


Protecting Your Independence: A Data-Driven Approach to Night Driving After 70
Night driving risk rarely announces itself with a dramatic moment—it usually creeps in as small failures of margin: a curb seen late, a sign that blooms into glare, a familiar turn that suddenly feels crowded and fast. If you’re wondering when to stop night driving after 70, the most useful answer isn’t a birthday cutoff. It’s a pattern you can measure.
For many older drivers, the hard part isn’t admitting change; it’s separating normal aging from actionable warning signs like worsening halos, slower glare recovery, and contrast loss at dusk. Guessing night by night feels responsible in the moment, but over time it can hide a rising crash risk.
This guide gives you a conservative, practical framework: a quick pre-drive screen, a 14-day log, and clear thresholds for when to limit, pause, or stop nighttime driving—without turning the conversation into a family power struggle.
The method is simple, repeatable, and built around real-world signals: near-miss events, lane-position uncertainty, and trend data you can bring to eye care and medication review.
Start here.
Keep your independence, but protect it with evidence.
Small adjustments now beat forced decisions later.
Let’s turn uncertainty into a safer routine.
Table of Contents
Fast Answer
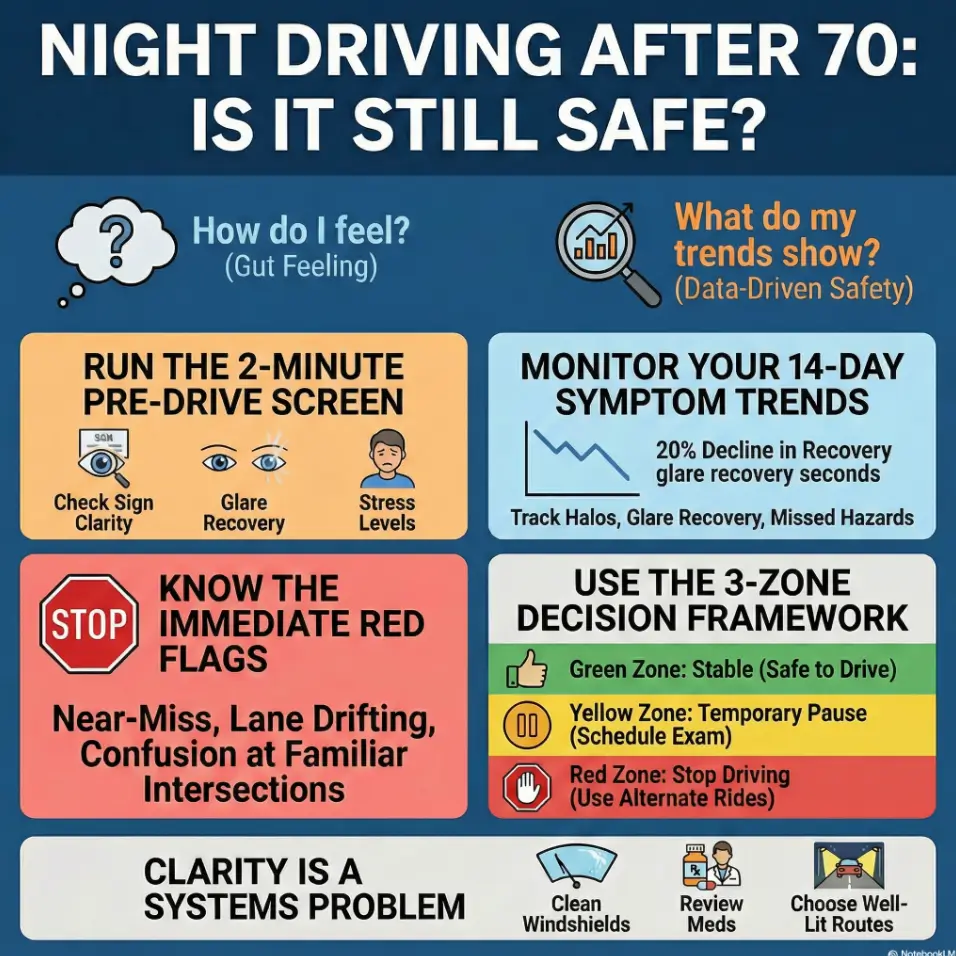
If night driving suddenly feels harder after 70—especially with halos, slow glare recovery, or trouble seeing low-contrast objects—it’s time for a structured self-check, not guesswork. Track symptoms for 2 weeks, test route-specific confidence, and use clear stop thresholds: near-misses, delayed reaction, lane-position uncertainty, or repeated confusion at familiar intersections. If red flags persist, pause night driving and schedule an eye exam plus medication review before resuming.
