

Hypertensive Retinopathy: From Diagnosis to Action
Most people hear it in the least dramatic setting: a routine eye exam, a polite tone, a printout—then the phrase lands like a dropped glass: hypertensive retinopathy.
You can walk out seeing perfectly… and still be holding evidence that your blood pressure hasn’t been as “fine” as it felt. The problem isn’t the diagnosis. It’s the fog that follows: vague urgency, scary vocabulary, and a calendar that tempts you to wait. Keep guessing and delaying, and the cost isn’t just anxiety—it’s time spent under load, when vessels don’t get a vote.
This guide turns those findings into a calm, practical plan: what the signs mean, when “same-day” is real, and what to do this week if it’s mild/moderate. It is built around the one thing clinicians can actually use: a clean 7-day home BP log you can keep in your notes app (or print).
No panic. No DIY med changes. Just traction.
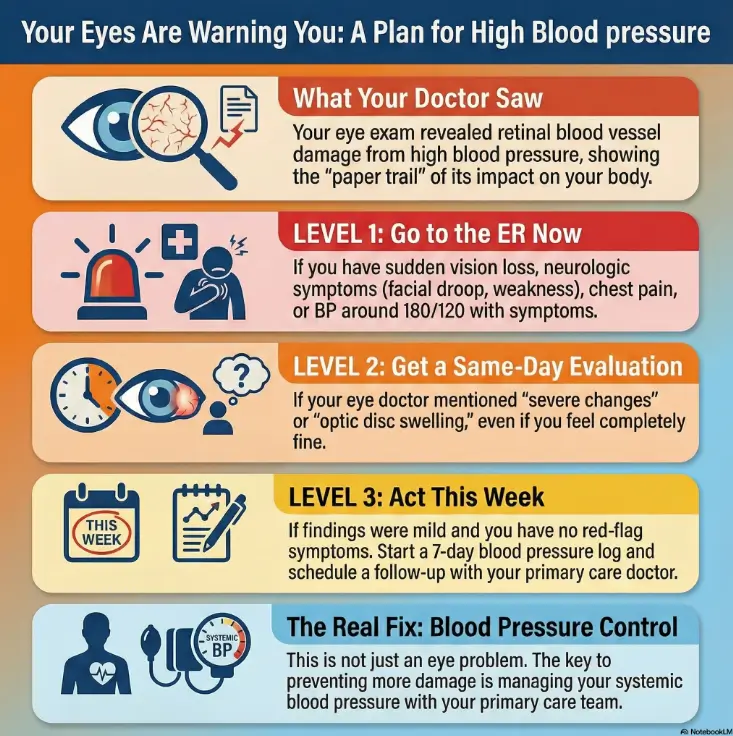
Hypertensive retinopathy is retinal blood-vessel damage from high blood pressure that an eye doctor can see during a dilated exam. Common findings include arteriolar narrowing, AV nicking, hemorrhages, cotton-wool spots, hard exudates, and in severe cases optic disc swelling. These signs can reflect cumulative hypertension damage and sometimes a hypertensive crisis—especially when BP is around ≥180/120 or symptoms are present. Your eye exam doesn’t replace a blood pressure reading, but it can reveal the “paper trail” your vessels have been leaving for a while.
Table of Contents
Hypertensive retinopathy, decoded
Let’s strip the jargon down to its moving parts. “Hypertensive” means high blood pressure. “Retinopathy” means damage in the retina—the light-sensitive tissue lining the back of your eye. Put together, hypertensive retinopathy is a visible pattern of blood-vessel stress and injury in the retina that tends to show up after blood pressure has been high long enough (or high enough) to leave marks.
Here’s the key mental model: the retina is like a transparent “window” to small blood vessels. Your doctor can’t casually look at the arteries in your brain in the exam room. But they can look at retinal vessels—often with a dilated exam, sometimes with photos. (If you’re overdue for one, this guide on how often seniors should get dilated eye exams helps you pick a reasonable baseline.)
