

Latanoprost vs Bimatoprost: Which Glaucoma Drop Has Fewer Side Effects?
Two weeks is all it takes for a “tiny bedtime sting” to turn into a silent habit of skipping—especially when your eyes look red by breakfast.
If you’re weighing Latanoprost vs Bimatoprost, you’re not shopping for a molecule. You’re trying to protect your vision and avoid the side effects that wreck consistency: conjunctival hyperemia (visible redness), burning, gritty ocular surface irritation, and the slow-burn cosmetic stuff like eyelash growth or iris pigmentation changes.
(If you’re over 60, the context around glaucoma eye drops side effects in seniors matters even more because baseline dryness and lid disease can amplify “tolerance.”)
Keep guessing, and the real cost isn’t discomfort—it’s drift: missed doses, unstable pressure, and avoidable risk.
This post helps you choose in minutes using FDA-label reality, plus a simple 7-night tracking method and technique tweaks (including punctal occlusion) that can reduce irritation.
- Screenshotable side-effect table (so you stop relying on memory)
- A 60-second tolerance estimator you can bring to your appointment
- Technique fixes that cut burn, spill, and preservative (BAK) fallout
Table of Contents
The quick answer in 5 minutes
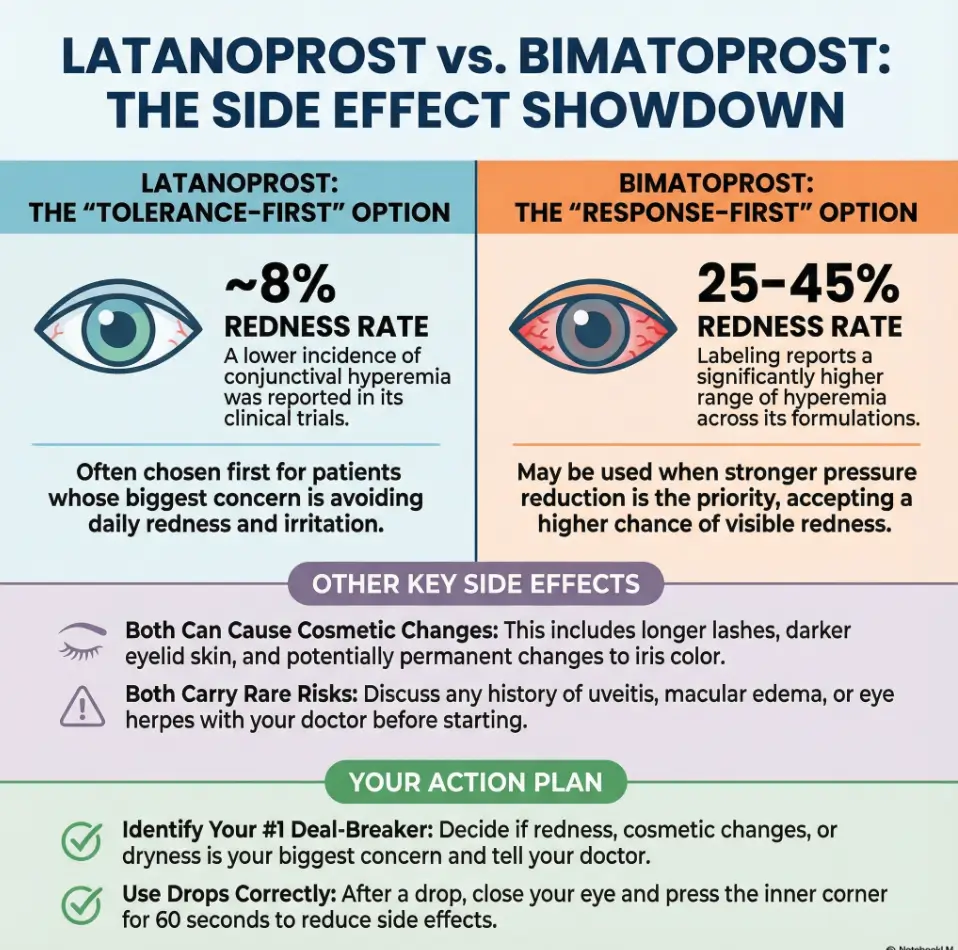
If your only goal is “fewer side effects,” here’s the practical reality: latanoprost is often better tolerated day-to-day, especially for redness, while bimatoprost more often causes visible redness—but it can still be the right choice for the right eye and the right person.