- One bad night can happen to anyone.
- Three worsening nights in a row is a pattern.
- A near-miss overrides all optimism.
Apply in 60 seconds: Start a note in your phone titled “Night Driving Log” with four fields: halos, glare seconds, missed hazards, stress.
Safety / Disclaimer
This article is educational, not medical or legal advice. A self-assessment helps you organize risk, but it does not replace a comprehensive eye exam, clinician guidance, pharmacist medication review, or state licensing rules. If uncertainty exists, choose the safer option and avoid night driving until you are evaluated.
I’ve watched families wait for a dramatic event before acting, because nobody wanted to “overreact.” That delay is often where risk grows. Conservative, early adjustments protect independence longer than heroic denial.
When to Seek Help Now
Red-flag signals that should end night driving immediately
- New near-miss or delayed braking in low light
- Repeated lane drift after oncoming headlights
- Missing pedestrians, curbs, cyclists, or unlit hazards
- Confusion at familiar intersections at night
- Sudden change from “manageable last week” to “unsafe this week”
Who to contact first
- Optometrist or ophthalmologist: evaluate glare disability, contrast issues, cataract/dry-eye/refractive causes
- Primary care clinician or pharmacist: review medication timing, sedating effects, interactions, glucose fluctuation risk
- Driver rehabilitation specialist (often OT-based): formal functional driving evaluation
- State DMV resources: licensing expectations and safety pathways
CDC older-driver guidance emphasizes route planning, safer conditions, and adapting habits as reflexes and processing change with age. NHTSA also highlights medication review and current prescription correction as essential safety steps, not optional extras.
Who this is for / not for
This is for
- Drivers 70+ who feel less confident at dusk or night
- Caregivers noticing new nighttime mistakes
- Anyone with halos, headlight glare, starbursts, or washed-out signs
- People who passed basic chart acuity yet still struggle on real roads
This is not for
- Emergencies: sudden vision loss, severe neurological symptoms, acute confusion
- One-article legal clearance decisions
- Situations where repeated safety incidents are being ignored
Short version: this framework helps with risk sorting, not denial. If you want a practical bridge between “I’m not ready to quit” and “I need to be safer now,” you’re in the right place.
Start here first: the 2-minute “Should I drive tonight?” screen
Three yes/no checks before you pick up the keys
- Sign clarity: Can I read reflective signs comfortably from my usual distance tonight?
- Glare recovery: After bright light exposure, does my vision reset quickly enough to feel calm?
- Body signal: Am I calm and alert, not tense, groggy, or rushed?
If any answer is “no,” downgrade tonight’s plan: delay, reroute, ride-share, or postpone.
Let’s be honest… confidence is data, not weakness
When people say, “I’m nervous at night,” families sometimes hear fear. I hear telemetry. Anxiety can be the first dashboard light—especially when tied to specific triggers like left turns across glare-heavy traffic or wet roads after dusk. Ignore ego, trust pattern recognition.
- Use the same three questions each time.
- “No” means adjust the plan, not force the trip.
- Consistency beats perfect judgment in a tired moment.
Apply in 60 seconds: Save these 3 questions as a lock-screen note.
Halos getting worse? Decode what they usually mean
Halo patterns that suggest optical vs ocular causes
- Starbursts around LEDs may point to scatter/refractive factors or surface issues.
- Diffuse glow around many light sources can track with broader optical degradation.
- One-eye-dominant symptoms can signal asymmetry worth prompt exam attention.
- Both-eye worsening may suggest systemic or shared optical factors.
