

In the next six months, proliferative diabetic retinopathy can demand 2 retina visits—or 10.
That’s why PRP laser vs anti-VEGF injections for PDR isn’t really “laser vs shots.” It’s durability vs follow-up burden, and how much your eyes can afford real life.
PDR (proliferative diabetic retinopathy) is an advanced stage of diabetic retinopathy where abnormal new blood vessels grow on the retina. Those vessels can bleed (vitreous hemorrhage) and, in some cases, pull on the retina, raising the stakes when treatment or monitoring gets interrupted.
Keep guessing, and the cost isn’t just money—it can be a sudden step backward in vision that’s harder to recover from.
This guide helps you choose a plan you can actually complete: factoring in diabetic macular edema (DME) symptoms, visual field/night-driving tradeoffs, and what happens when a visit slips. It’s built around the same real-world triage points clinics quietly use: schedule reliability, macula status, and urgency risk.
Table of Contents
Decide first: the 90-second plan you can’t “Google” for you
If you only read one section, make it this one. Most articles start with studies. Real life starts with your calendar, your macula, and whether your retina team can reach you when things change.
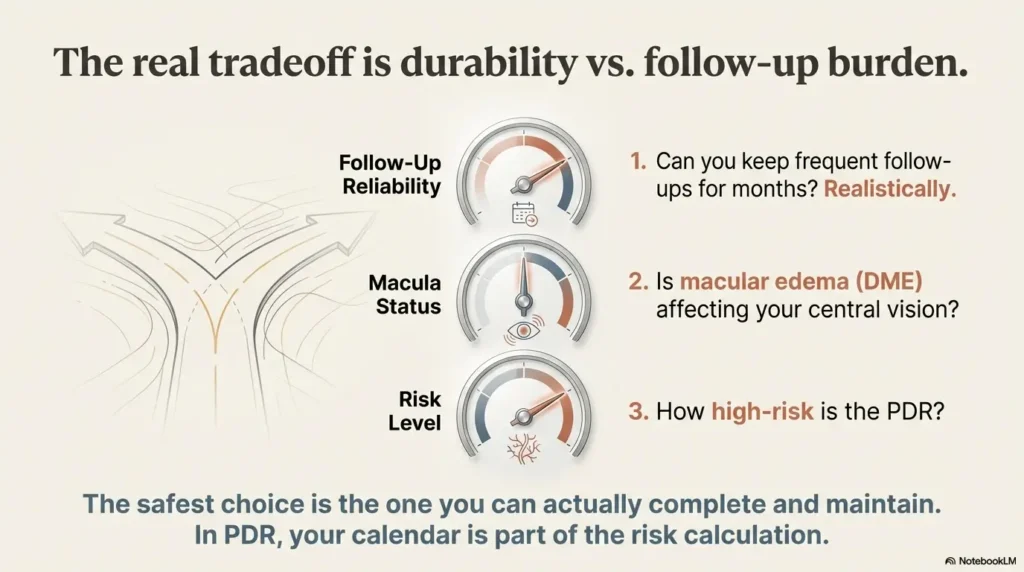
The 3 questions retina clinics silently triage by (and why)
- Can you keep frequent follow-ups for months? Not “I hope so.” Actually, realistically.
- Is DME (swelling) affecting central vision? If yes, injections often become the anchor.
- Is there high-risk PDR or traction concerns? The urgency and sequencing can shift.
Here’s what no one tells you… your calendar can change your risk curve
I’ve seen this play out in the most boring way possible: someone chooses the “best” therapy on paper, then their life does what life does—work travel, caregiving, a car that refuses to start—and suddenly follow-up becomes the treatment. In PDR, time and consistency aren’t just logistics; they’re part of the risk calculation.
Open loop: what “good adherence” actually means in PDR care
“Monthly” rarely stays monthly. Early on, injections can be frequent, then gradually spaced out if the retina stays quiet. But that “quiet” needs monitoring. When you ask, “How often will I need shots?” the better question is: “What’s the minimum visit schedule you consider safe for me?”