Why the split? These two drops sit in the same family, but your eyes don’t care about family reunions. They care about your ocular surface, your inflammation history, and how your eyelids and blood vessels react.
- Most common “quit factor”: persistent redness and irritation
- Most common “mirror factor”: lash/skin/contour changes over months
- Most important “safety factor”: inflammation or macular edema risk
Apply in 60 seconds: Write down your #1 deal-breaker (redness, dryness, cosmetic change, or flare risk) and bring it to your next appointment.
My own mistake early on: I treated side effects like a “comfort problem,” not a consistency problem. Two weeks of skipping “just this once” can turn into a habit faster than you think. In glaucoma, habits are the medication. (If you want a clear, appointment-ready overview of what gets checked and why, see what happens during a glaucoma test.)
- If you’re time-poor: pick the drop you’ll use nightly for 30 days straight.
- If you’re appearance-sensitive: ask about lid/iris changes up front, not after the photos show it.
- If you’ve had uveitis or retinal issues: treat that as a first-order decision factor, not a footnote.
What latanoprost and bimatoprost actually are
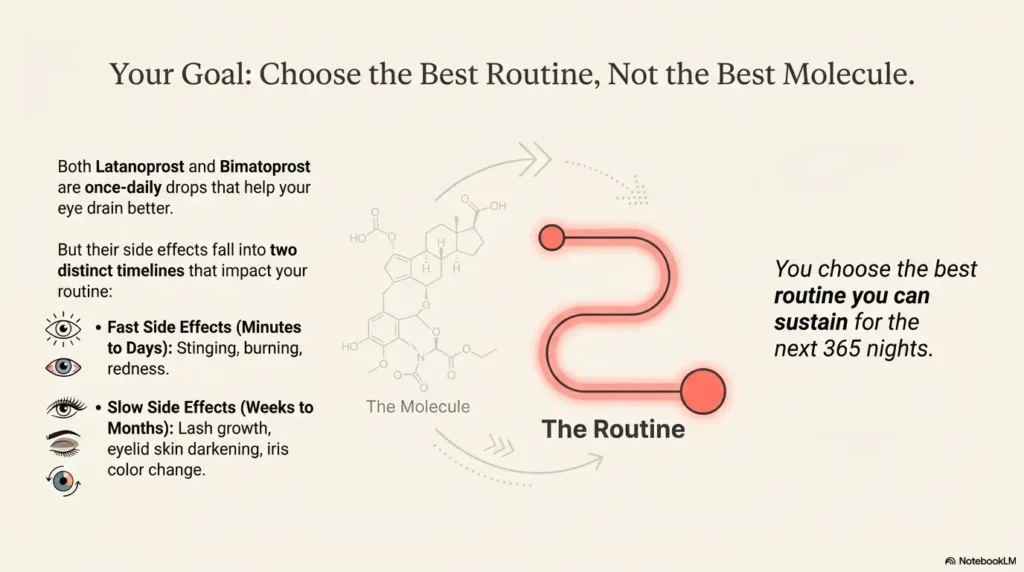
Both latanoprost and bimatoprost are once-daily glaucoma drops designed to lower intraocular pressure by improving outflow of fluid from the eye. In plain English: they help the eye drain better.
They’re often used as first-line therapy for open-angle glaucoma or ocular hypertension because they’re simple: one drop nightly, not a complicated schedule. And that matters when your life is already full of alarms you ignore. (If your numbers look “fine” but the story feels off, it can help to understand normal tension glaucoma after 60—because pressure is a number, not your whole risk profile.)
Here’s the non-obvious part: “side effects” here aren’t just a checklist. They fall into two buckets:
- Fast side effects within minutes to days: stinging, burning, foreign-body sensation, redness.
- Slow side effects over weeks to months: lash growth, eyelid skin darkening, and sometimes iris color change.
I once told myself, “It’s just a little burn.” Then I started dreading bedtime like it was a dentist appointment. The drop didn’t fail me. My routine did.
