


Navigating the Invisible: A Guide to Hemianopia
The first warning sign may be small enough to miss: peas untouched on one side of the plate, the same shoulder brushing the same doorway, a glass knocked over from the “invisible” edge of the table.
Hemianopia after stroke can turn familiar rooms into uneven terrain. Families often see missed food, doorway bumps, spills, poor scanning, and sudden frustration before they know what to call the problem.
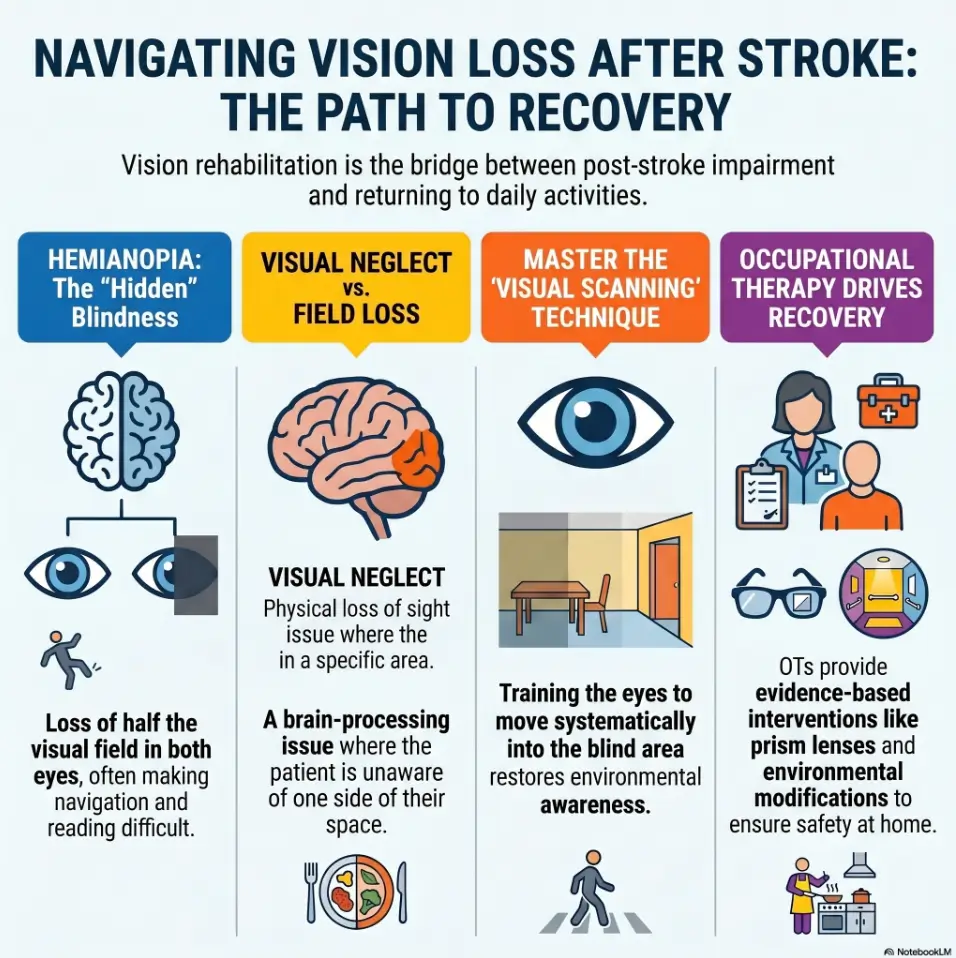
Hemianopia is a loss of vision on one side of the visual field, often affecting the same side in both eyes. If left unaddressed, meals become stressful and walking paths become riskier. Caregivers may mistake this visual field loss for simple carelessness.
This guide helps you build safer routines faster through practical, occupational-therapy-style thinking:
- 🔹 Consistent plate placement & simple plate clocks.
- 🔹 Doorway scanning & high-contrast cues.
- 🔹 Caregiver prompts that support without overwhelming.
Table of Contents
Safety / Disclaimer: This Is Home Strategy, Not Stroke Treatment
This guide is for home routine-building after stroke. It is not a diagnosis, not a substitute for rehabilitation, and not permission to resume risky tasks without professional input.
Stroke-related vision changes can overlap with balance problems, attention changes, swallowing difficulty, weakness, medication side effects, and fatigue. That is why a “simple” plate setup can be helpful, but it should sit inside a bigger care plan. The kitchen table is not a clinic, even when it starts feeling like one.
Use this as a routine-building guide, not a diagnosis
Hemianopia usually means loss of vision on one side of the visual field. A person may miss the same half of space in both eyes. But families may also hear terms like visual neglect, visual inattention, double vision, visual-perceptual impairment, or field cut. These are not interchangeable labels.
In lived home language, the difference may show up like this:
- The person leaves food on the same side of the plate.
- They bump one shoulder into doorframes.
- They miss people approaching from one side.
- They read only part of a line.
- They seem surprised by objects that were “right there.”