- If follow-up is fragile, durability matters more.
- If DME is present, central vision often drives the plan.
- If traction risk is high, sequencing becomes urgent.
Apply in 60 seconds: Write down your “realistic monthly visit capacity” (0–4) before you discuss options.
- You might miss visits due to work/transport/caregiving.
- You want a more “durable” baseline plan.
- You’re okay discussing field/night-vision tradeoffs.
- You can reliably keep frequent follow-ups.
- DME is affecting central vision or imaging suggests it.
- You want to prioritize field preservation if possible.
- You need fast control now, plus long-term durability.
- Your schedule is “mostly” reliable, not perfect.
- Your retina specialist wants sequencing flexibility.
Neutral next action: Bring this card to your appointment and circle the box that matches your life.
Who this is for / not for (avoid the wrong comparison)
PDR isn’t one uniform problem. And you aren’t one uniform patient. The smartest comparison starts by narrowing which bucket you’re actually in.
PRP-leaning scenarios: durability-first when follow-up is fragile
- You live far from retina care, rely on rides, or your schedule shifts weekly.
- You’ve already had missed appointments for non-medical reasons (it happens).
- You want a plan that still holds if life punches the calendar.
Anti-VEGF-leaning scenarios: frequent monitoring is realistic
- You can reliably attend frequent visits for months.
- You have DME or central vision symptoms that need attention.
- Your care team expects close imaging follow-up (OCT, sometimes angiography).
Not-ideal without special planning: one-eye vision, transportation barriers, unstable systemic health
If one eye carries most of your daily function, the margin for error shrinks. Same if you’re balancing dialysis schedules, unstable blood sugar, or caregiving. This doesn’t mean you “can’t” do any option. It means your plan should include explicit fail-safes: backup rides, backup clinic, and a clear “if I miss two visits…” pathway.
Quick self-check: If you can’t confidently commit to follow-ups, say that out loud in the visit. It’s not embarrassing. It’s crucial data.
Follow-up burden: what your next 6 months actually look like
“Follow-up burden” sounds like jargon until you translate it into real life: hours off work, ride coordination, copays, waiting rooms, dilation, imaging, and the mental load of never quite being “done.”
PRP visit pattern: sessions, completion, and what “done” really means
PRP is often delivered in one or more sessions. “Done” usually means the laser treatment is complete and the retina is stable enough that visits can space out. It doesn’t mean you never need monitoring again. It means the plan tends to have a more durable baseline if adherence becomes uneven.
Anti-VEGF visit pattern: injections, OCT/FA checks, and why tapering is tricky
Injections are a rhythm: treat, reassess, adjust. Modern retina practice often uses OCT imaging to track swelling and response. The tricky part is tapering. When treatment is reduced, some eyes stay stable. Some don’t. That’s why the follow-up schedule isn’t just tradition—it’s a safety mechanism. (If you want a concrete reference point for how “injection rhythm” can look over time, compare it to a real-world anti-VEGF injection schedule—the details differ by disease, but the continuity principle is the same.)
Curiosity gap: “What happens if I miss 8 weeks?” (ask this before choosing)
This single question forces the plan into reality. If your clinic can answer clearly—Plan A, Plan B, what counts as urgent—you’re in a better place than most people reading generic comparison charts.
Show me the nerdy details
PRP reduces retinal oxygen demand by treating peripheral retina, which helps decrease the stimulus for abnormal new vessel growth. Anti-VEGF medications target vascular endothelial growth factor pathways that drive neovascularization. The practical difference is durability: PRP’s effect persists after sessions are complete, while anti-VEGF requires ongoing dosing to maintain suppression in many cases.
Pick conservative numbers. This is not medical advice—just scheduling math.
Estimated total retina visits in 6 months: (click calculate)
Neutral next action: If the number feels impossible, discuss a more durable plan and a backup pathway.