Operator mindset: You don’t choose “the best molecule.” You choose the best routine you can sustain for the next 365 nights.
Redness and stinging: the side effect that ruins compliance
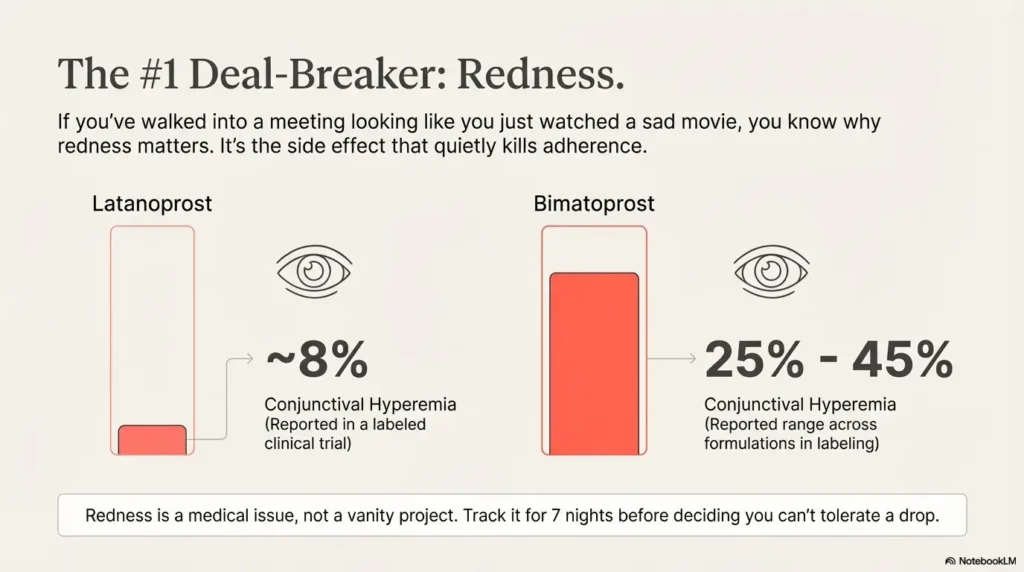
If you’ve ever walked into a meeting looking like you watched a sad movie on an airplane, you already understand why redness is the side effect that matters. It’s visible, it’s constant, and it makes people quit.
In FDA clinical-trial reporting, latanoprost commonly shows conjunctival hyperemia in the single digits percentage-wise, while bimatoprost labeling reports a much higher range for hyperemia across formulations. That doesn’t mean you personally will land on the worst end of the range—but it explains why many clinicians describe bimatoprost as more likely to look red.
Numbers that are worth knowing (because they shape expectations):
- 1 drop nightly is the standard dosing for both.
- 5 minutes is the minimum spacing between different drops if you use more than one.
- 15 minutes is a practical contact-lens wait time many labels use before reinsertion.
Show me the nerdy details
Redness is not just “irritation.” Prostaglandin analogs can increase superficial vessel prominence and alter local inflammatory signaling. Two people can have the same pressure drop and completely different redness. That’s why your doctor asks about symptoms even when the pressure number looks great.
My small trick after a bad week: I wrote “redness vs. regret” on a sticky note. If the redness was tolerable, I stayed consistent. If it wasn’t, I didn’t “tough it out” silently—I asked for an adjustment.
- Track redness for 7 nights before you declare “I can’t tolerate this.”
- Note if it’s worst in the first 30 minutes or lasts all day.
- Tell your doctor if you’re using contact lenses or lubricating drops.
Apply in 60 seconds: Take one well-lit selfie at the same time each day for 7 days to document change. If you prefer a printable version (especially helpful for parents), use a printable symptom diary for seniors.
Cosmetic changes: lashes, eyelid skin, and iris color
Both drops can cause lash growth and darkening—sometimes it’s a “free mascara” moment, and sometimes it’s “why do my lashes poke my eye now?” The difference is often intensity and how noticeable it becomes for you.