The “same road, different night” clue
If the same route feels easy on Tuesday and impossible on Thursday, don’t assume “I’m just imagining it.” Dry eye, fatigue, weather moisture, and headlight scatter can stack together. If this pattern repeats, a targeted dry-eye trigger review can uncover why symptoms spike unpredictably. I once tested this on a short grocery route: after cleaning windshield interior haze plus switching departure 40 minutes earlier, discomfort dropped sharply. Same road. Same driver. Different input conditions.
NEI identifies cataract-related symptoms that map directly to nighttime complaints, including sensitivity to light and trouble seeing at night. That’s why persistent halos should be evaluated, not normalized—especially if they resemble early cataract warning patterns.
Show me the nerdy details
Visual discomfort at night is often about signal-to-noise ratio, not brightness alone. Scatter adds noise, and contrast loss reduces usable signal. The brain then spends extra cognitive energy predicting hazards, which raises fatigue and reaction variability.
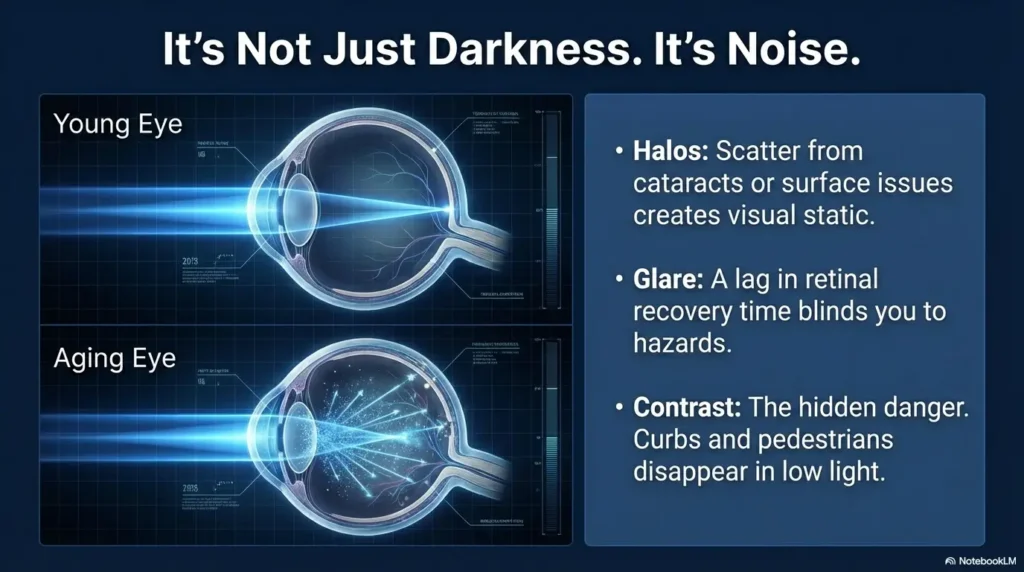
Glare recovery lag: measure your seconds, not your feelings
Simple at-home glare recovery timing method
Safety note: Do this indoors, seated, and not while driving.
- Use a dim room and a fixed low-contrast target (e.g., light gray text on darker gray card).
- Look briefly at a bright but safe light source direction (not staring directly into dangerous light).
- Start timer as you return gaze to the target.
- Stop timer when target details are comfortably readable again.
- Repeat 3 times; log median seconds.
What counts as meaningful slowdown
Don’t obsess over one off-night. Track trend and context. If median recovery time climbs across several nights—or rises alongside near-misses and stress—treat it as actionable. In operations terms: trend beats anecdote.
Many people wait for a “major scare.” I’d rather see a boring spreadsheet and no crash stories. If you want a ready template, use a printable symptom diary for seniors and keep entries consistent.
Mini Calculator: Are you trending worse?
Enter two numbers from your log:
- Week 1 median glare recovery seconds
- Week 2 median glare recovery seconds
If Week 2 is ≥20% higher and stress or missed hazards also rise, move to Yellow Zone (temporary pause + evaluation).
Neutral next step: Bring both week medians to your eye-care visit.
Contrast loss at dusk: the hidden reason curbs “disappear”
Low-contrast hazards older drivers miss first
- Dark-clothed pedestrians near unlit edges
- Faded lane lines and wet asphalt transitions
- Unlit medians and shallow curb lips
- Construction markings with poor reflective quality
Quick contrast self-checks you can repeat weekly
- Print check: Compare easy high-contrast text vs low-contrast text in consistent room lighting.
