


The Blur Isn’t Just Aging—It’s a Pattern
By 7 p.m., the words on your screen can look lightly smeared, then snap back after a few blinks, then blur again by bedtime. That pattern is often medication-related dry eye, not “just aging,” and it becomes far more common after 60 when multiple prescriptions, OTC products, and indoor habits start stacking their effects.
The hard part is that fuzzy sight feels random when it is actually patterned. Miss those patterns, and you risk months of avoidable discomfort, shaky night-driving confidence, and delayed care while the real contributors keep piling up.
This guide helps you sort signal from noise with a safer, practical method: identify likely medication groups, map symptom timing, and prepare a focused medication review plus eye-surface exam without risky self-experiments.
You will also see how polypharmacy, tear film instability, preservative-free tears, and everyday factors like screen time, heat, and CPAP leak can combine into one confusing blur story. The approach is grounded in a clinic-style workflow: track first, de-risk second, coordinate care third.
Start here. Because clarity usually returns in steps, not miracles.
Table of Contents
First clue, not first panic: when “fuzzy” points to dry eye
The symptom pattern that fits medication-related dryness
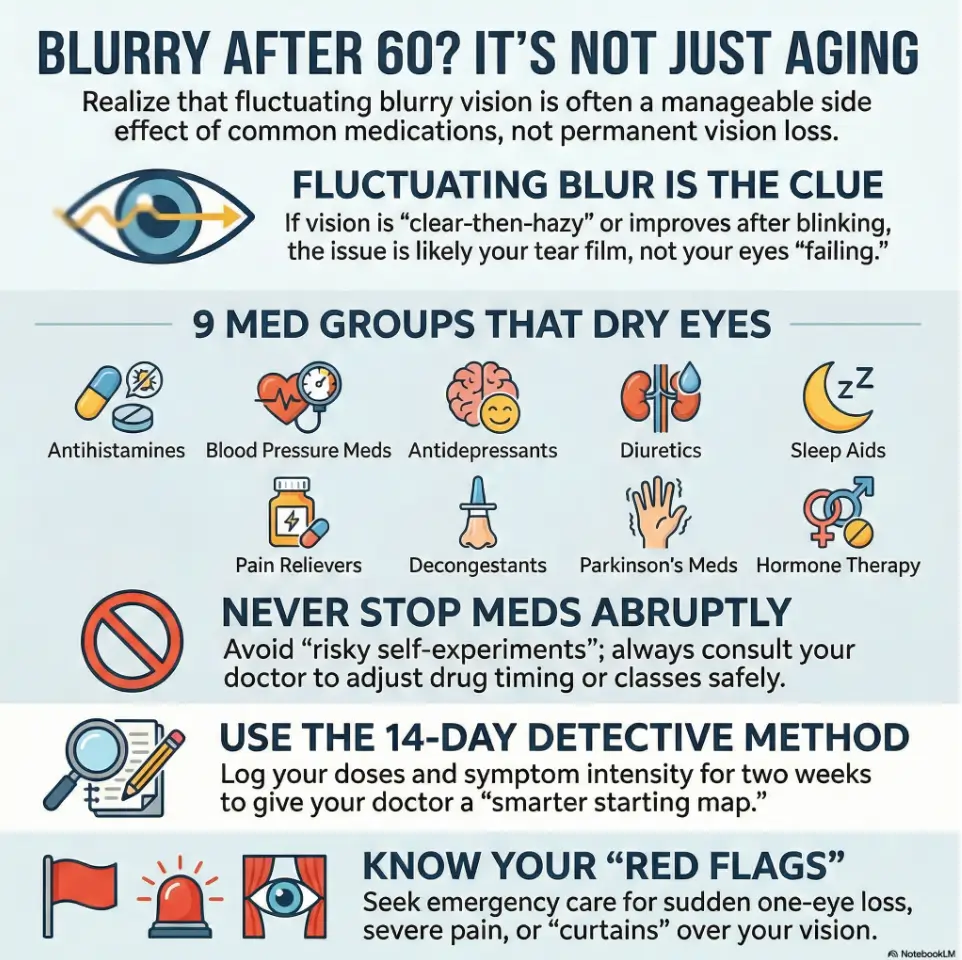
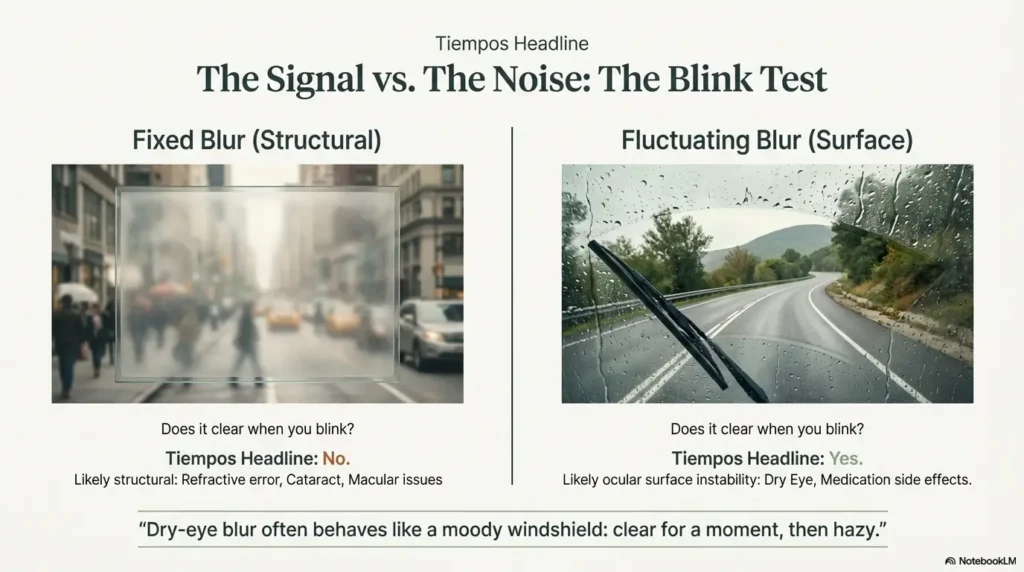
Dry-eye blur often behaves like a moody windshield: clear for a moment, then hazy, then better again after blinking. That fluctuation matters. People describe it as “soft focus,” “ghosting,” or “I can read, then suddenly I can’t.” The National Eye Institute and major eye centers consistently note that dry eye can cause both discomfort and visual disturbance, not just gritty eyes. If your symptoms include burning, foreign-body sensation, light sensitivity, or watery reflex tearing, dry eye becomes a strong suspect. If this sounds familiar during reading-heavy hours, compare your pattern with this guide on dry eyes from reading and this late-day profile of 3 p.m. burning eyes.
In clinic-style language: symptoms that vary across the day often point to ocular surface instability, while fixed blur all day may push us to consider refractive error, cataract, macular disease, or neurologic causes.