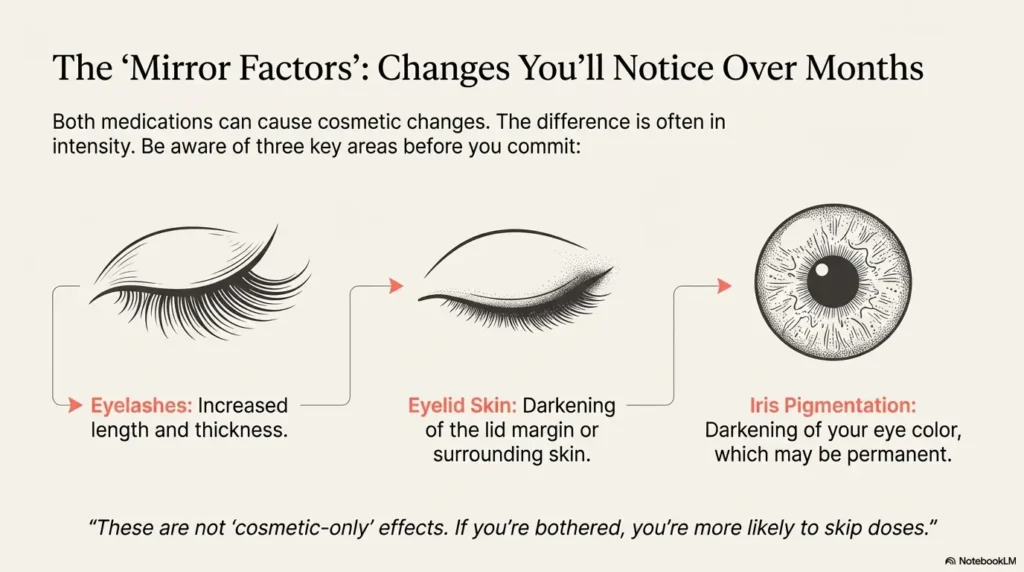
Three cosmetic effects to understand before you commit for months:
- Eyelashes: increased length, thickness, and number can happen with both.
- Eyelid skin: the lid margin or periorbital skin can darken in some users.
- Iris pigmentation: darkening of the iris can occur and may be permanent, especially in mixed-color irises.
Anecdote from the real world: a friend once celebrated “amazing lashes”… until the lashes started growing a little sideways and scratching the eye. Glamour lasted 8 weeks. Irritation lasted until the regimen changed.
What “fewer side effects” means here depends on your priorities:
- If you hate visible redness, you’ll usually care more about hyperemia.
- If you dislike appearance changes, you’ll care more about skin/contour and iris changes.
Quiet truth: These are not “cosmetic-only” effects. If you’re bothered, you’re more likely to skip doses.
In 2025 reality, many time-poor people choose “tolerable now” over “perfect later.” That’s human. It’s also why it’s worth discussing these changes early—before you’ve invested 90 days of habit. If your worry is “am I overreacting?” this framing can be clarifying: is it just getting older—or could it be serious eye disease?
The rare risks: uveitis, macular edema, herpes keratitis
This is the part most blog posts whisper about. I won’t whisper. If you have a history of certain eye conditions, prostaglandin analogs may require extra caution—sometimes a different first choice, sometimes closer monitoring. (If your risk context includes genetics, this is worth a quick read: family history of eye disease.)
Three “ask your doctor directly” flags:
- Uveitis or iritis history: these drops can aggravate intraocular inflammation in susceptible patients.
- Macular edema risk: especially after cataract surgery or in certain lens situations, risk discussions matter. (If you’ve recently had surgery, the “what could happen” list is here: cataract surgery complications in seniors.)
- Herpes simplex keratitis history: reactivation has been reported in labeling for this drug class.
I once made the classic time-poor move: I assumed “my old episode was years ago, so it doesn’t count.” It counts. Not as panic—just as context.
Show me the nerdy details
When labels talk about inflammation or macular edema, they’re describing postmarketing reports and clinical caution areas where causality can be hard to prove but risk management is still prudent. The clinical move is not fear; it’s targeted screening and a plan for what to do if symptoms flare.
Useful numbers here are not dramatic statistics; they’re practical timelines:
- If vision distortion or new floaters appear, don’t “watch it” for 2 weeks—call.
- If severe pain, light sensitivity, or sudden blurred vision shows up, treat it like a same-day problem.
- If you recently had eye surgery, ask what monitoring is needed over the next 4–6 weeks. (If you’re in that 65+ window, this timeline lens helps: cataract surgery after 65.)