When she finally returned, she wasn’t “starting over,” but she wasn’t where she’d been. Her retina specialist didn’t scold her. He rewrote the plan. They used injections to calm the eye down again, then added PRP so the baseline would hold even when life didn’t. “We’re building a plan that survives your real life,” he said. That sentence changed how she felt walking out.
Lost-to-follow-up risk: the mistake that can erase progress
This is the section people skim because it feels like a lecture. Please don’t. The lost-to-follow-up problem isn’t about character. It’s about how PDR behaves when treatment is interrupted.
Why injection-only can be unforgiving when life interrupts
Anti-VEGF works while it’s being administered and monitored. When follow-up breaks down, you can lose the ability to catch reactivation early. That’s the blunt truth behind the “you must keep appointments” message. It’s not drama. It’s risk management.
PRP’s durability advantage when consistency is uncertain (what it does and doesn’t guarantee)
PRP can provide a more stable baseline after it’s completed. It doesn’t guarantee nothing will ever worsen. Diabetes is a long game. But it can reduce your dependence on perfect visit timing, which matters if you’re time-poor, working hourly, or caring for someone else.
Let’s be honest… “I’ll definitely make every visit” is not a plan
I’ve written reminder systems for everything from dental cleanings to IRS deadlines, and here’s what I’ve learned: intentions are fragile. Systems are stronger. If you choose injections, build a system: calendar blocks, ride backups, and a clinic contact plan for rescheduling fast. (If the idea of “first injection logistics” feels heavy, you may relate to what to expect at your first anti-VEGF injection appointment—again, different condition, same human fear.)
- Injection strategies often require tighter continuity.
- PRP may offer more durability if life gets chaotic.
- Hybrid plans can bridge “control now” and “durability later.”
Apply in 60 seconds: Ask your clinic: “What’s your Plan B if I miss two visits?”
Field vision & night driving: the tradeoff patients notice at 9 PM
Visual acuity charts are bright, high-contrast, and polite. Real life is none of those things. Field vision, contrast, and glare show up when you’re navigating dim parking lots, rain-slick roads, and the “why does this aisle feel like a maze?” moments.
PRP and peripheral sensitivity: what “field” changes can feel like
- Curb confidence: stepping off a curb feels slightly less automatic.
- Crowd navigation: you notice people “appearing” from the side sooner than you’d like.
- Stairs in dim light: you become more cautious—sometimes wisely, sometimes annoyingly.
Not everyone experiences these changes the same way. But if you drive at night, work in low light, or already feel your vision is “soft” around the edges, you should bring that into the decision.
Night vision, glare, contrast: the after-dark complaints you should name up front
Some people describe it as headlights blooming. Others say it’s not the lights—it’s the in-between: shadows, contrast, that moment when your brain is filling in missing information. The right move is not to panic, but to ask for baseline testing and discuss what changes would matter most for your daily life.
Open loop: which vision test to ask for before and after treatment (and why)
Ask about visual field testing and whether your clinic tracks functional symptoms over time. A quick “Do you monitor fields or contrast complaints?” can turn a generic plan into a tailored one.
- PRP can carry more field/night-vision risk for some patients.
- Injections may preserve field in some cases, but continuity matters.
- Testing + symptom tracking turns fear into data.
Apply in 60 seconds: Write down two “low-light tasks” you need to protect (driving, stairs, work) before your visit.