Morning blur vs evening blur—what timing can reveal
Morning-heavy blur can suggest overnight dryness, incomplete lid closure, or CPAP airflow leak toward the eyes. Evening-heavy blur may reflect screen time, indoor heat, lower blink rate, cumulative tear evaporation, and medication peaks. I once tracked my own evening eye fatigue during a winter deadline sprint: same glasses, same monitor, but by 8 p.m. letters looked like they were wearing little halos. The fix wasn’t heroic, short blink breaks, humidity, preservative-free tears, and better lamp placement. If your mornings are consistently worse, this checklist for waking up with blurry vision and this CPAP-specific breakdown on mask leak into the eyes can help you prepare better questions for clinic day.
Timing won’t diagnose you. But it gives your clinician a smarter starting map.
Let’s be honest… “I thought it was just aging”
Most people wait too long because “aging” sounds tidy. Reality is messier: age changes tear quantity and quality, and medicines can amplify the stress. So yes, age matters. But age plus medication burden plus environment is usually the more truthful equation.
- Notice whether blur improves after blinking
- Track time-of-day pattern (morning vs evening)
- Write down two trigger settings (screens, heat, wind)
Apply in 60 seconds: Put “Does blur change after blinking?” in your phone notes right now.
The 9 medication groups most linked to dry eye and blurry vision
Think of this as a probability list, not a verdict list. A medication can contribute without being the only cause.
Antihistamines and decongestants (allergy/cold meds)
These are classic drying agents. They can reduce watery secretions broadly, including the tear film. In real life: symptoms often worsen during allergy season or when nighttime cold meds become a daily habit. Many people notice “clear nose, dry eyes” within days. If you use OTC allergy products regularly, this comparison of dry-eye effects across Claritin, Zyrtec, and Allegra is worth reviewing.
Antidepressants (especially anticholinergic effects)
Some antidepressants and related psychiatric meds can reduce tear production or alter focusing comfort. Not everyone is affected, and mental-health stability is non-negotiable, so this is a “discuss and optimize,” never “panic and stop” category.