What it is: evidence of how your small vessels have been behaving under pressure.
What it isn’t: a precise number for your current blood pressure, a guaranteed prediction of your future, or a reason to DIY medication changes.
I learned this the awkward way: years ago, I ignored “borderline” BP because I felt great. My only symptom was… being busy. When a clinician finally asked for a home BP log, I realized my “normal” days had been doing quiet damage. Hypertensive retinopathy is that kind of receipt. Not a sentence. A receipt.
- It reflects vessel stress over time (or sudden severe spikes).
- It doesn’t tell your exact BP at this moment.
- It is a strong reason to tighten control and follow through.
Apply in 60 seconds: Put “bring eye exam note” as a calendar task for your next primary care visit.
Urgency first: when this is an emergency
Before we translate any retina vocabulary, we do the grown-up thing first: triage. Because the cost of underreacting can be real, and the cost of overreacting is… an annoying bill and a long wait (still better than a stroke).
Safety / Disclaimer (read this)
This article is for education—not diagnosis or treatment. If you have sudden vision loss, a severe headache, chest pain, shortness of breath, new weakness/numbness, confusion, or you’ve measured blood pressure around 180/120 with symptoms, seek urgent care. Many U.S. clinicians and major medical organizations discuss 180/120 as a threshold that can indicate a hypertensive crisis, especially with symptoms. If you’re unsure what counts as “serious,” this quick explainer on when eye symptoms aren’t “just aging” can help you sanity-check.
ER-now red flags (vision + neuro + chest + breathing)
- Vision: sudden loss of vision, a curtain/shadow, new severe blurring, or flashing lights paired with concerning symptoms.
- Neurologic: facial droop, slurred speech, one-sided weakness, confusion, severe “worst” headache.
- Cardiopulmonary: chest pressure, severe shortness of breath, fainting, new severe swelling.
- Pregnancy/postpartum: vision changes + high BP should be treated as urgent.
Same-day vs 24–48h: what “severe changes” can imply
If your eye doctor used words like “severe,” “grade 3/4,” “optic disc swelling,” “papilledema,” or urged immediate BP evaluation, don’t negotiate with that advice. Same-day evaluation can be appropriate even if you feel okay—because severe hypertension can be sneaky until it isn’t.
Let’s be honest…
If you’re Googling this at 2 a.m., you’re not looking for a philosophy lecture. You want to know whether to sleep, drive, or call someone. If you have red-flag symptoms or truly scary readings, go in. If you don’t, you still deserve a clear next-day plan—which we’ll build below.
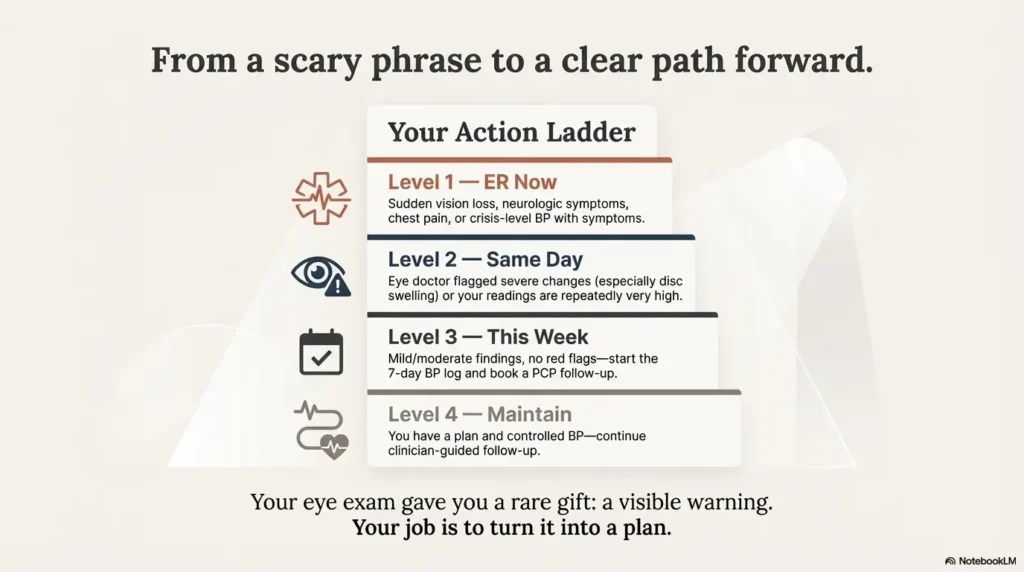
- Yes if you have red-flag symptoms (vision loss, neuro signs, chest pain, severe shortness of breath).
