


Mastering Your Morning: A Guide to Dizziness and Fall Prevention
Most people don’t fall because of a dramatic medical event—they fall in the first 20 minutes after getting out of bed. When blood pressure drugs and vision changes collide, mornings can feel like walking through a camera that won’t focus.
The hardest part is that symptoms can look similar while causes are very different: medication timing, orthostatic hypotension, dehydration, or a true neurologic emergency. If you “wait and see” without a clear system, you risk preventable falls and dangerous delays.
This guide provides a practical triage flow to help you separate manageable blurry mornings from red-flag symptoms—before breakfast.
Our approach is built on a simple, clinical pattern method: time-stamped symptom logging, posture-linked blood pressure checks, and escalation thresholds aligned with major public guidance on stroke warning signs.
Table of Contents

Fast Answer
Blood pressure medicines can cause blurry vision or dizziness in some people, especially after dose changes or when symptoms cluster around standing, dehydration, or medication peak time. The key is pattern recognition and safety: do not stop medication abruptly, track timing carefully, and contact your clinician for dose/timing review. If you have sudden vision loss, severe eye pain, fainting, chest pain, shortness of breath, face droop, arm weakness, or speech trouble, treat it as an emergency and call 911.
- Do not self-stop or self-double doses.
- Track symptom timing for 7 days.
- Escalate quickly for vision-loss or stroke signs.
Apply in 60 seconds: Put a note in your phone now: “Log first symptom time tomorrow.”
Who This Guide Is For (and Not For)
Who this is for
- US adults with new blurry mornings, lightheadedness, or dose-related dizziness after starting/changing antihypertensives
- Caregivers trying to reduce fall risk for a parent or partner
- People on one or more BP medications who need a safer morning workflow
Who this is not for
- Anyone with acute emergency signs right now (sudden vision loss, fainting, stroke-like symptoms, severe chest pain, severe breathing trouble)
- People seeking a diagnosis without medical assessment
- Anyone planning to stop medications without clinician guidance
I once helped a family member sort this exact mess: “Is this medicine side effect, dehydration, or something worse?” The breakthrough was not a miracle supplement. It was a humble timeline: wake time, stand time, pill time, first symptom time, and what happened after water + breakfast. In three days, the pattern became obvious enough that the clinician made a precise adjustment instead of guessing.
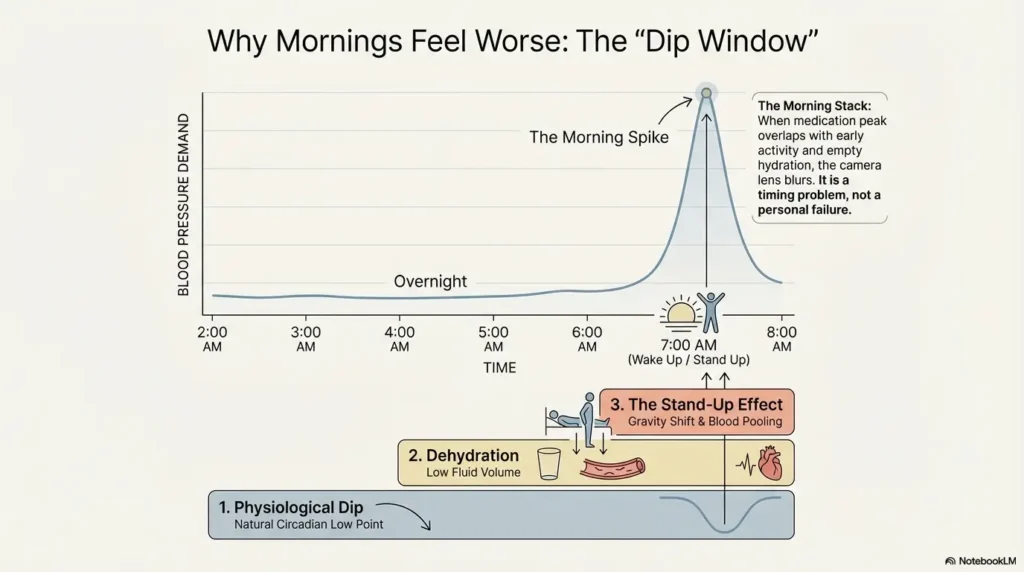
Why Mornings Feel Worse: The Blood Pressure “Dip Window”
Overnight dip + morning stand-up effect
Blood pressure often shifts overnight. Then morning posture changes hit fast: lying to sitting to standing. If circulation does not adapt quickly, symptoms can show up as blur, “head rush,” wobbliness, or near-faint feelings. This posture-linked pattern is common in orthostatic intolerance and can be amplified by dehydration.