- Landmark score: On a familiar passenger-only route at dusk, score 5 fixed landmarks as clear / late / missed.
- Consistency check: Run at same time window weekly to reduce noise.
Here’s what no one tells you… bright isn’t the same as clear
More light can improve visibility up to a point, but scatter can erase detail if optical quality is poor. That’s why simply “turning everything brighter” sometimes backfires. Clarity is a systems problem: eyes, lenses, windshield, road condition, fatigue, and speed all interact. At home, many people discover similar contrast problems first in kitchens and hallways; this is why glare-controlled task lighting strategies can be unexpectedly useful training for safer nighttime visual habits.
- Track what disappears first, not just what feels bright.
- Use repeatable checks at the same time/day.
- If misses rise, reduce night exposure immediately.
Apply in 60 seconds: Pick 5 dusk landmarks and start weekly visibility scoring.
Don’t do this: 7 night-driving mistakes that raise crash risk
Common mistakes
- “I only drive nearby, so it’s fine.” (Familiarity can hide declining margin.)
- Skipping lens prescription and anti-reflective review for years.
- Driving during peak glare windows when timing could be adjusted.
- Ignoring medication timing effects (sleep meds, sedating antihistamines, mixed pain regimens).
- Overdriving headlights on darker roads.
- Dirty windshield + scratched lenses + oxidized headlights stack.
- Waiting for a major scare before changing habits.
Small confession: I used to delay windshield interior cleaning because “it looks clean enough.” Night glare said otherwise. Ten minutes of cleaning produced a dramatic difference I should not have been surprised by.
Eligibility Checklist: Should you drive tonight?
- Yes/No: No near-miss in last 14 days?
- Yes/No: Glare recovery trend stable this week?
- Yes/No: Stress score tonight ≤4/10?
- Yes/No: Route is familiar and well lit?
- Yes/No: No sedating medication effect window active?
Decision: If any answer is “No,” downgrade or defer.
Neutral next step: Re-check after rest, route change, or ride alternative.
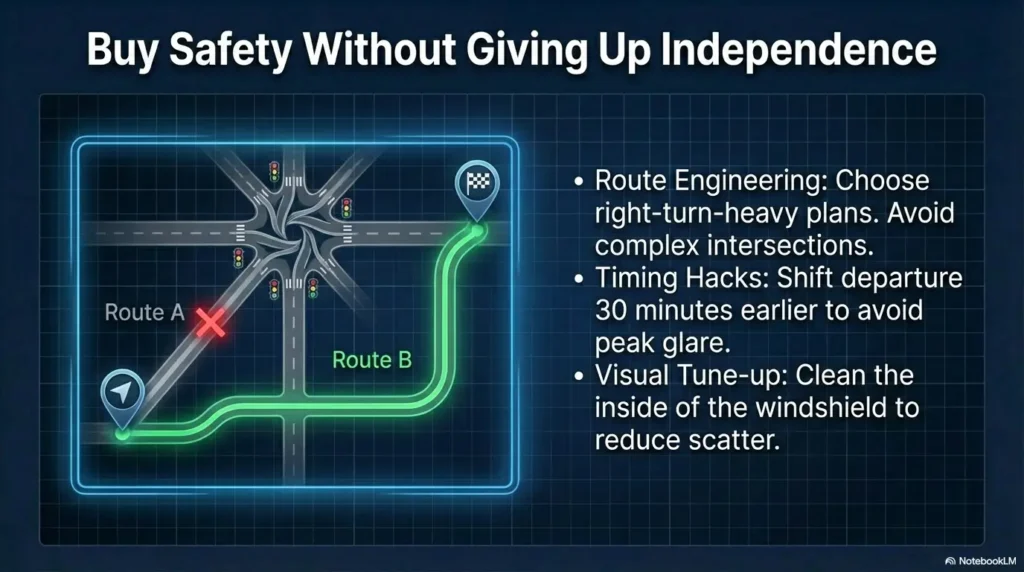
Micro-adjustments that buy safety without giving up independence
Route engineering for safer nights
- Prefer familiar, well-lit corridors over shortest-distance routes
- Use right-turn-heavy plans where feasible
- Avoid complex intersections with heavy opposing headlight glare
- Build “easy exit” points where you can stop safely if overwhelmed
Timing hacks that reduce visual load
- Shift departure 30–60 minutes earlier when possible
- Avoid peak commuting glare windows
- Keep trips short and single-purpose after dusk
Vehicle visibility tune-ups with outsized payoff
- Headlight lens restoration and alignment check
- Windshield interior/exterior deep clean
- Mirror anti-glare setup and dash brightness adjustment
- Verify wiper condition for rainy-night scatter control
NHTSA specifically advises against sunglasses or tinted lenses at night and emphasizes current prescription correction for older drivers. That simple adherence can materially improve useful vision in low light.