- Tell your doctor about any prior uveitis, retinal swelling, or herpes eye disease.
- Ask what symptom should trigger a same-day call.
- Get clarity on follow-up timing in the next 30 days.
Apply in 60 seconds: Open your phone notes and list your last 3 eye diagnoses and surgeries in one line each.
Dry eye and preservatives: why the bottle matters
Sometimes the enemy isn’t latanoprost or bimatoprost. It’s the preservative load hitting an already cranky ocular surface.
Many multi-dose glaucoma drops use benzalkonium chloride, often called BAK. For some people, BAK is fine. For others, it’s the difference between “I can live with this” and “my eyes feel sandblasted by lunch.”
Two practical points that save time:
- If you already use artificial tears more than 2 times a day, tell your doctor that up front.
- If you’re on 2 or more prescription drops, preservative exposure adds up—your symptoms may be cumulative.
Show me the nerdy details
Ocular surface irritation is multifactorial: preservative toxicity, meibomian gland dysfunction, and baseline dry eye can all amplify the same drop’s “feel.” When someone says “I can’t tolerate prostaglandins,” the real issue is often ocular surface optimization rather than the drug class itself.
I’ve had nights where the drop stung and I blamed the medication—then realized I’d just used a face wash that migrated into my eyes. Glaucoma drops aren’t fragile, but your eyelid margin can be.
Simple technique matters: blot overflow from the eyelid skin. It’s a tiny move that can reduce skin darkening and irritation over time.
Money Block: 60-second eligibility checklist
Use this as a binary “yes/no” screen before you spend time comparing brands, copays, or formulary tiers. It’s not a diagnosis—just a faster way to ask better questions. (If you’re in the U.S. and cost decisions are tied to coverage rules, these two pages can save you phone-tag: high risk for glaucoma on Medicare and Medicare glaucoma screening for diabetics.)
- Yes/No: Have you ever been told you had uveitis or iritis?
- Yes/No: Have you had macular edema or retinal swelling, especially after surgery?
- Yes/No: Have you had herpes infection in the eye?
- Yes/No: Do you wear contact lenses daily for more than 8 hours?
- Yes/No: Do you use artificial tears more than 2–3 times a day?
Next step: If you answered “Yes” to any, ask your eye doctor what monitoring or alternative options make sense for you.
Neutral action: Save this checklist and confirm current precautions on the medication’s official prescribing information.
Decision card: when to choose A vs B
This is the part readers want: the clean, honest “pick this if…” without pretending we can replace your doctor. Here’s a decision card that matches how real clinics think—benefit, tolerance, and risk.
- Redness is your #1 deal-breaker for daily life.
- You want a widely used, once-nightly baseline option.
- You’re trying to reduce “drop dread” over the first 30 days.
Trade-off: Cosmetic changes are still possible over months.
- Your doctor is targeting stronger response or a different individual response profile.
- You tried latanoprost and pressure goals weren’t met.
- You accept a higher chance of visible redness in exchange for the plan.
Trade-off: Hyperemia can be more common and more noticeable.
Neutral action: Save this card and ask for a written plan that includes follow-up timing and what to do if redness is intolerable.
Money Block: side-effect rate table you can screenshot
You don’t need a spreadsheet to make a decision—but you do need a grounded sense of scale. Below is a plain-language table using numbers reported in FDA labeling and clinical-trial summaries. Keep one rule in mind: trial rates vary, and people vary more.
These figures reflect ranges or incidence reported in labeling for branded reference products. Use them as expectation-setting, not a personal prediction.
| Side effect | Latanoprost | Bimatoprost | Notes |
|---|---|---|---|
| Conjunctival hyperemia | About 8% reported in a labeled clinical-trial table | Reported range 25%–45% across formulations in labeling | This is the “looks red” effect that often drives switching. |
| Burning/stinging | Around 7%–9% in labeled trial tables | Commonly reported; labeling highlights burning/irritation among reported events | Technique and dry-eye status can change the “feel” dramatically. |
| Foreign-body sensation | About 13% in a labeled trial table | Reported among common ocular reactions | Often overlaps with baseline dry eye or lid margin disease. |
| Iris pigmentation increase | About 7% in a labeled trial table | Reported in labeling; exact rates vary by study and population | Can be gradual over months to years; may be permanent. |
| Discontinuation due to redness | Less than 1% noted in labeling | About 0.5%–3% noted in labeling | A small percentage matters because it represents real-life intolerance. |
| Year marker | Label revision noted as 2022 for one reference label | Label document commonly circulated as 2012 for one reference label | Label dates reflect document updates, not when your generic was made. |
Neutral action: Screenshot this table and confirm the latest label version on the official FDA database page.