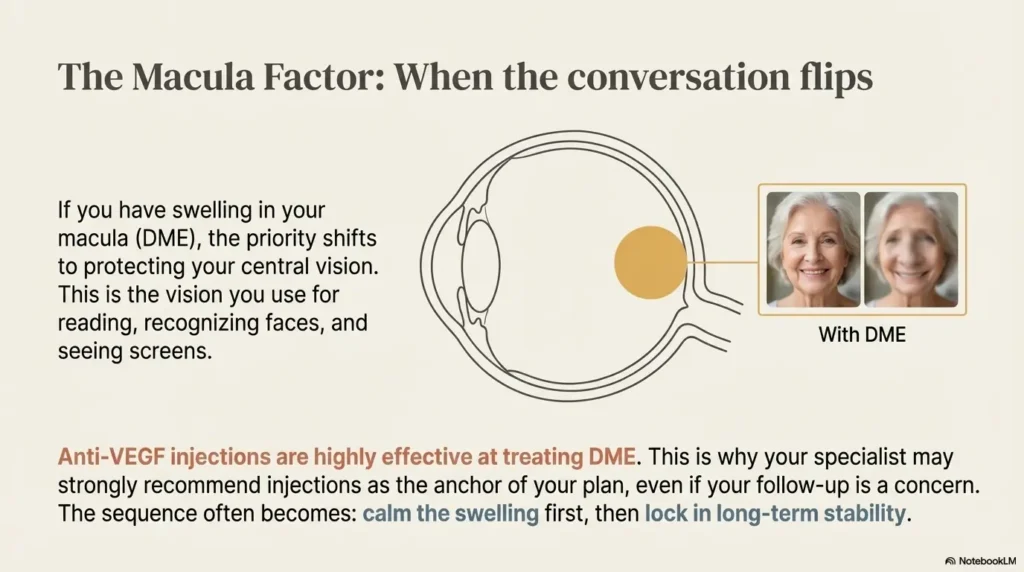
Macula factor (DME): when the comparison flips
If the macula is involved, the conversation changes. Not because PRP “doesn’t work,” but because central vision is precious and swelling can change priorities.
When anti-VEGF becomes the anchor because central vision is on the line
Anti-VEGF therapy is widely used in diabetic eye disease, including situations where swelling affects central vision. This is one reason your retina specialist may emphasize injections even if you came in convinced you want “the laser.” Central vision often drives function: reading, faces, screens, medication labels—the stuff that keeps you independent. (If you’re trying to map your symptoms to what your doctor is seeing, start with a clear DME symptom guide before you get lost in laser-vs-shot debates.)
PRP timing when swelling exists: why sequencing matters
Clinicians often think in sequences: stabilize swelling, control neovascularization, then consolidate durability. This is where hybrid strategies show up—less as ideology, more as practical craftsmanship.
Curiosity gap: two people both “have PDR”—why one gets laser first and the other doesn’t
Because “PDR” is a label, not a full story. Your imaging, swelling status, hemorrhage history, and traction risk add chapters. This is why a one-size-fits-all recommendation online can feel oddly confident and strangely useless.
Show me the nerdy details
OCT (optical coherence tomography) helps clinicians measure retinal thickness patterns that suggest edema and track response to therapy over time. DME can influence treatment sequencing because therapies aimed at neovascularization and therapies aimed at edema may overlap, but the timing can matter for symptoms and monitoring.
- Yes/No: I can reliably attend retina visits as often as my clinic recommends for at least 3 months.
- Yes/No: I have a backup ride plan if my primary option fails.
- Yes/No: I can reschedule within 7–10 days if something comes up.
- Yes/No: I understand what symptoms trigger an urgent call.
Neutral next action: If you answered “No” to two or more, discuss durability-focused or hybrid plans.
Combination therapy: the “both/and” plan many clinics default to
Online debates love binary choices. Clinics love outcomes. Hybrid strategies exist because they solve real problems: rapid control when the eye is active and long-term durability when life is unpredictable.
Stabilize then lock-in: injections to quiet activity → PRP for long-term stability
A common real-world pattern is: injections first to calm active neovascularization (and possibly help DME), then PRP to reduce the risk that everything hinges on perfect follow-up forever. It’s not “giving up on injections.” It’s building resilience into the plan. (For readers wondering about coverage details for the medication side of this plan, see how Medicare coverage can work for Eylea injections.)
Rescue pathways: what it signals when your plan switches mid-year
Switching doesn’t automatically mean failure. Sometimes it means your retina changed. Sometimes it means your life changed. I’ve heard readers describe the switch as a relief: “I stopped feeling like one missed appointment would ruin everything.” That emotional load matters. Stress doesn’t treat PDR. But stress can sabotage adherence.