- Yes if BP is around 180/120 and you feel unwell (headache, confusion, chest pain, breathlessness).
- Yes if your eye doctor flagged optic disc swelling or “malignant” changes.
- No doesn’t mean “ignore.” It means “act this week with a plan.”
Neutral next step: If unsure, call your clinician’s after-hours line or urgent care for guidance.
Eye exam signs: what your doctor saw
This is the section people wish their eye doctor had time to narrate like a sports commentator. What follows is a translation layer—no drama, no false certainty.
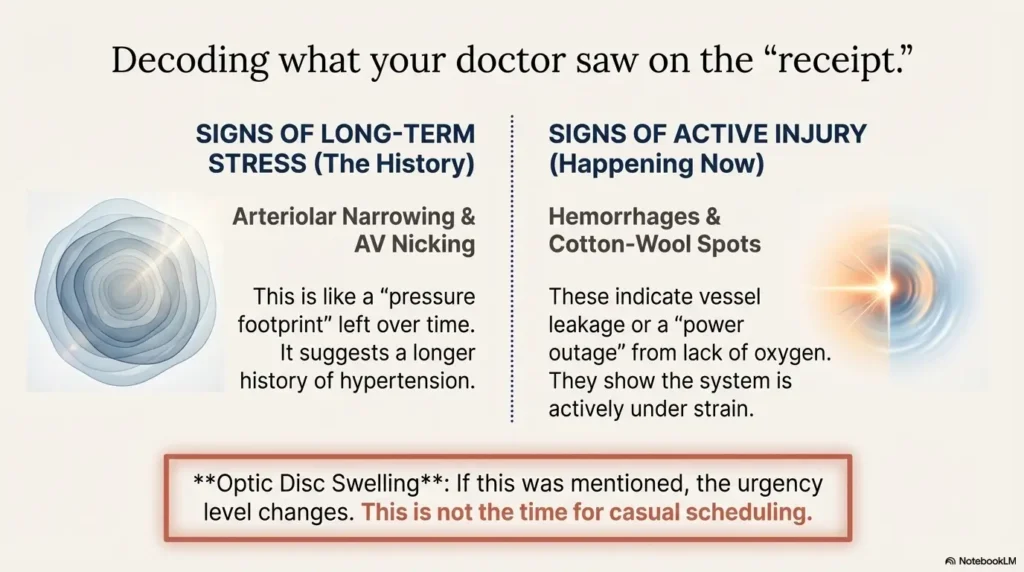
- Some changes suggest chronic pressure.
- Some suggest active injury/leakage.
- Disc swelling shifts the urgency conversation.
Apply in 60 seconds: Ask for a copy of your retinal photos or imaging summary (portal message works).
Arteriolar narrowing: the “pressure footprint” over time
Retinal arterioles may narrow in response to sustained high pressure. Think of it as a long-term stress posture: vessels adapt, stiffen, and the caliber changes. This tends to be a “history” finding—useful as a warning sign, not a timer counting down.
AV nicking: when arteries squeeze veins at crossings
At places where an artery crosses a vein, chronic arterial wall thickening can compress the vein. The term sounds like a harmless nickname; it isn’t. It suggests longer-term hypertension effects on vessel walls.