Money Block: a 60-second “tolerance estimator”
This tiny tool won’t diagnose you. It will do something more useful: it turns your priorities into a clean question to bring to your next visit, especially if you’re juggling copays, prior authorization, or formulary tier switches. (If you’re also navigating procedure-related bills, these pages may help you frame the cost conversation: cataract surgery and Medicare Part B and how a cataract surgery bill is structured.)
Choose options, then read the output. Inputs: 3. Output: 1–2 lines.
Output will appear here.
Neutral action: Save your output text and ask your provider whether switching within the same class or adjusting formulation is appropriate.
How to use drops to reduce side effects
This is the simplest section and the one that saves the most suffering. Technique can reduce burning, skin darkening, and “why is my eyelid itchy?” moments. It’s not glamorous. It’s effective.
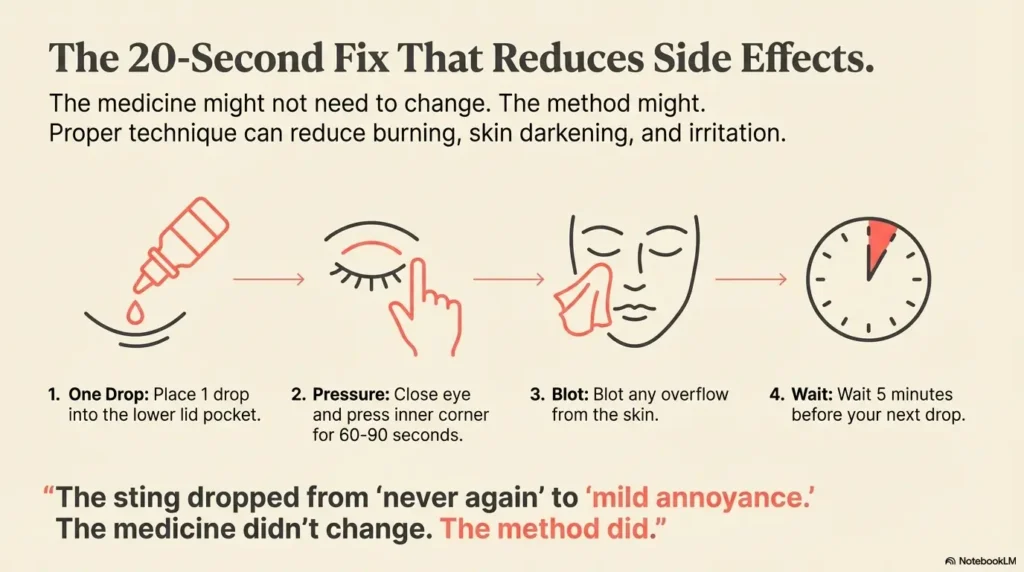
My own “I can’t believe I didn’t do this” fix took 20 seconds:
- Wash hands, dry them fully.
- Pull the lower lid gently, place 1 drop into the pocket.
- Close the eye and press lightly at the inner corner for 60–90 seconds.
- Blot overflow from the skin with a clean tissue.
Why it works: you reduce drainage into the nose and throat, reduce skin exposure, and give the drug time to absorb where it belongs.
Small discipline, big payoff: one drop, one minute of gentle corner pressure, and you often cut the “taste in throat” effect too.
Two more practical numbers:
- If you use two drops, separate them by 5 minutes.
- If you wear contacts, consider the 15-minute pause before reinsertion.
Anecdote: I once doubled a drop because I thought “more is better.” It wasn’t. It was messier, stingier, and it didn’t make me twice as protected. In glaucoma drops, more often just means more spill.