The “minimum viable follow-up” question to ask your retina team
Try this phrasing: “What follow-up schedule is the minimum you consider safe for me, and what’s our fallback if I can’t meet it?” It’s respectful. It’s clear. And it forces a plan you can execute.
Show me the nerdy details
In landmark clinical research, anti-VEGF regimens have shown strong outcomes compared with PRP in many patients, while PRP remains an established, durable therapy. Clinicians often tailor combination approaches based on disease activity, imaging, and adherence risk rather than treating therapies as mutually exclusive.
Common mistakes: regret-proofing your treatment choice
Here’s the part where we prevent the most common “I wish someone had told me” moments. None of these mistakes make you a bad patient. They’re predictable. That’s why they’re preventable.
Mistake #1: choosing injections while underestimating adherence reality
The most common mismatch is not medical—it’s logistical. People say yes to injections while quietly thinking, “I’ll figure it out.” If you’re time-poor, you need a concrete system on day one: rides, reminders, and rescheduling rules.
Mistake #2: treating PRP as “one quick laser” and skipping post-laser checks
PRP can feel like a checkbox. It isn’t. Post-laser monitoring matters, especially early. Don’t let the “procedure completed” feeling trick you into skipping the follow-up that confirms stability.
Mistake #3: tapering injections too casually (why worsening can be faster than expected)
Even when things look stable, spacing visits should be deliberate. This is where experienced retina teams differ from a simplistic online schedule. If you’re spacing out, ask what signs would trigger stepping back in.
Mistake #4: never asking for a written Plan A / Plan B
Verbal plans evaporate the moment you hit the parking lot. A written plan is not “being difficult.” It’s being safe.
- Match treatment to your follow-up reality.
- Don’t skip the confirmation visits after PRP.
- Ask for a written Plan A / Plan B with triggers.
Apply in 60 seconds: Text yourself the four mistakes above and circle the one you’re most likely to make.
Safety & urgent symptoms: when to call now (not later)
If you’re anxious reading this section, I get it. The goal isn’t fear. It’s clarity. In diabetic eye disease, delays can matter, and the symptoms can be easy to rationalize away— the same trap described in “is it just getting older?” red-flag eye symptoms.
PRP: expected short-term effects vs warning signs
- Often expected: temporary blur, mild irritation, light sensitivity, a “worked-on” feeling.
- Call urgently: sudden major vision drop, curtain/shadow, severe pain, persistent vomiting/nausea, rapidly increasing floaters.
Injections: common irritation vs rare but serious infection concern
- Often expected: scratchy sensation, mild redness, small surface irritation.
- Urgent red flags: significant pain, worsening redness, light sensitivity with decreased vision, thick discharge, feverish feeling.
When to seek help: sudden vision loss, curtain/shadow, flashes/floaters surge, severe pain
If your vision suddenly changes, don’t negotiate with yourself. Call your retina clinic’s emergency line or seek urgent ophthalmic care. “I’ll wait until tomorrow” is a tempting thought—especially if you’re exhausted. In this category, it’s often the wrong one.
Red flags that deserve urgent evaluation: a new curtain or shadow, sudden vision drop, a surge of floaters/flashes, severe eye pain, marked light sensitivity with vision change, or symptoms that worsen hour by hour.
US cost & logistics: the hidden compounding effect of repeat care
Let’s talk about what people whisper about in waiting rooms: cost, time off work, parking fees, and prior authorizations. The US system can turn “more visits” into a meaningful burden—even when each visit is medically appropriate.
The cost drivers that matter: frequency, site-of-care, and imaging add-ons
- Frequency: repeated injections can create repeated copays/coinsurance.
- Site of care: office vs hospital outpatient settings can change billing.
- Imaging: OCT and other tests may be billed as separate line items.
Prior auth rhythm: how delays can quietly disrupt continuity (and what to ask staff)
Prior authorizations can introduce pauses. If you’re on an injection plan, ask staff: “How do you handle authorization renewals so visits don’t get delayed?” That’s not being nosy—it’s protecting continuity.