Hemorrhages: when leakage becomes visible
Retinal hemorrhages can appear in particular shapes and layers. You don’t need to memorize them. You need to know the message: bleeding means vessel integrity has been compromised. That can happen with significant hypertension, and it can overlap with other causes—another reason not to self-diagnose from one word in a note.
Cotton-wool spots: tiny nerve “power outages” (ischemia)
Cotton-wool spots are small areas where nerve fibers aren’t getting enough oxygenated blood—like a brief brownout. They often show up in more advanced hypertensive retinopathy and in other conditions too. The practical meaning is: your retina has been asking for more blood flow than your vessels were delivering.
Hard exudates / macular star: leakage near vision-critical zones
Hard exudates are lipid/protein deposits left behind after leakage. When they gather in certain patterns (including around the macula), they can threaten central vision. This is one reason your doctor might talk about closer follow-up even if your current vision feels “fine.” (If you’re trying to separate “retina swelling” language from everything else, this diabetic macular edema symptoms guide can help you decode macula-centered warning terms, even when diabetes isn’t the main story.)
Optic disc swelling: the finding that changes urgency
Optic disc swelling (sometimes discussed alongside “papilledema,” depending on context) is a serious finding. It can be associated with dangerously high blood pressure and other urgent neurologic issues. If this was mentioned, it’s not the time for casual scheduling.
Here’s what no one tells you…
Clinicians sometimes say “mild” to avoid scaring you. Patients hear “mild” and file it under “ignore.” A better translation is: mild can still be meaningful—because it’s an early receipt, not a final invoice.
Show me the nerdy details
Ophthalmology references often describe hypertensive retinopathy through vessel caliber changes (arteriolar narrowing), arteriovenous crossing changes (AV nicking), and signs of retinal ischemia/leakage (cotton-wool spots, hemorrhages, exudates). The “why” is a mix of acute vasoconstriction and longer-term vascular remodeling. The more severe patterns are the ones that push urgency—especially when optic disc changes enter the picture.
Stages & grades: what the severity labels really mean
Different clinicians use different grading schemes. The point isn’t to win a trivia night. The point is to understand the practical bucket you’re in: early vessel changes vs active injury vs possible emergency.
Two timelines: chronic damage vs acute crisis patterns
Hypertensive retinopathy is one condition with two common stories:
- Chronic story: years of imperfect control gradually change vessel walls and caliber.
- Acute story: a spike (sometimes severe) triggers hemorrhages, cotton-wool spots, and more dramatic findings.
Common grading approaches (what you’ll see in notes)
Some notes describe “grade 1–4” or similar. Others list specific signs. If you see a grade, ask what that means for you in one sentence: “Does this require same-day BP evaluation?” That’s the question that cuts through grading differences.
The open-loop: “Can the eye findings tell my exact BP?”
No. Not precisely. Your retina can show patterns consistent with hypertension and severity trends, but it can’t hand you a number the way a cuff can. What it can do—powerfully—is tell you: “This isn’t hypothetical anymore.”
Choose the ‘urgent’ path if any of these are true: disc swelling/papilledema was mentioned, you have new neuro symptoms, chest pain, severe headache, or your home readings are consistently near crisis levels.
Choose the ‘tighten control’ path if: findings were described as mild/moderate, you have no red-flag symptoms, and your readings are elevated but not crisis-level—yet you still need a near-term plan and follow-up.
Neutral next step: Ask your eye clinic for the exact wording of the finding and recommended timeframe.
Why your vision can be “fine” (and still risky)
This is the emotional core of the whole topic: how can something be wrong if I can see? Because your retina is resilient—until it isn’t. Many people don’t experience noticeable symptoms early on. Your eye exam catches the quiet changes first.
I’ve watched friends treat blood pressure like a mood: “I’m calm, so I’m fine.” But hypertension is more like gravity. It does what it does, even on cheerful days.