That pattern deserves clinical attention, not family blame. It may also belong beside broader warning-sign conversations, especially when families are trying to separate ordinary aging from senior vision changes that deserve prompt follow-up.
Keep the stroke team, eye doctor, and occupational therapist in the loop
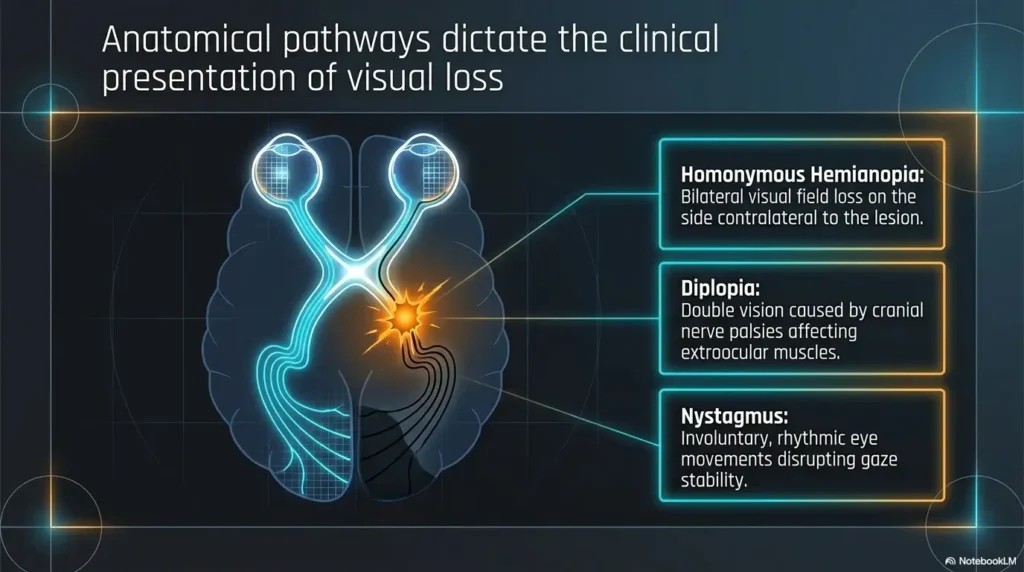
The American Stroke Association explains that many stroke survivors report vision difficulties, including reading problems, balance changes, depth perception changes, and visual memory problems. Canadian Stroke Best Practices recommends screening after stroke for visual field deficits, eye movement problems, central vision impairment, and visual-perceptual disorders as part of rehabilitation assessment.
In plain terms: if meals and doorways are becoming confusing, that is not too small to mention. Bring it up. Families who want a broader starting point can also review how vision loss after stroke can affect daily routines before the next appointment.
Do not use plate placement or doorway scanning as a substitute for rehab
Plate placement helps the home environment behave more predictably. Doorway scanning helps the person slow down before entering a risk-heavy space. Neither one repairs the stroke injury by itself.
Occupational therapy, vision rehabilitation, ophthalmology, optometry, physical therapy, speech therapy, and medical follow-up may all matter depending on the person’s symptoms. A person with hemianopia plus swallowing difficulty, for example, needs more than a clever placemat.
Driving, cooking, stairs, and bathing need extra caution
Driving may be unsafe or legally restricted after visual field loss. Cooking adds heat, sharp tools, timing, and divided attention. Stairs and bathing add fall risk. These are not “try harder” zones. They are clinician-guided zones.
Bathing deserves special caution because water, glare, slick surfaces, and visual field loss can gather in one unforgiving room. If the bathroom is part of the risk pattern, a separate home review of low vision nighttime bathroom safety can help families spot hazards before the 2 a.m. trip becomes a little disaster ballet.
- Use plate and doorway routines as safety support.
- Report missed food, bumping, falls, or navigation trouble.
- Ask directly about vision rehab and occupational therapy.
Apply in 60 seconds: Write down one repeated problem from this week, such as “left side of plate missed” or “right doorframe bumped,” and bring it to the next clinical visit.
Start Here: Hemianopia Is Not “Just Not Looking Hard Enough”
Families often describe hemianopia with moral words before they learn the medical words. “Careless.” “Not paying attention.” “Stubborn.” “Rushing.” Those words can do quiet damage.
After a stroke, one side of the visual world may not register normally. The person may not be ignoring the fork, doorframe, or visitor. Their brain may be receiving, processing, or attending to visual space differently. The missing half becomes a kind of silent furniture.
Why one side may vanish even when the eyes seem “fine”
Hemianopia can happen even when the eyes themselves are structurally healthy. The issue may be in the brain’s visual pathways after stroke. That is why a person may say, “My eyes are fine,” and still miss half the plate.
I have watched families point harder at the missing side, as if volume could become vision. It usually creates frustration first. Better strategy: build the missing side into the routine before frustration arrives.
The difference between visual field loss, neglect, and attention fatigue
Visual field loss means part of the visual field is reduced or absent. Neglect means the person may not attend to one side of space, often without full awareness. Fatigue can make either problem more obvious.