Loss-prevention: avoiding surprise bills by requesting a written estimate and coding clarity
One simple tactic: ask for a written estimate for the next step and what the billing category is (office procedure, imaging, medication administration). You don’t need to become an insurance expert. You just need fewer surprises. (If you want a baseline number for planning, start with what Medicare patients often pay for a diabetic eye exam, then ask your clinic how injections/laser are billed in your specific setting.)
Show me the nerdy details
In the US, biologic medications administered in clinic may involve separate charges for the drug, administration, and associated imaging/visits. Insurance policies vary widely, and site-of-care differences can affect patient responsibility. Asking for a “what gets billed on a typical injection visit?” breakdown can clarify expectations.
- Frequency matters as much as procedure type.
- Ask about prior auth timing before it becomes a delay.
- Get a written estimate to reduce surprise bills.
Apply in 60 seconds: Call your insurer or clinic billing desk and ask, “What do patients typically owe for an injection visit vs laser session?”
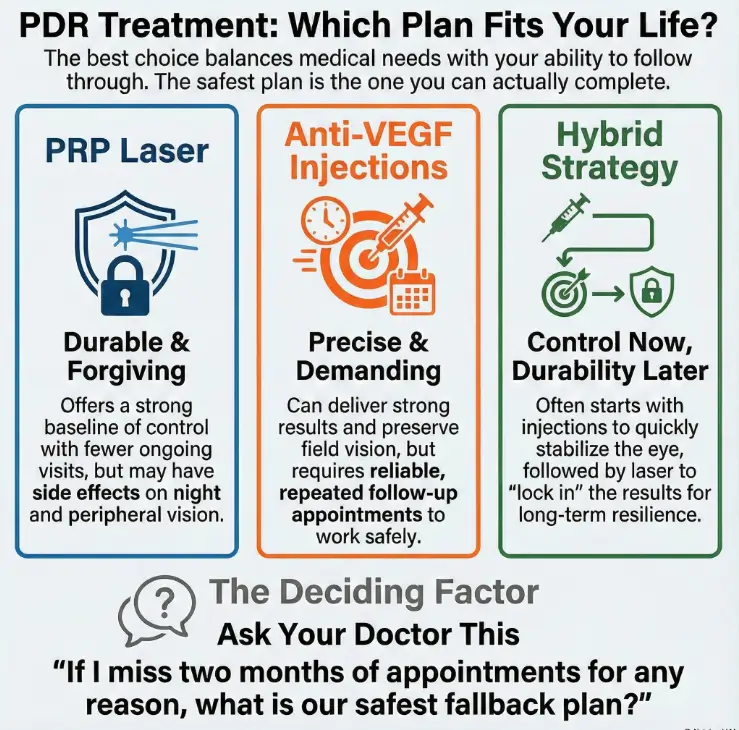
- Durability: often stronger baseline after completion
- Visit burden: typically fewer ongoing visits
- Tradeoff: possible field/night-vision impact
- Best when: follow-up reliability is uncertain
- Control: strong outcomes with close monitoring
- Visit burden: requires repeated follow-ups
- Upside: may help preserve field in some cases
- Best when: adherence is reliable; DME may be present
- Stabilize: injections to quiet active disease
- Lock in: PRP for durability if life disrupts visits
- Reality: flexible sequencing based on response
- Best when: you want both control and resilience
How to use this: Pick the column that matches your life this season, not your best intentions.
Next step: one concrete action (do this today)
If you do nothing else after reading, do this: go into your next retina visit with a script that forces a real-world plan. It will feel awkward for 10 seconds. Then it will feel like relief.
The 60-second script: “If I miss 2 months, what’s the safest fallback plan?”
You can say it exactly like that. Then pause. Let them answer fully. If the answer is vague, ask: “Can we put Plan A and Plan B in writing?”