Medication timing and peak effect
Same medication, different hour, different experience. Some people feel worse when the dose peak overlaps with early activity; others feel rough if nighttime medication carries into an under-hydrated morning. The mechanism matters less than the practical result: timing can be adjusted safely, but only with your prescriber.
Here’s what no one tells you…
In clinic, symptom timing is often more actionable than symptom intensity. “It’s a 4/10 blur every morning within 20 minutes of standing” can be more useful than “sometimes I feel bad.”
Public guidance from major US medical sources consistently notes that orthostatic symptoms can include dizziness and blurry vision, and that dehydration can worsen this pattern. That’s why your morning sequence—not just your prescription name—matters. If this is happening regularly, compare your notes with this focused guide on waking up with blurry vision and what patterns matter most.
Show me the nerdy details
Orthostatic symptoms are tied to rapid blood pressure regulation when changing posture. If vascular tone, heart-rate response, or circulating volume lags, transient cerebral perfusion drops can produce dizziness, dim vision, or instability. Medication timing, volume status, autonomic function, and multi-drug combinations all influence this response.
- Stand in stages, not in one jump.
- Hydrate before your busiest first tasks.
- Track symptoms relative to posture and dose time.
Apply in 60 seconds: Move a water bottle to your bedside tonight.
Vision Changes That Are Usually Side Effects vs Signs You Shouldn’t Ignore
Often medication-related (non-emergency, still report)
- Intermittent blur when rising quickly
- Mild foggy focus that improves with hydration, food, seated rest, or slower transitions
- Short episodes clustered near medication timing
Red-flag eye symptoms (urgent)
- Sudden vision blackout or “curtain” effect
- Persistent double vision
- Severe eye pain with nausea/headache
- New severe headache with visual disturbance
Stroke/cardiac overlap signs (emergency)
- Face droop, arm weakness, trouble speaking/understanding
- Sudden trouble walking or severe imbalance
- Chest pain, severe shortness of breath, fainting
CDC stroke guidance includes sudden trouble seeing, dizziness, balance trouble, and speech/weakness changes as emergency signals. If those symptoms appear, do not “observe for a few hours.” Call 911 immediately. For families managing recovery after a vascular event, this companion explainer on vision loss after stroke and urgent follow-up signs can help with next-step triage.
Don’t Make These 7 Mistakes in the First Week of Symptoms
Mistake #1: Stopping blood pressure meds abruptly
Sudden discontinuation can create dangerous rebounds in some cases. It feels decisive, but it can be risky.
Mistake #2: Waiting it out with no log
No timeline means your clinician is flying blind. If you prefer a ready-made format, use a printable symptom diary for seniors and keep entries short but time-stamped.
Mistake #3: Skipping hydration and meals
Low fluid volume + BP medication can worsen dizziness.
Mistake #4: Driving during active blur episodes
Not worth it. Reschedule, rideshare, ask for help, or delay departure. If driving confidence has already dropped, review broader senior driving safety adjustments for vision-related risk before returning to routine trips.
Mistake #5: Using OTC decongestants without checking
Some cold medications can raise BP or conflict with your regimen.
Mistake #6: Doubling after a missed dose
Follow your label and clinician plan; don’t improvise.
Mistake #7: Bad home BP technique
Wrong cuff size, arm position, and rushed timing distort decisions.
Quick personal confession: I used to check BP after sprinting up stairs with coffee in hand and then wonder why numbers looked dramatic. Clean technique fixed half the anxiety in one week.
- No abrupt stops.
- No dose doubling.
- No driving during active visual symptoms.
Apply in 60 seconds: Add your pharmacy number to favorites for interaction questions.
Is It the Medication, the Dose, or Something Else? (Quick Triage Framework)
Pattern A: Symptoms right after dose
Could suggest peak-effect intolerance. Bring exact onset timing to your clinician.
Pattern B: Symptoms on standing only
Could reflect orthostatic drop, deconditioning, or low intravascular volume pattern.
Pattern C: Persistent blur regardless of posture
Needs eye-specific evaluation sooner; don’t assume “just meds.”
Pattern D: New symptoms after adding a second BP drug
Combination therapy can create cumulative effects—especially in mornings.
Let’s be honest…
“I don’t want to bother my doctor” sounds polite, but it delays easy fixes. Most prescribing teams prefer a quick early adjustment to an avoidable fall, ER visit, or self-discontinuation cycle.
Decision Card: When A vs B
When A (watch + call within 24h): Mild, brief episodes linked to standing; symptoms improve with seated rest/hydration; no red flags.
When B (same-day urgent care): Worsening instability, persistent double vision, vomiting/dehydration, unsafe gait.
When C (911 now): Sudden vision loss, fainting, stroke signs, severe chest pain, severe breathing difficulty.
Neutral action: Choose the lane now and share your symptom timeline with a clinician.