At breakfast, the person may scan beautifully. By dinner, after visitors, therapy, phone calls, and medication timing, the same person may miss half the table. This is not hypocrisy. It is a nervous system with a small battery icon blinking red.
Show me the nerdy details
Clinicians may test visual acuity, visual fields, eye movements, visual scanning, reading, spatial attention, and functional task performance. A home observation such as “misses food on the left at dinner” is not a diagnosis, but it is useful functional evidence. Specificity helps the rehab team separate field loss, neglect, fatigue, positioning, lighting, and task complexity.
Why families often mistake hemianopia for carelessness
Hemianopia can be inconsistent in daily life. The person may find the TV remote once and miss it the next time. They may pass through one doorway safely, then clip the next one. That inconsistency makes families suspicious.
But daily performance depends on lighting, clutter, speed, fatigue, pain, background noise, and whether the person is talking while moving. Add a barking dog and a hallway rug, and suddenly the room becomes a pop quiz with furniture.
The small danger zone: meals and doorways
Meals and doorways are deceptively rich with hazards. Meals involve plates, utensils, drinks, pills, napkins, hot food, swallowing, conversation, and divided attention. Doorways involve edges, thresholds, changing light, turning, people, pets, walkers, and rugs.
That is why this guide focuses on two everyday moments. They are small enough to practice and important enough to matter.
Who This Is For, and Who Should Not Use This Alone
This guide is best for families who are past the emergency moment and trying to make home life safer after stroke discharge. You may be a spouse, adult child, neighbor, home-health aide, or the person recovering. You may also be the unofficial Chief Finder of Lost Forks, which is a real job even if no one prints the badge.
Best fit: families adjusting home routines after stroke discharge
Use this if someone has already been evaluated for stroke and is now managing daily routines at home. The goal is not to redesign the entire house in one heroic weekend. The goal is to reduce repeatable risks in repeatable places.
Good candidates for this guide include families noticing:
- Food consistently left on one side of the plate.
- Drinks or utensils knocked from one table edge.
- Doorframes bumped on the same side.
- Clutter missed on one side of a walking path.
- More errors when tired, rushed, or distracted.
Best fit: caregivers noticing missed food, bumped doorframes, or one-sided scanning
Caregivers often see patterns before the survivor does. That can create tension. The survivor may feel watched. The caregiver may feel ignored. The toast, meanwhile, sits there like a witness.
Instead of arguing over whether the problem happened, track the pattern neutrally. “Missed food on left side at dinner 3 times this week” is more useful than “You never look left.”
Not enough: sudden new vision loss, confusion, weakness, or worsening balance
Do not use home strategy as a delay tactic for urgent symptoms. Sudden new vision loss, facial droop, arm weakness, speech trouble, severe dizziness, severe headache, sudden confusion, or abrupt worsening balance needs urgent medical help.
Stroke warning signs are time-sensitive. A placemat cannot compete with emergency care, and should not try.
Not enough: unsafe swallowing, severe neglect, or repeated falls
If the person coughs during meals, pockets food, loses weight, has repeated falls, forgets safety steps, or cannot follow scanning cues, ask for professional help. Speech-language pathology, occupational therapy, physical therapy, and medical review may be needed.
When falls or near-falls become part of the story, families may also need a wider room-by-room look at fall prevention at home for aging vision changes, because the problem is rarely only one doorway.
Eligibility Checklist: Is This Home Routine Appropriate Today?
| Question | Yes | Next step |
|---|---|---|
| Stroke symptoms are stable today? | Proceed gently | Practice one meal or one doorway only |
| No new facial droop, weakness, speech trouble, or sudden vision change? | Continue | If no, seek urgent medical help |
| Person can pause and follow a short cue? | Try routine | If no, ask OT for a simpler cue plan |
| Caregiver can observe without rushing? | Helpful | Use one phrase, not a lecture bouquet |
Neutral action: Choose the smallest safe practice zone before changing the whole house.
Plate Placement: Put the Meal Where Safety Can Find It
Plate placement is not about making the table look tidy. It is about helping the brain find the whole meal without turning breakfast into a scavenger hunt.
The first rule is consistency. A perfectly clever setup that changes every meal is less useful than a simple setup repeated 7 days in a row. The recovering brain likes boring. Boring is underrated. Boring saves the soup.
Place the plate with the affected side in mind, not just table symmetry
Ask the occupational therapist or vision rehab professional whether food should begin more toward the seeing side, the center, or whether scanning toward the affected side should be built into each meal. The right setup depends on the person’s visual field, attention, posture, cognition, arm use, and swallowing safety.
At home, avoid guessing based on décor. The plate does not need to satisfy the dining room. It needs to serve the person.
Keep high-risk items away from the blind-side edge
Hot coffee, pills, sharp knives, glass cups, and full bowls should not live casually on the affected-side edge without a cue or a stable routine. That edge can become an accidental launch zone.
For many families, moving the drink 4 inches inward and placing it on a contrasting coaster reduces spills immediately. It is not glamorous. Neither is mopping orange juice from under a chair at 7:10 a.m.