Show me the nerdy details
Risk reduction comes from margin stacking: lower speed + less complex route + lower glare density + cleaner optics. None is magical alone; combined they meaningfully reduce cognitive load and late hazard detection.
Open loop: Are your meds quietly sabotaging night vision?
Medication classes that can worsen night driving
- Sedating antihistamines and certain sleep aids
- Some pain medications with drowsiness or slowed reaction effects
- Anticholinergic burden that may affect focus or clarity
- Complex timing interactions across multi-drug schedules
- Glucose variability episodes causing transient blur or cognitive fog
Bring this checklist to your pharmacist
- “Night-only symptoms” log (date/time + symptoms + dose timing)
- Question 1: Which medications peak during my usual evening driving window?
- Question 2: Are there non-sedating alternatives or timing changes?
- Question 3: Any interactions likely to worsen reaction time or visual clarity?
NHTSA notes that pharmacist or clinician review of medications is a core older-driver safety step. This is practical medicine, not bureaucracy. If your regimen is already complex, a low-vision medication management checklist can make this conversation faster and safer.
Decision Card: Drive tonight vs delay
Choose A (Drive with limits) if symptom score stable, no sedating window active, and route is low complexity.
Choose B (Delay / alternate ride) if you’re within 2–4 hours of a sedating dose, stress is elevated, or glare recovery worsened this week.
Time trade-off: +20 to +40 minutes now can prevent a high-cost event later.
Neutral next step: Document your decision and discuss at the next med review.
Open loop: Is this aging—or an eye condition you can treat?
Treatable causes often mistaken for “just getting older”
- Cataract-related scatter and reduced contrast
- Uncorrected refractive shifts (including astigmatic changes)
- Ocular surface disease (dry eye) worsening night quality
- Lens coating mismatch or outdated prescriptions
Exam requests that make visits more useful
- “Please evaluate glare disability, not just chart acuity.”
- “Can we assess contrast sensitivity relevance to driving?”
- “I have a 14-day symptom log—can we review trend triggers?”
- “My goal is safe function on short evening routes; what changes are realistic?”
NEI describes cataract symptoms that align with your complaint cluster: night trouble, light sensitivity, and faded quality. Naming those symptoms clearly can accelerate practical care decisions. If cost anxiety is delaying evaluation, review what Medicare typically covers for cataract-related care in 2026 before your appointment.
Short Story: The Tuesday Grocery Route
Marian was 74 and stubborn in the most charming way. She told her daughter, “I’m fine, I just hate those new LED headlights.” Fair. But she also started missing the shallow curb by her pharmacy—same curb, three weeks in a row. Instead of declaring war over the keys, they ran a calm 14-day log. Halos rose from 3 to 7, glare recovery slowed, stress climbed, and one near-miss showed up on a rainy Thursday.
They paused night driving, saw eye care, then pharmacist, then adjusted route and timing. Her prescription changed. Dry-eye treatment started. A cataract conversation began with less fear and more clarity. Four weeks later she still limited night driving, but she regained daytime confidence and planned rides for darker trips. Nobody “won” an argument. They won a safer routine. Sometimes autonomy is not about doing everything; it’s about choosing wisely, earlier.
Decision thresholds: when to limit, pause, or stop night driving
The 3-zone framework
- No near-miss
- Stable log metrics
- Low stress, familiar route
Action: Keep restrictions + monthly reassessment.