Blood pressure meds (including some beta blockers)
Certain antihypertensives are associated with ocular dryness in some patients. Blood pressure control remains critical, but if blur rose after a dose change, your prescribing clinician may be able to adjust class, timing, or companion strategies. For a focused medication-side-effect pathway, see blood pressure medication, dizziness, and blurry vision.
Diuretics (“water pills”)
Diuretics can contribute to dehydration and worsen dryness. It’s not only about total water intake, it’s also about fluid timing, comorbid disease, and indoor environment.
Hormone-related meds (including HRT and some birth control)
Hormonal shifts affect meibomian gland and tear dynamics. After menopause, this becomes especially relevant. Hormonal therapy decisions need broader risk-benefit context, so avoid all-or-nothing thinking.
Acne meds and retinoid-related exposure
Systemic retinoid exposure is well known for mucosal dryness, including eyes. Even past history can matter if gland function remains fragile.
Parkinson’s disease medications
Parkinson’s itself can alter blink rate and ocular surface function; medication effects can overlap. This is the textbook definition of “stacked causes.”
Sleep/anxiety meds with drying side effects
Sedating agents can change blink behavior and surface lubrication overnight. If morning irritation is strong, this bucket deserves a careful review.
Chronic eye drops with preservatives (including some glaucoma drops)
Long-term exposure to preserved drops can irritate the ocular surface in susceptible eyes. For many people, preservative-free alternatives or regimen changes help without compromising pressure control. If you are juggling pressure control and tolerability, this can pair well with glaucoma eye drop side effects in seniors and practical options for preservative-free eye drops for seniors.
- Count prescriptions + OTC products + supplements
- Mark any medication started or dose-changed in the last 8 weeks
- Flag all nighttime products
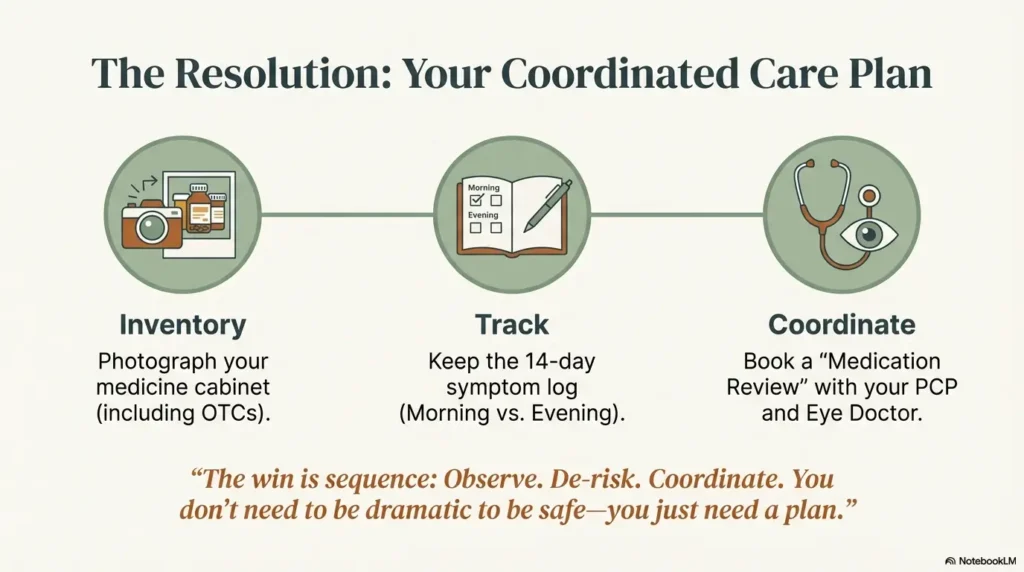
Apply in 60 seconds: Open your medicine cabinet and snap one inventory photo.
Why this happens after 60: tears, glands, and polypharmacy
Tear production drops with age
As we age, both tear quantity and tear quality can shift. Oil layer function may weaken, evaporation rises, and the surface becomes less forgiving. So the same medication that felt fine at 45 can feel very different at 67.
More meds, more interactions, more ocular surface stress
Polypharmacy isn’t a moral failure; it’s often appropriate chronic-care medicine. But each added drug can nudge dryness risk, focus comfort, sleep pattern, hydration status, or inflammation. The effect can be additive, sometimes multiplicative. I’ve seen readers describe this perfectly: “No single med wrecked me. The pileup did.”
Hidden multiplier: low humidity, screens, CPAP, and indoor heat
Environment often acts like an amplifier. Heated indoor air, winter wind, ceiling fans, and long screen sessions reduce blink completeness. CPAP leaks aimed at the eyes can make mornings rough. If your symptoms change by room, device, or season, that is useful diagnostic information. You may also benefit from this practical routine for a 15-minute night routine for dry eyes and this broader guide on digital eye strain in seniors.