Use contrast so food does not disappear into the plate
Low contrast can hide food. White rice on a white plate, pale fish on a cream plate, clear water in a clear glass on a glass table: this is not a meal, it is camouflage.
Try:
- Dark plate for pale foods.
- Light plate for dark foods.
- Contrasting placemat under the plate.
- Colored coaster for the drink.
- Napkin marking the far side of the tray.
Kitchen contrast can also reduce knife and food-prep confusion. If meal prep remains part of the person’s routine, a guide to choosing the best cutting board color for low vision may help families think beyond the dinner plate.
Build a repeatable “plate clock” routine
A plate clock uses simple clock language to describe food locations: chicken at 6 o’clock, carrots at 3 o’clock, bread at 9 o’clock. It works because it gives the table a map.
- Keep high-risk items away from surprise edges.
- Use contrast for plates, trays, cups, and placemats.
- Repeat the same setup long enough for it to become familiar.
Apply in 60 seconds: Put tomorrow’s breakfast plate on a contrasting placemat and choose one fixed drink location.
The Plate Clock: A Simple Cue That Reduces Missed Food
The plate clock is one of those tiny tools that sounds almost too simple. Then you watch it work, and it feels like someone opened a window in a stuffy room.
Instead of saying, “You missed the left side,” you can say, “Check 9 o’clock.” That shift matters. One sounds like failure. The other sounds like navigation.
Use 12, 3, 6, and 9 o’clock language during meals
Start with four anchors. Too many details can overload the meal. If the person is already tired, hungry, or frustrated, do not turn lunch into air traffic control.
A simple script might be:
- “Your eggs are at 6 o’clock.”
- “Toast is at 9 o’clock.”
- “Fruit is at 3 o’clock.”
- “Cup is above the plate at 12 o’clock.”
Keep the same words for several days. Consistency is not childish. It is kindness with a calendar.
Start scanning from the safe side, then deliberately cross to the affected side
Some people do better when they begin scanning from the side they can detect more easily, then move across the plate to the affected side. Others may need direct training toward the affected side. This is where occupational therapy guidance helps.
The household version is simple: do not rush the scan. Let the person pause, look, turn the head if needed, and confirm the far side.
Mark the far edge with a napkin, placemat, or contrasting tray
A visual boundary can help the plate feel less endless. A contrasting tray edge, bold placemat, or folded napkin at the far side can become a landmark.
In one family kitchen I helped troubleshoot, the winning tool was not expensive adaptive equipment. It was a blue placemat and a stubborn commitment to leaving the cup in the same place for 2 weeks. The blue placemat deserved a tiny medal.
Let’s be honest: “Look harder” is not a strategy
“Look harder” is vague, emotionally loaded, and usually too late. Better cues are short, calm, and directional.
Mini Infographic: The Plate Clock Routine
12
Place cup or napkin above the plate only if safe and consistent.
3
Name food clearly: “Fruit at 3 o’clock.”
9
Use this side as a deliberate scan target if it is the missed side.
Scan path
Pause, locate center, sweep to far side, then begin eating.
Accessible note: This visual describes a plate as a clock face so caregivers can cue food locations with short, repeatable language.
Decision Card: Seeing-Side Placement vs Affected-Side Training
| Option | When it may help | Trade-off |
|---|---|---|
| Seeing-side start | Early meals, fatigue, low frustration tolerance | May not challenge scanning enough unless paired with deliberate sweep |
| Centered plate with clock cue | Person can follow simple cues | Requires caregiver consistency |
| Affected-side target | Therapist-guided scanning practice | Can frustrate or create spill risk if introduced too aggressively |
Neutral action: Ask OT which placement supports safety and skill-building for this specific person.
Doorway Scanning: Stop Before the Frame Becomes a Surprise
Doorways are tiny obstacle courses dressed as architecture. They combine edges, thresholds, handles, changing light, and traffic flow in one narrow little drama.
For someone with hemianopia after stroke, the problem is not only the doorway. It is arriving at the doorway while already moving, talking, carrying something, or turning the head toward a voice. That is when the frame becomes a surprise.
Pause before crossing every doorway
The safest doorway routine starts before the threshold. Stop first. Then scan. Then step.
This matters because scanning while moving divides attention. If the person is using a walker, cane, or has balance changes, moving and scanning at the same time may increase risk. A 2-second pause can be the difference between “nice recovery routine” and “why is the laundry basket attacking me?”
Scan the doorframe, floor, handle side, and room opening
Teach a sequence, not a vague command. A useful doorway scan checks:
- Doorframe on the affected side.
- Floor and threshold.
- Handle side or hinge side.
- Room opening beyond the doorway.
- Any pet, rug, cord, stool, walker wheel, or oxygen tubing.
Turn the head and eyes together toward the affected side
Depending on the visual loss, eye movement alone may not be enough. Many people need to turn the head and eyes together toward the affected side. This should be practiced slowly and safely.