Late symptoms are common—even as changes progress
Symptoms tend to show up late or intermittently—blur that comes and goes, trouble focusing, or headaches that aren’t obviously “eye-related.” That’s why clinicians stress monitoring and control even when you feel normal.
What eye findings can signal about your broader risk
In many clinical discussions, hypertensive retinopathy is treated as a marker of small-vessel stress. In plain language: if the small vessels in your eyes are showing strain, it’s a nudge to treat your cardiovascular risk seriously. It doesn’t mean disaster is imminent. It means prevention is suddenly a lot less theoretical. (If you’re in your 60s or beyond, it’s also worth skimming common age-related eye diseases after 60 so you can separate “BP-related” from “age-related” conversations without spiraling.)
Show me the nerdy details
Retinal microvascular changes are sometimes discussed as correlates of systemic vascular health because the retina is one of the few places clinicians can directly visualize small vessels. That’s why hypertensive retinopathy is often framed as more than “an eye finding”—it can be a proxy signal for broader microvascular burden.
Look-alikes: hypertensive vs diabetic retinopathy
Hypertensive retinopathy isn’t the only condition that can cause retinal hemorrhages, exudates, or cotton-wool spots. Diabetes is a major look-alike in the U.S., and many people have both hypertension and diabetes—so the clean separation people want isn’t always real life.
When both can be true (common U.S. overlap)
If you have diabetes (or prediabetes), the “which one is it?” question becomes “how much of each is contributing?” This matters because follow-up cadence and additional testing can change based on combined risk. If you need a clean baseline on what diabetes-related findings typically include, start with this plain-English overview of diabetic retinopathy.
Screening mindset: diabetes tends to come with structured eye screening language
Diabetic retinopathy guidance often emphasizes regular retinal screening. Hypertensive retinopathy discussions are more likely to focus on BP control and systemic evaluation. If your note seems to mix terms, it’s worth a clarifying call: “Was this hypertensive changes, diabetic changes, or both?” If you’re also navigating insurance logistics, this post on Medicare diabetic eye exam cost and how to book an annual screening can reduce the friction that makes people “wait until later.”
- Hypertension and diabetes often overlap.
- Similar findings can have different drivers.
- Clarify the cause before you assume the plan.
Apply in 60 seconds: If you don’t know your last A1C, write it down as a question for your next visit.
Common mistakes after a scary eye exam
Here’s the part where I play the slightly annoying friend who cares about you: most bad outcomes come from boring mistakes, not dramatic ones.
Mistake: treating it as “just an eye problem”
Hypertensive retinopathy is an eye finding, but the lever that changes the outcome is usually systemic blood pressure control. That means primary care, cardiology, and lifestyle realities—not just a return visit to the eye clinic.
Mistake: stopping meds or “resetting” without guidance
It’s tempting to experiment when you’re scared or frustrated. Don’t. Medication changes should be clinician-guided, especially if your readings are high or you have symptoms.
Mistake: relying on one-off readings (and calling that “monitoring”)
A single calm reading at a pharmacy kiosk can be a soothing lie. Clinicians make better decisions with patterns: consistent technique, multiple readings, and context.
Mistake: assuming “white coat” explains everything
White coat hypertension is real, but it’s not a hall pass. If your retina is showing changes, you still need a disciplined plan to confirm your true baseline.
- Your eye exam note (exact words) and any retinal photos or imaging summary.
- A 7-day home BP log (AM/PM, two readings each time).
- Medication list + doses + what you actually take (yes, including missed doses).
- Symptoms timeline (headache, vision changes, chest symptoms, pregnancy/postpartum status).
Neutral next step: Put these into one folder (paper or phone) before your next appointment.
Don’t do this: the 7-day trap
The week after a scary finding is when people accidentally sabotage themselves. Not because they’re careless—because they’re human. Here’s what to avoid.