- Worsening metrics for 3+ nights
- Glare recovery trend up
- Rising hazard misses
Action: Pause night driving + eye/med review.
- Near-miss/collision
- Lane drift with glare
- Confusion on familiar roads
Action: Stop night driving, arrange alternatives, seek formal evaluation.
Family conversation script (without power struggles)
Try this wording: “I want you safe and independent for the long run. Can we test a 14-day plan with clear metrics, then decide together?”
- Use when/where limits first (not identity labels like “you can’t drive”).
- Focus on concrete events: near-miss date, glare seconds trend, missed hazards.
- Offer alternatives immediately: ride-share credits, family rota, earlier schedule blocks.
- Zones reduce ambiguity.
- Near-miss means immediate escalation.
- Alternatives preserve dignity and compliance.
Apply in 60 seconds: Pick one sentence from the script and send it tonight.
Quote-Prep List: Before formal driving evaluation
- 14-day log printout
- Medication list with timing
- Vision prescription history
- Two recent route examples where symptoms appeared
Neutral next step: Gather these before calling a driver rehab specialist.
FAQ
1) Is night driving after 70 always unsafe?
No. Many adults over 70 drive safely at night with current vision correction, conservative route/time limits, and regular reassessment.
2) Are halos always a sign I should stop driving?
Not always. But worsening halos plus delayed glare recovery, hazard misses, or near-miss events should trigger immediate evaluation and likely temporary pause.
3) Can you pass a vision chart and still be unsafe at night?
Yes. Standard acuity can miss glare disability and contrast issues that matter in real-world night traffic.
4) Do cataracts always cause night-driving problems?
Not always, but cataracts commonly contribute to night glare and reduced visual quality. Symptom pattern and exam findings determine impact and options.
5) What medications are most likely to worsen night driving?
Any regimen causing drowsiness, slowed reaction, visual blur, or cognitive fog can raise risk. The exact effect is individual—review timing and interactions with a pharmacist or clinician.
6) Should I stop night driving after one near-miss?
At minimum, pause and review urgently. One near-miss in low light can be a serious warning, especially with concurrent symptom worsening.
7) Is anti-reflective coating enough to solve this?
It may improve comfort for some drivers, but it does not replace diagnosis, updated correction, or route/time risk controls.
8) What is the safest first restriction?
Limit to familiar, well-lit routes; avoid peak-glare windows; shorten trip duration; and avoid complex intersections when possible.
9) How often should I reassess if symptoms are present?
At least monthly, and immediately after any medication change, visual change, near-miss, or major stress/fatigue period. A practical cadence is to pair monthly checks with an annual eye exam checklist for seniors so nothing gets missed.
10) Who can perform a formal driving fitness evaluation?
A driver rehabilitation specialist, often occupational therapy-based, can conduct functional assessment and practical recommendations.
Next step: do this tonight
Open a notebook or notes app and create a 14-day Night Driving Log with four fields:
- Halos severity (0–10)
- Glare recovery time (seconds)
- Missed low-contrast hazards (count)
- Stress level before/after trip (0–10)
If any metric worsens for 3+ nights—or any near-miss occurs—move to Yellow or Red Zone immediately, pause night driving, and arrange eye plus medication review within 7 days. For readers who want a broader household plan, combine this with a nighttime home safety checklist for low vision so driving risk and fall risk are managed together.
Show me the nerdy details
Use medians rather than single values to damp random noise. Compare Week 1 vs Week 2. Couple quantitative trends (seconds, counts) with qualitative load (stress, confusion) for safer real-world decisions.
Conclusion
The real question was never “At what birthday do I stop?” It’s “When does my safety margin shrink enough that adaptation is smarter than stubbornness?” You now have a clear answer path: screen tonight, track for 14 days, act on trends, and escalate on red flags. That closes the uncertainty loop—without drama, and without gambling with someone’s life. For a broader framework, keep this page alongside your senior driving safety plan.
Your 15-minute move: set up the log now, choose one lower-risk route rule, and schedule one professional review if your recent pattern has been worsening. Independence lasts longer when decisions get earlier, clearer, and calmer.
Last reviewed: 2026-02.