One caregiver told me the cue that finally worked was not “watch out.” It was “find the far frame.” The phrase gave the person a target instead of a panic button.
Teach one phrase: “Stop, sweep, step”
Short phrases travel well. Long instructions fall apart in real rooms.
Try this:
- Stop: Feet still before the doorway.
- Sweep: Head and eyes scan toward the affected side and across the opening.
- Step: Move only after the path is clear.
- Stop before the threshold.
- Sweep the frame, floor, and room opening.
- Step only after the affected side has been checked.
Apply in 60 seconds: Pick one doorway today and practice “Stop, sweep, step” 3 calm times with no rushing.
The Hidden Half of a Room: Why Doorways Are Trickier Than Hallways
A hallway often gives the brain a corridor. A doorway gives it an ambush. The person must handle a narrow frame, a visual transition, a decision point, and whatever lives just beyond the opening.
That is why someone may walk down a hall safely but bump into the bedroom doorway. The hallway was predictable. The doorway had opinions.
A doorway creates edges, thresholds, people, pets, and clutter all at once
Doorways gather clutter like tide pools gather shells. Shoes, pet bowls, laundry baskets, walkers, cords, side tables, delivery boxes, and the family dog who believes every threshold is a nap invitation.
For someone missing one side of space, these objects may appear late. Late detection means late correction. Late correction can mean a bump, stumble, spill, or fall.
The affected side may hide a chair leg, oxygen tubing, rug corner, or walker wheel
Low objects are especially sneaky because they sit below the main line of sight. A person may scan at eye level and still miss the rug corner near the foot.
Try a doorway floor audit. Stand at the approach point and look specifically at the affected-side lower corner. If something lives there, move it. The best hazard is the one that never gets a chance to audition.
Lighting changes can make the blind-side risk worse
Doorways often sit between different lighting zones: bright kitchen to dim hallway, sunny living room to shadowy bedroom, bathroom glare to dark landing. The visual system may need a moment to adjust.
Use steady lighting where possible. Avoid glare that washes out edges. Add contrast tape or visual markers only if they help without creating visual clutter. If glare is part of the doorway problem, families may need to look at surface reflection too, especially on bright tile floors where white tile floor glare can make edges and thresholds harder to judge.
Here’s what no one tells you: the problem often starts before the person enters the room
The risky moment may begin 3 to 6 feet before the doorway. That is where the person turns, speeds up, responds to a voice, looks toward a caregiver, or starts carrying an item.
So place the cue before the doorway. Not inside it. Not after the bump. Before.
Quote-Prep List: What to Gather Before Comparing Home Safety Help
If you are comparing home health, outpatient OT, vision rehabilitation, or fall-prevention services, gather these details first:
- Which side is missed most often during meals or walking.
- How many doorway bumps or near-falls happened in the last 7 days.
- Whether the person uses a walker, cane, wheelchair, oxygen tubing, or shower chair.
- Which tasks are unsafe: meals, bathing, stairs, cooking, reading, medication setup, or driving.
- Insurance details and referral requirements, if applicable.
Neutral action: Bring this list to the stroke follow-up visit or therapy intake so the plan starts with real home friction, not guesswork.
Common Mistakes: Small Habits That Quietly Increase Risk
The hardest risks are not always dramatic. They are small habits repeated until the house quietly becomes less forgiving.
Most families are not careless. They are tired. They are improvising between medication times, appointments, laundry, work emails, and the emotional weather of recovery. Still, a few habits deserve eviction.
Don’t keep moving while scanning
Scanning while walking may sound efficient, but efficiency is not the goal when vision and balance are still recovering. Stop first. Then scan. Then move.
If the person resists stopping, try framing it as a skill drill, not a restriction: “We are practicing the doorway pause.” Adults generally prefer skill language over being managed like a runaway shopping cart.
Don’t place drinks, pills, or utensils on the affected-side edge without a cue
High-risk items need predictable placement. Pills should follow the medication plan from the clinician or pharmacist. Drinks should be stable and visible. Utensils should not hide on the side that already disappears.
For medication routines, visual field loss can turn tiny print, look-alike bottles, and shifted pill organizers into a quiet trap. A safer plan may include low vision medication management habits and tactile cues that make the right bottle easier to identify before the dose is due.
Don’t rearrange the table every meal
Variety is lovely in soup. It is less lovely in post-stroke safety routines.
Keep the table layout boring for at least a week while the person practices. Change one variable at a time. If everything moves, you will not know what helped.
Don’t shout directions from the blind side and expect instant response
A caregiver standing on the affected side and calling rapid instructions may not be detected quickly. This can startle the person or make them turn too fast.
Stand where the person can safely notice you. Use calm cues. Give time.
Don’t treat one good day as proof the problem is gone
Recovery can fluctuate. A good morning does not guarantee a safe evening. Fatigue, poor sleep, pain, dehydration, medication changes, and busy environments can bring errors back.
- Do not scan while moving through tight spaces.
- Do not keep changing plate or cup locations.
- Do not interpret one good day as full recovery.