One-glance infographic and the 15-minute next step
Let’s close the loop from the hook: you want fewer side effects, because you want a plan you can live with. Here’s a one-glance infographic you can screenshot—then a 15-minute next step to act on it today.
- Redness: commonly lower reported trial incidence than bimatoprost labeling ranges
- Sting/feel: can still happen; technique matters
- Cosmetic: lashes/skin/iris changes possible over months
- Routine: once nightly, keep it boring
Best for: people who will quit if they look red.
- Redness: labeling reports higher hyperemia ranges
- Itch/lash growth: commonly reported reactions
- Cosmetic: similar category of changes, sometimes more noticeable
- Plan: set expectations for first 30 days
Best for: people needing a different response after first-line fails.
- Pick your deal-breaker: redness, dryness, cosmetic change, or flare risk.
- Run the estimator above and copy the output into a note.
- Message your clinic with one question: “If I can’t tolerate redness by day 14, what’s our next step?”
- Choose based on your #1 deal-breaker, not internet bravado.
- Document symptoms for 7 nights before switching.
- Ask for a written follow-up plan in the next 30 days.
Apply in 60 seconds: Set a recurring bedtime reminder labeled “1 drop, 1 minute corner pressure.”
FAQ
1) Which has fewer side effects overall: latanoprost or bimatoprost?
Many people experience fewer day-to-day tolerance issues with latanoprost, especially regarding visible redness. Bimatoprost can be more noticeable for hyperemia in labeling summaries, but individual response varies and sometimes it’s chosen for response goals. 60-second action: decide whether redness or pressure response is your top priority and tell your doctor in one sentence.
2) Will either drop change my eye color permanently?
Iris darkening can occur gradually over months to years with prostaglandin-class drops, and it may be permanent. It’s more noticeable in mixed-color irises. 60-second action: take a baseline photo of both eyes in the same lighting today.
3) Do these drops cause “sunken eyes” or eyelid contour changes?
Periorbital and lid changes have been reported with this drug class, including deepening of the eyelid sulcus in some cases. Not everyone experiences this, but if appearance changes matter to you, it should be part of the decision. 60-second action: compare a current photo with one from 6–12 months ago and note any asymmetry.
4) I’m getting stinging—should I stop immediately?
Mild stinging can occur, especially early, and technique can reduce it. But severe pain, major light sensitivity, or sudden vision changes should be treated as urgent. Do not stop on your own without a plan if glaucoma control is at stake. 60-second action: write down severity from 1–10 and how long it lasts, then call if it’s escalating.
5) Can I use both latanoprost and bimatoprost together?
Using two drugs from the same prostaglandin class together is generally not a typical strategy and can be counterproductive; your doctor will usually choose one and then add a different class or a combination product if needed. 60-second action: read your current drop list and confirm each drug class with your pharmacist.
6) How long should I trial a drop before deciding it’s “not tolerable”?
Many tolerance issues reveal themselves within the first 7–14 days, while cosmetic changes may unfold over 8–12 weeks. A structured, short trial with symptom tracking is better than random skipping. 60-second action: commit to 7 nights of consistent technique and document redness daily.
7) What should I ask if I’m worried about cost, copay, or prior authorization?
Ask for the exact medication name, concentration, and acceptable substitutes; then ask what the next step is if your formulary denies it. “Out-of-pocket” surprises happen when the plan is vague. 60-second action: call your pharmacy and ask what alternatives are on your plan’s formulary tier list.
Conclusion
Back to the hook: you don’t want the “strongest” drop on paper—you want the drop you’ll take every night without negotiating with your own face in the mirror. If you’re choosing strictly by side effects, latanoprost often wins for everyday tolerance, especially redness. If your pressure goals or personal response demand it, bimatoprost may still be the right tool—just with more deliberate expectation-setting.
Next step in 15 minutes: run the estimator above, screenshot the rate table and infographic, and send one message to your clinic: “My #1 deal-breaker is ___; if that happens by day 14, what’s our next step?” That single question turns uncertainty into a plan. If you want to walk into that conversation with zero ambiguity, revisit what happens during a glaucoma test so your questions match what the clinic is measuring.
Last reviewed: 2025-12. This article is based on official prescribing information for reference products plus patient-education guidance from major ophthalmology organizations.