Your 3-Minute Symptom Log That Gets Better Appointments
What to track daily
- Medication time and dose
- Wake time and first stand time
- Hydration (first glass, total by noon)
- Meals/snacks timing
- Symptoms (what, when, how long)
- BP and HR with posture note (lying/sitting/standing)
The “morning stack” checklist
- Wake
- Sit 1–2 minutes
- Stand slowly
- Water
- Medication
- First symptom time
How to present it in clinic
One-page timeline wins. Bring 7 days. Circle 2 worst mornings and 2 best mornings. Clinicians can compare conditions and tune treatment faster.
Mini calculator (no app needed)
Input 1: Number of dizzy/blur episodes before noon (per day)
Input 2: Average duration in minutes
Input 3: Number of near-falls this week
Output: Symptom burden score = (episodes × minutes) + (near-falls × 20).
If score rises for 3 days or any near-fall occurs, escalate clinician contact.
Neutral action: Calculate once nightly for 7 days.
Show me the nerdy details
Clinicians can adjust dose, split dosing, switch agent class, review heart rate effects, and evaluate orthostatic response more safely when they see structured longitudinal data rather than isolated snapshots.
Medication Classes and Side-Effect Patterns (Without Guesswork)
Diuretics and dehydration-linked dizziness
Diuretics lower BP partly by reducing fluid volume. That is useful therapeutically, but in some people it can increase morning lightheadedness if hydration is poor or illness reduces intake.
Beta blockers and fatigue/low-heart-rate sensations
Some beta blockers can reduce heart rate and produce fatigue or “sluggish” mornings in sensitive patients. Visual complaints may ride alongside tiredness and reduced exercise tolerance.
ACE inhibitors / ARBs / calcium channel blockers
These classes have distinct profiles, but real-world symptoms still depend on timing, combinations, comorbidities, and individual response. Mechanism matters; lived pattern matters more.
Combination therapy: small changes, big shifts
Adding one extra medication can transform morning tolerance. A “small” change on paper can feel huge at 6:30 a.m.
Fee/Rate-style reference table (practical pattern map)
| Class | Typical Symptom Pattern | What to Track | Next Step |
|---|---|---|---|
| Diuretics | Morning lightheadedness, volume-sensitive days | Fluid intake, illness, first-stand symptoms | Review hydration + timing with prescriber |
| Beta blockers | Fatigue, lower-HR sensations, slower mornings | HR trend, exercise tolerance, symptom window | Clinician review for dose or class fit |
| ACEi/ARB/CCB | Variable by patient and combination | Posture relation + exact timing | Targeted adjustments, not abrupt stops |
Neutral action: Bring this pattern table to your next medication review and annotate your own timeline.
When to Call Your Doctor vs When to Seek Emergency Care
Call your doctor within 24 hours if…
- Blurry mornings recur for more than 2–3 days
- You have near-falls or unsafe unsteadiness
- Symptoms cluster near dose timing
- Home readings are repeatedly much lower/higher than your usual pattern
Same-day urgent care if…
- Symptoms are worsening despite rest/hydration
- You cannot walk steadily
- Persistent double vision appears
- Vomiting or dehydration limits oral intake
Call 911 now if…
- Sudden vision loss
- Fainting
- Stroke signs (face/arm/speech/seeing/walking changes)
- Severe chest pain or severe shortness of breath
- Uncertain + worsening = same-day evaluation.
- Neurologic/cardiac red flags = emergency response.
- Recurrent mild patterns = timely prescriber adjustment.
Apply in 60 seconds: Save your local urgent care and emergency contact info now.
Safer Daily Routine: Morning-Proof Your First 90 Minutes
Stand-up protocol (bed → sit → stand)
Pause at each transition for 30–120 seconds. If symptoms appear, sit back down and retry slower. This tiny pacing often prevents the worst “rush” episodes.
Hydration + breakfast sequence
If your clinician permits normal fluid intake, start with water before high-demand tasks. Add a modest breakfast when possible. For many people, an empty tank plus quick movement is the perfect storm.
Home safety edits that prevent falls
- Brighten hallway/bedside lighting
- Install grab points in bathroom/shower zones
- Avoid ladders/chairs on symptomatic days
- Delay showering until steadier if mornings are rough
If you want a room-by-room setup, this practical checklist on aging vision and fall prevention at home pairs well with the routine above. Nighttime is another common risk window, so it also helps to review low-vision nighttime bathroom safety fixes before the next near-fall happens.
Eligibility checklist (yes/no safety gate)
Before driving, stairs, or solo errands:
- Any active blur right now? (Yes/No)
- Any dizziness on standing in last 30 minutes? (Yes/No)
- Any near-fall this morning? (Yes/No)
- Any new neurologic/chest/breathing symptoms? (Yes/No)
If any “Yes,” scale down activity and escalate care level as needed.