Apply in 60 seconds: Remove one low object from the affected-side doorway path before the next room transfer.
Caregiver Cueing: Help Without Becoming a Human Alarm Bell
Caregiving after stroke can turn even gentle people into hallway sirens. “Watch out. No, left. LEFT. Your other left. Wait. Stop. Careful!” Nobody plans to become a talking smoke detector. It just happens.
The better path is cue design. Calm, repeatable, short, and timed early enough to help.
Use calm, repeatable prompts instead of rapid corrections
Choose 1 or 2 phrases for meals and doorways. Repeat them the same way.
Good options include:
- “Check the far side.”
- “Find 9 o’clock.”
- “Stop, sweep, step.”
- “Look to the doorframe.”
- “Pause before you cross.”
Avoid stacking 5 instructions in one breath. The brain after stroke is already doing heavy lifting.
Stand where the person can detect you safely
Caregiver position matters. If you stand on the affected side and speak suddenly, the person may startle or turn quickly. If you stand directly in the walking path, you may create a new obstacle.
Stand slightly ahead and toward the seeing side when appropriate, unless a therapist has advised otherwise. Your body should be a lighthouse, not a surprise furniture item.
Cue the action, not the failure
Try not to say, “You missed it again.” That sentence may be true, but truth without timing can bruise.
Use action language:
- “Sweep to the left edge.”
- “Check the floor by the frame.”
- “Find the cup at 12 o’clock.”
- “Pause, then step.”
Gradually reduce prompts only when the routine becomes reliable
Prompt reduction should be earned by consistency, not caregiver exhaustion. If the person completes the scan safely across multiple days and settings, you can reduce the cue from full phrase to gesture, then to silence.
But if errors return, bring the cue back without drama. Recovery is not a straight hallway. It has corners.
Mini Calculator: Caregiver Prompt Load
Use this quick estimate for 1 practice meal or 1 doorway routine. No storage, no tracking app required.
Neutral action: Share rising prompt load with OT or the stroke team, especially if safety is worsening.
Home Setup: Make the Blind Side Less Sneaky
A safer home does not need to look like a clinic. It needs to behave predictably. The goal is not to buy every device with a reassuring label. The goal is to make the missed side easier to detect before it causes trouble.
Start with the places used every day: eating area, bathroom doorway, bedroom doorway, favorite chair, kitchen path, medication zone, and route to the toilet at night.
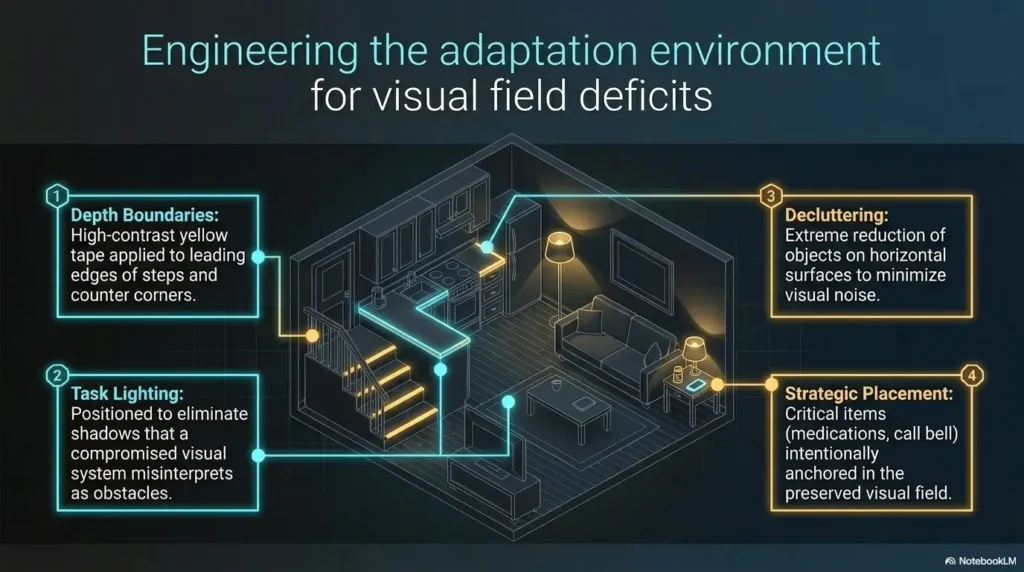
Add contrast to doorframes, thresholds, table edges, and chair backs
Contrast helps edges announce themselves. A dark chair against a dark floor may vanish. A white plate on a white tablecloth may become a little ghost buffet.
Use contrast where it matters:
- Doorframe edge on the affected side.
- Threshold strip if safe and flat.
- Contrasting placemat under the plate.
- Colored tape on walker handle only if approved and not distracting.
- Chair backs that stand out from the wall.
In bathrooms, contrast has to work alongside traction. If shower entry is part of the route, review anti-slip shower strip placement for low vision so the surface gives both the feet and the eyes a clearer path.
Remove low clutter from the affected-side travel path
Low clutter is rude because it hides below attention. Shoes, pet toys, laundry piles, cords, and footstools should not live in travel lanes.
