A calm, practical “before you go” list (no drama, just speed)
When you’re heading in for urgent evaluation, you don’t need more information—you need fewer obstacles.
- Bring: medication bottles or a phone list (dose + start date + last change)
- Bring: a companion if your vision is compromised
- Say: the triage script once, clearly
- Ask: “Can you check my eye pressure and evaluate for angle-closure?”
- Note: when symptoms started (time matters)
Neutral next step: Pack the basics, send one text asking for a ride, and go.
Conclusion
Remember the bargain your brain tries to make—“maybe it’s nothing”? Here’s the gentler, truer replacement: maybe it’s something treatable, and time helps. Topiramate-related severe eye events are not everyday occurrences, but sudden blurry vision with red flags is an everyday reason to seek urgent evaluation. You don’t have to diagnose yourself. You only have to choose the safer lane.
Your 15-minute CTA: If symptoms began today, use the one-sentence script, grab your med list, and go to same-day evaluation. If symptoms are milder but new and fast, call your prescriber today and describe the timeline clearly—then follow the plan you’re given.
Last reviewed: 2025-12-26