Neutral action: Run this checklist in under 20 seconds before leaving home.
Short Story: The Wednesday Hallway Test
On a wet Wednesday, a reader wrote me: “I’m fine by noon, but mornings feel like I’m walking on a boat.” She had done everything “right” except one thing—she rushed from bed to coffee, then to the garage steps, then blamed herself when her vision blurred. We rebuilt her first 20 minutes: sit first, breathe, water, stand slowly, and no staircase carrying laundry before symptoms settled.
She added a one-page log: wake time, dose time, first symptom, and how long it lasted. By day four, a clear pattern emerged: symptoms peaked within 25 minutes of her dose on low-hydration mornings. Her clinician adjusted timing and reviewed regimen fit. She didn’t need heroics. She needed sequence. The fear dropped first, then the episodes. Sometimes recovery starts with less “push through” and more choreography.
FAQ
Can blood pressure medication cause blurry vision in the morning?
It can, especially when symptoms are linked to standing quickly, dehydration, or dose timing. But persistent or sudden severe vision changes must be evaluated urgently to rule out eye or neurologic emergencies.
Is dizziness after taking BP medicine normal or dangerous?
Mild, brief dizziness can happen, particularly after dose changes. Dangerous signs include fainting, worsening instability, new neurologic symptoms, severe chest pain, or breathing distress.
Should I skip my dose if I wake up dizzy?
Do not self-adjust unless your prescriber already gave a specific plan for that scenario. Skipping or doubling can create instability. Contact your clinician promptly with symptom timing and home readings.
What blood pressure number is “too low” for me?
There is no universal single number for all adults. What matters is symptoms + trend + your medical context. If numbers are lower than usual and symptoms are significant, call your clinician the same day.
Can dehydration make BP-med side effects worse?
Yes. Lower fluid volume can worsen dizziness and orthostatic symptoms in susceptible people, especially in the morning or during illness.
Do diuretics increase risk of morning dizziness?
They can in some patients because of fluid shifts. That does not mean the medication is “wrong,” but timing, hydration strategy, and regimen fit may need adjustment.
Can I drive if my vision is blurry after medication?
No. If vision is currently blurry or you feel unstable, do not drive. Safety first. Arrange alternative transport and contact your clinician if episodes recur. For older adults who still drive, these practical guardrails for night driving after 70 and senior DMV vision renewal requirements can make planning easier.
What should I bring to my doctor appointment about side effects?
Bring a 7-day log with medication times, symptoms, posture context, hydration/meal timing, and home BP/HR readings. This often leads to faster, more precise adjustments.
Could this be an eye emergency and not a medication side effect?
Yes. Sudden vision loss, severe eye pain, persistent double vision, or neurologic symptoms require urgent or emergency evaluation. If you’re noticing blood-pressure-related retinal warning signs, this overview of hypertensive retinopathy symptoms and progression clues can help you frame better questions for your eye specialist.
How long do side effects last after a dose change?
Some effects settle over days to a few weeks, but you should not “wait it out” if symptoms are worsening, unsafe, or accompanied by red flags.
Next Step: One Concrete Action for Today
Start a 7-day morning symptom-and-BP log today. Keep it simple and time-stamped: medication, first stand, first symptom, hydration, and BP/HR readings with posture note. Then message or call your prescribing clinician and request a medication timing/dose review using your data. This one action turns vague discomfort into a fixable clinical decision.
Safety / Disclaimer (High-Risk Topic)
This article is educational and not a diagnosis. Do not stop or change prescribed blood pressure medication on your own. If you have sudden vision loss, stroke symptoms, fainting, severe chest pain, or severe breathing trouble, seek emergency care immediately.
Conclusion
Let’s close the loop from the opening scene: the blurry, unsteady morning is frightening precisely because it feels random. But it usually isn’t random. It follows a pattern—timing, posture, hydration, dose interaction, or an urgent red flag that needs fast escalation. Your job is not to become your own cardiologist before breakfast. Your job is to run a safe routine, capture clean data, and escalate at the right threshold.
Within the next 15 minutes, do three things: set out tomorrow’s water, create your log template, and save your clinician contact with “BP side effects review” in the note line. That is practical control, not panic.
Infographic: 90-Minute Morning Safety Flow
Wake → sit first → check how you feel.
Stand slowly → pause if dizzy/blurred.
Hydrate + medication per plan.
Log symptoms/BP/HR and avoid risky tasks if symptomatic.
Escalation rule: Red flags at any step → emergency care.
Last reviewed: 2026-02-10.
Medical references used for factual accuracy include current public guidance from CDC on stroke warning signs, NIH/NHLBI treatment information for hypertension medications, and major clinical resources describing orthostatic symptoms and dehydration-related dizziness.