Do a 5-minute floor sweep once a day. Not a full cleaning ritual. Just a hazard harvest.
Keep frequently used items in predictable zones
Predictable zones reduce search load. Put glasses, phone, water, medication organizer, remote, and walking aid in fixed locations. If something moves, tell the person before they need it.
This is especially important at night. A dark bedroom plus hemianopia plus urgency to use the bathroom is not a charming puzzle. It is risk wearing slippers. A bedside routine based on low vision bedside organization can keep glasses, phone, water, and walking aids from becoming midnight hide-and-seek contestants.
Use lighting that reveals edges without glare
More light is not always better. Glare can flatten edges and make shiny surfaces harder to interpret. Use soft, even lighting where possible. Add night lights along paths if recommended and safe.
For some homes, the problem is not darkness but harsh automatic lighting that startles the person or erases contrast. If that sounds familiar, troubleshooting a motion sensor light that is too bright may help the route feel safer without turning the hallway into a tiny interrogation room.
- Use contrast for plates, doorframes, and thresholds.
- Remove low clutter from the affected-side path.
- Keep daily items in fixed zones.
Apply in 60 seconds: Stand at the most-used doorway and remove anything below knee height on the affected-side approach.
When to Seek Help: Red Flags After Stroke Vision Loss
Home routines are useful only when the situation is medically stable. If something suddenly worsens, do not negotiate with the symptom. Get help.
The American Heart Association and American Stroke Association have long emphasized urgent recognition of stroke warning signs, because time matters in stroke care. In everyday family language: do not wait to see whether sudden changes “settle.”
Seek urgent medical help for sudden new vision loss, facial droop, arm weakness, speech trouble, severe dizziness, or sudden confusion
Call emergency services for sudden new or worsening stroke-like symptoms. This includes sudden vision change, facial droop, arm weakness, speech trouble, severe dizziness, severe headache, new confusion, or sudden trouble walking.
Even if the person already had a stroke, new symptoms deserve urgent attention. Families may also want a simple emergency information backup, such as a wallet card emergency info template for low vision, so key details are not trapped in someone’s memory during a stressful moment.
Contact the stroke team if bumping, falls, missed food, or navigation problems are increasing
If the pattern is getting worse over days or weeks, contact the stroke team, primary care clinician, neurologist, eye doctor, or rehabilitation team. Increasing errors may reflect fatigue, medication effects, new illness, vision changes, balance issues, cognition changes, or home hazards.
Ask for vision rehabilitation or occupational therapy if daily tasks remain unsafe
Vision rehabilitation and occupational therapy can help translate visual changes into safer daily routines. The American Occupational Therapy Association has practice guidance for adults with stroke, and occupational therapists commonly work on task adaptation, home safety, visual scanning strategies, and caregiver training.
Ask before driving; hemianopia can make driving unsafe or legally restricted
Driving is not just another errand. It requires fast visual detection, judgment, lane position, signs, pedestrians, mirrors, and hazard response. Hemianopia can affect driving safety and may affect legal eligibility depending on state rules and clinical findings.
Ask the physician, eye care professional, occupational therapist, or driver rehabilitation specialist before resuming driving. Do not use “I know the route” as the safety plan. Familiar roads still contain unfamiliar pedestrians. For a broader family conversation, senior driving safety can help frame driving as a risk decision, not a personal verdict.
Coverage Tier Map: What Support May Change From Basic to More Specialized Care
| Tier | Support type | What may change |
|---|---|---|
| 1 | Home routine | Consistent plate setup, clutter reduction, caregiver cues |
| 2 | Primary care or stroke follow-up | Medical review, referrals, medication and symptom discussion |
| 3 | Occupational therapy | Task-specific scanning, home safety, caregiver training |
| 4 | Vision rehabilitation or eye care | Visual field assessment, compensatory strategies, device discussion |
| 5 | Driver rehabilitation or specialized assessment | Driving readiness, legal requirements, behind-the-wheel risk review |
Neutral action: Match the support level to the risk pattern, not to family optimism or fear.
Next Step: Build One 7-Day “Plate and Doorway” Practice Loop
The safest plan is usually the one small enough to repeat. Do not redesign every room, every meal, and every movement pattern by Thursday. That is how good intentions become a junk drawer with medical vocabulary.
Pick one meal and one doorway. Practice daily for 7 days. Track the pattern. Bring the results to the rehab team.
Choose one meal and one doorway to practice every day
Breakfast is often a good meal because it repeats. Choose a doorway the person uses often, such as bedroom to hallway or kitchen to dining area.
Keep the practice short. One focused routine beats 12 scattered corrections.
Use the same cue phrase for both: “Stop, sweep, check the far side”
You can adapt the phrase, but keep it stable. For meals, the phrase might mean scanning the far side of the plate. For doorways, it means scanning the affected-side frame, floor, and opening.
Same phrase. Different settings. One mental groove.