Don’t “wait for the next annual exam” if severe findings were mentioned
If your clinician flagged severe changes or urgent evaluation, treat that timeframe as real. Delays don’t help a vessel heal. They just extend the time under load.
Don’t downgrade symptoms because the visit was “routine”
Routine visits discover non-routine problems. If you develop new symptoms after the exam—especially neurologic or chest symptoms—take them seriously.
Don’t treat 180/120 as “a number to sleep on”
In U.S. clinical guidance discussions, BP around 180/120 is often used as a crisis threshold—especially with symptoms. If your readings are there and you feel unwell, that’s not a “maybe tomorrow” situation.
Don’t buy a cuff and assume it’s accurate forever
Home cuffs can be excellent tools, but technique matters: correct cuff size, arm position, rest time, and consistent timing. Otherwise you’ll collect data that looks impressive and helps no one.
Quick confession: the first time I used a home cuff, I measured after climbing stairs and mentally rehearsing an argument. My numbers were… dramatic. The cuff wasn’t wrong. My technique was. Fix the method before you judge the body.
Diagnosis: what clinicians confirm
In most standard medical descriptions, hypertensive retinopathy is diagnosed through history plus fundus exam findings. In real-world care, that expands into a bigger question: how controlled is your blood pressure, really?
Fundus exam + history are central
Eye clinicians look at vessel caliber, crossing changes, and evidence of leakage/ischemia. They also consider your BP history, other risk factors, and whether another condition could be contributing.
Why clinicians ask about duration, control, and adherence
Hypertension isn’t a single event—it’s an exposure over time. Duration matters. Variability matters. Medication adherence matters. If your eye findings are concerning, your care team may evaluate for other end-organ stress (kidneys, heart) depending on the situation. If you have a strong family pattern of eye or vascular disease, it can help to bring that up explicitly—this family history of eye disease checklist makes it easier to summarize without rambling.
Show me the nerdy details
Clinicians sometimes describe hypertensive retinopathy through stages that reflect chronic arteriolar changes and more acute exudative/hemorrhagic findings. The practical point for patients: if the pattern suggests acute injury, it often triggers faster systemic evaluation.
Short Story: The “I’m fine” week that wasn’t fine (120–180 words) …
Short Story: A friend of mine—smart, stubborn, always “too busy”—went for new glasses and came home with retinal photos. The optometrist used gentle words: “some hypertensive changes.” My friend laughed it off. No symptoms. Great energy. He promised to “get around to it” after a work deadline. Three days later, he woke with a pounding headache and the kind of dizziness that makes the hallway tilt.
He finally checked his blood pressure at a pharmacy, then checked it again because he didn’t believe the first number. It was high enough that the urgent care receptionist didn’t hand him forms; she walked him back. He was okay in the end—because he went in. But he told me later the scariest part wasn’t the symptoms. It was realizing his body had been warning him quietly, and he’d trained himself not to listen.
Treatment: what actually changes the outcome
Most hypertensive retinopathy management comes down to the least glamorous phrase in medicine: blood pressure control. It’s not a single heroic act. It’s a set of small, repeatable behaviors plus the right medication plan for your body.
The core: long-term blood pressure control
U.S. organizations like the American Heart Association emphasize consistent BP control strategies—home monitoring when appropriate, medication adherence, and addressing lifestyle contributors. The retina doesn’t need perfect. It needs lower and steadier. (For older adults juggling multiple eye risks, it can be grounding to read this piece on blindness risk after 70 and what actually moves the needle—it keeps “fear headlines” from running your plan.)
When eye-directed treatment enters the chat
If complications like macular involvement or significant swelling are present, your eye specialist may discuss additional imaging or treatment options. That conversation is individualized—based on what’s happening near the macula (central vision) and whether other retinal conditions are involved.
Follow-up expectations (why rechecks matter)
Follow-up is where improvement becomes visible. Even if changes don’t fully reverse, stabilization is a win. Think of it like stopping a leak: the goal is to prevent more damage and protect function.