Ask for Plan A / Plan B in writing (dates + triggers + who to call)
- Plan A: what you do if visits go smoothly
- Plan B: what you do if you miss or must delay care
- Triggers: symptoms that require a same-day call
If choosing injections: set up a no-miss system (rides, reminders, backup clinic)
My favorite low-tech trick: set two reminders—one 7 days before, one 24 hours before—and write “backup ride” in the 7-day reminder. Because “I’ll figure it out” is where plans go to die.
FAQ
Is PRP laser permanent, or can PDR come back?
PRP’s effect is durable once completed, but diabetes is ongoing. Retinopathy can still progress, especially if blood sugar and blood pressure remain unstable. Think “strong baseline,” not “one-and-forever guarantee.” (If blood pressure control has been a moving target, it’s worth understanding how the retina can reflect it in hypertensive retinopathy.)
Are anti-VEGF injections “better” than PRP for PDR?
“Better” depends on the outcome you prioritize and what you can consistently do. Clinical research has shown strong outcomes with anti-VEGF regimens in many patients, and PRP remains an established treatment with durability. In the real world, follow-up reliability often decides what’s safest.
How often are anti-VEGF injections needed for PDR in real life?
It varies widely. Some people need frequent dosing early on, then spacing if the retina stays quiet. Others need ongoing treatment at closer intervals. Ask your retina specialist for a “minimum safe schedule” and a backup plan if you miss visits.
What happens if I miss an injection appointment for PDR?
Missing one appointment doesn’t automatically mean disaster, but it can increase risk—especially if missed time becomes a pattern. Call the clinic, reschedule as soon as possible, and ask whether symptoms or changes in vision require urgent evaluation.
Will PRP ruin my peripheral vision or night driving?
Not “ruin” for everyone, but PRP can affect peripheral sensitivity and night vision for some people. If night driving, low-light work, or balance in dim environments is important to you, bring that up explicitly and ask about baseline field testing.
Can PRP worsen macular edema (DME)?
In some patients, swelling can fluctuate during treatment. That’s one reason clinicians may sequence therapies—using injections to stabilize swelling or monitoring OCT closely. This is a personalized decision based on your imaging and symptoms.
Is combination therapy (PRP + anti-VEGF) common?
Yes—often because it addresses both immediate control and long-term durability. Injections can quiet active neovascularization, and PRP can help reduce reliance on perfect follow-up forever. Your team’s sequencing reflects your eye’s activity and your practical constraints.
Does Medicare cover PRP and anti-VEGF injections for diabetic retinopathy?
Coverage depends on your specific plan and setting. Medicare and many insurers generally cover medically necessary retinal treatments, but out-of-pocket costs can vary based on deductibles, coinsurance, drug coverage, and whether care is billed in an office or hospital outpatient setting.
How do I know if it’s vitreous hemorrhage vs “normal floaters”?
New floaters can happen for many reasons, but a sudden shower of floaters, a haze that looks like smoke, or a rapid drop in clarity can be concerning. If the change is sudden or worsening, call your retina clinic urgently.
Should I stop blood thinners before injections or laser?
Don’t stop prescribed blood thinners without guidance from the clinician who prescribed them. Tell your retina specialist what you take. They’ll weigh bleeding risk, clot risk, and the specifics of your procedure.
Conclusion
Let’s close the loop from the hook: the “right” choice isn’t the one that wins an internet argument. It’s the one that still works when you’re tired, busy, and human. PRP laser tends to offer more durability with fewer ongoing visits, with potential field/night-vision tradeoffs. Anti-VEGF injections can deliver strong outcomes—especially when DME is part of the picture—but the plan lives or dies by follow-up. And in real clinics, a hybrid approach often exists for one reason: it survives reality.
Your next 15-minute move: open your calendar and your phone. Put your next retina appointment date in, add two reminders (7 days and 24 hours), and write one sentence to bring to the visit: “If I miss two months, what is our safest fallback plan?” (If you’re building an eye-care routine around multiple risks, it can help to pair this with an annual eye exam checklist for seniors and a realistic plan for how often to get dilated eye exams.)
Last reviewed: 2025-12-27