Track three things: missed food, bumped edges, and caregiver prompts
Use a paper note, phone note, or calendar mark. Keep it simple:
- Missed food: yes or no.
- Bumped edge or near-miss: yes or no.
- Caregiver prompts: number used.
Patterns beat memory. Memory after a long caregiving day can become soup with receipts floating in it.
Bring the pattern to OT, vision rehab, or the stroke follow-up visit
Instead of saying, “Things are okay,” bring data from real rooms. “He needed 5 prompts at dinner but only 1 at breakfast.” “She bumps the right bathroom doorway at night.” “Missed food increases when the plate is white.”
Those details help clinicians adjust the plan.
Short Story: The Doorway That Told the Truth
Maria thought her father was rushing because he kept brushing the left side of the kitchen doorway. She reminded him, then warned him, then finally snapped one morning when coffee spilled across the floor. Later, during an OT visit, they practiced stopping 2 steps before the frame.
Her father turned his head slowly, scanned the left edge, checked the floor, and stepped through without touching the wall. The room had not changed. The timing had. That evening, Maria put a small strip of contrast tape on the left doorframe and moved the recycling bin away from the threshold. It felt almost embarrassingly simple. But for the first time all week, dinner began without a bump, a spill, or an apology hanging in the doorway.
FAQ
Can hemianopia after stroke improve over time?
Some people improve, some adapt, and some continue to have lasting visual field loss. Recovery depends on the stroke location, severity, time since stroke, other impairments, and rehabilitation plan. Families should avoid both despair and overpromising. A good goal is safer function while the clinical team monitors recovery.
Should food be placed on the seeing side or the affected side?
It depends. Early on, placing key items where the person can find them may reduce frustration and spills. But scanning toward the affected side may also be part of rehabilitation. Ask the occupational therapist or vision rehab professional for a side-specific plan. At home, consistency matters more than table symmetry.
What is the easiest plate setup for someone missing food on one side?
Start with a high-contrast plate and placemat, a fixed drink location, fewer items around the plate, and simple clock cues. For example, “Toast at 9 o’clock, eggs at 6 o’clock.” Keep hot drinks, pills, and sharp utensils away from risky edges unless there is a clear cueing plan.
How do you teach doorway scanning without overwhelming someone?
Use one short phrase: “Stop, sweep, step.” Practice at one doorway, not every doorway at once. The person stops before the threshold, turns head and eyes toward the affected side, checks the frame and floor, then steps through. Keep the first practice sessions calm and short.
Is bumping into doorframes a vision problem or a balance problem?
It can be either, both, or something else. Hemianopia, neglect, balance problems, weakness, fatigue, medication effects, poor lighting, clutter, and rushing can all contribute. Track which side, what time of day, and which doorway. Share that pattern with the stroke team or therapist.
Can occupational therapy help with plate placement and room scanning?
Yes. Occupational therapy often focuses on daily tasks, home safety, caregiver training, visual scanning strategies, adaptive routines, and safer participation in meals, bathing, dressing, mobility, and kitchen tasks. Ask for a referral if daily routines remain unsafe or exhausting.
Should caregivers sit on the affected side during meals?
Not automatically. Sitting on the affected side may encourage scanning for some people, but it may also startle, frustrate, or overload others. Ask the therapist what is appropriate. A safer first step is usually calm cueing, predictable plate setup, and high-contrast landmarks.
Is it safe to cook with hemianopia after stroke?
Cooking requires heat, knives, timing, reaching, reading labels, and moving through the kitchen. Hemianopia can increase risk, especially with fatigue or neglect. Ask the stroke team or occupational therapist before independent cooking. Start with supervised, low-risk tasks only if cleared. Families who are redesigning the kitchen for safer routines may also want to review low vision knife storage, especially when the affected side makes sharp tools easier to miss.
Is hemianopia the same as neglect?
No. Hemianopia is visual field loss. Neglect is reduced attention or awareness toward one side of space. They can look similar at home and may occur together. A clinical assessment helps separate the causes and guide the safest strategy.
What should I track before the next appointment?
Track missed food, spills, doorway bumps, near-falls, side of errors, time of day, fatigue, lighting, and how many prompts were needed. Bring examples, not just impressions. “Left-side food missed at dinner 4 of 7 days” gives the clinician something useful to work with.
Conclusion: Make the Missing Side Easier to Find
The peas left on one side of the plate and the shoulder brushing the doorway were never small clues. They were the house whispering, “This routine needs a map.”
Hemianopia after stroke can make one side of daily life harder to detect, but families do not have to answer that with panic or blame. Use consistent plate placement. Add contrast. Teach the plate clock. Pause before doorways. Practice “Stop, sweep, step.” Track what happens for 7 days, then bring the pattern to occupational therapy, vision rehabilitation, or the stroke follow-up visit.
Your 15-minute next step: choose one meal and one doorway today. Set the plate with contrast, move one hazard from the affected-side path, and practice one calm cue. Not the whole house. Not the whole recovery. Just one safer loop, repeated until the missing side becomes easier to find.
Last reviewed: 2026-04.