Next step: the one action that reduces uncertainty
If you do only one thing after reading this, do this: create a BP record your clinician can actually use. Not a vibe. Not a memory. A clean log.
7-day home BP log (simple, clinician-friendly)
- Measure morning and evening for 7 days.
- Each time, take two readings, one minute apart, seated and rested.
- Write down: date/time, readings, meds taken, and any symptoms (headache, vision changes, chest symptoms).
Input (max 3): (1) Your average AM systolic, (2) your average PM systolic, (3) number of days logged.
Output: If your PM average is lower than AM and both are improving week-to-week, you’re likely stabilizing. If either average remains near crisis levels or spikes with symptoms, escalate care.
Neutral next step: Bring the averages (and the raw readings) to your clinician rather than guessing alone.
Copy/paste message to your primary care office
Message template: “My dilated eye exam noted hypertensive retinopathy findings. I’m attaching the eye note/photos and a 7-day home BP log (AM/PM, two readings each). Please advise whether this needs urgent evaluation and what follow-up you recommend.”
Close the loop: the question from the hook
Why would your retina show damage when you feel okay? Because hypertension often harms quietly. The fix isn’t fear. It’s follow-through: confirm your real BP pattern, tighten control, and recheck the eyes on a clinician-recommended timeline.
FAQ
Can an eye exam show uncontrolled high blood pressure?
An eye exam can show signs consistent with hypertension (like arteriolar narrowing or hemorrhages), but it can’t give your exact BP number. Think of it as evidence of vessel stress that should prompt proper BP measurement and follow-up. If you’re building a “bring-to-the-visit” checklist, this annual eye exam checklist for seniors pairs well with the BP log idea.
What does arteriolar narrowing mean on an eye exam?
It often suggests longer-term vessel response to higher pressure—more of a “history” clue than an emergency sign by itself. The next step is confirming your BP pattern and tightening control.
What do cotton-wool spots mean with high blood pressure?
Cotton-wool spots can indicate retinal ischemia (reduced blood flow to nerve fibers). They can occur with more advanced hypertension and also with other conditions, so clinicians interpret them in context.
Is hypertensive retinopathy an emergency?
Sometimes. Severe findings (especially optic disc swelling) or hypertensive crisis-level readings with symptoms can require urgent evaluation. Mild findings usually mean “act soon and tighten control,” not “panic”—but don’t ignore them.
What blood pressure numbers define a hypertensive crisis?
Many U.S. medical resources discuss readings around 180/120 as a crisis threshold—particularly when symptoms are present. If you’re at or above that level and feel unwell, seek urgent care.
Does hypertensive retinopathy go away after BP is controlled?
Some findings can improve, and many can stabilize with good BP control. Other changes may not fully reverse, especially if they reflect long-term vessel remodeling. The win is preventing progression and protecting vision.
How often should I get a dilated eye exam if I have hypertension?
It depends on severity and other risk factors (like diabetes). If hypertensive retinopathy was found, ask your eye clinician for a specific follow-up interval rather than guessing.
Do I need a cardiologist if my eye doctor found hypertensive changes?
Not always, but sometimes. Many people start with primary care. Referral to cardiology can make sense if BP is difficult to control, very high, associated with symptoms, or complicated by other conditions.
Conclusion
Hypertensive retinopathy is one of those diagnoses that feels unfair because it arrives quietly—often in a room where you expected nothing more than “read the bottom line.” But it’s also a rare gift: a visible warning before something irreversible happens. Your job isn’t to become an ophthalmologist overnight. Your job is to turn a scary phrase into a clean next step: a real BP log, a timely clinician conversation, and a plan you can execute on busy days.
Your 15-minute CTA: open your notes app and create a simple table for the next 7 days: AM reading 1, AM reading 2, PM reading 1, PM reading 2, symptoms. Then message your primary care office using the template above. That’s how you turn an eye finding into a prevention plan.
Last reviewed: 2025-12-26