Commercial entities worth knowing in this space include the National Eye Institute (NIH), the American Academy of Ophthalmology, and major health systems like Mayo Clinic. They all emphasize that dry eye can blur vision and that medication and environment are common contributors.
Show me the nerdy details
The tear film has multiple interacting layers (lipid, aqueous, mucin). Medication effects can reduce secretion volume, alter gland output, or increase evaporation indirectly through behavior (blink suppression, sleep architecture changes). In practice, clinicians often treat both “supply” and “evaporation” simultaneously because mixed-mechanism dry eye is common in older adults.
Eligibility checklist: Is a medication review likely to help?
- Yes/No: Age 60+ with new or worsening blur in last 3 months
- Yes/No: Taking 2 or more daily prescriptions
- Yes/No: Also using OTC allergy/cold/sleep products
- Yes/No: Symptoms fluctuate by time of day
- Yes/No: Eye irritation improves briefly after blinking/tears
Neutral next step: If you checked 3+ “Yes,” schedule a combined medication review + eye-surface exam.
Open loop: “Which one is doing this to me?” A practical detective method
Build a 14-day symptom + dose timeline
Don’t guess from memory. Use a simple two-column log: medication timing and symptom intensity. Include blur, burning, foreign-body feeling, light sensitivity, and night-driving confidence (0 to 10 scale). In 14 days, patterns often emerge that one office visit can act on quickly. If you want a ready template, use this printable symptom diary for seniors.
Spot the dose-response signal without self-experimenting dangerously
The safe method is observational, not improvisational. You’re watching correlations: symptom spikes 2 to 6 hours after specific doses, worse after PRN antihistamines, better on low-screen days, etc. Avoid “trial stops” of blood pressure, mood, Parkinson’s, or glaucoma medications without medical supervision.
Bring this one-page log to your next visit
When clinicians see data, the conversation shifts from vague discomfort to targeted decisions. One reader told me her appointment went from “come back later” to a same-day plan after she brought a one-page timeline and a full OTC list. The visit lasted 18 minutes. The uncertainty dropped by half.
Mini calculator: Should you fast-track your appointment?
Input 1: Worst blur score this week (0–10)
Input 2: Night-driving confidence drop (0–10)
Input 3: Number of “new or changed” meds in last 8 weeks
Quick output: If (Input1 + Input2 + Input3) ≥ 14, move from “routine” to “soon” (within days), unless emergency signs are present.
Neutral next step: Call and request a medication-related vision review slot.
Don’t do this: 5 common mistakes that prolong blurry vision
Stopping blood pressure or mood meds abruptly
This creates a safety risk that usually outweighs any short-term eye benefit. Your job is to report patterns; your clinician’s job is safe medication architecture.
Using “get-the-red-out” drops daily
Vasoconstrictor redness relievers can irritate some eyes with daily use. Many clinicians prefer lubricating tears, especially preservative-free options for frequent use.
Treating every blur as a glasses problem
New glasses can help refractive blur, but they won’t fix unstable tear film alone. If letters sharpen after blinking and then smear again, think surface first.
Ignoring nighttime driving changes
Night blur is a functional safety metric. If road signs bloom, halos worsen, or lane contrast drops, act early. Don’t let pride drive the schedule. If you need a practical self-check framework, see night driving after 70 and this broader senior driving safety guide.
Waiting months before a medication review
Delay turns a reversible process into a chronic routine. You don’t need panic. You need tempo.
- Don’t self-stop essential meds
- Don’t rely on redness drops as daily strategy
- Don’t postpone a medication reconciliation
Apply in 60 seconds: Put “night-driving changes” on your symptom tracker as its own line item.
Who this is for / not for
For: adults 60+, caregivers, and patients on 2+ chronic meds
If you (or someone you care for) are juggling chronic conditions and eye symptoms, this framework is built for you. It works especially well when time is tight and appointments feel fragmented between PCP, specialist, and eye clinic.
Not for: sudden one-eye vision loss, severe pain, flashes/floaters, trauma (urgent care needed)
These are not “wait and see” symptoms. Sudden visual field curtain, abrupt one-eye vision drop, severe pain, neurologic symptoms, or new flashes/floaters need same-day emergency evaluation.
Decision card: PCP first vs eye specialist first
Choose PCP first when medication changes are recent and symptoms are gradual, bilateral, and fluctuate.
Choose ophthalmology/optometry first when visual function is dropping, night driving worsens, or diagnosis is uncertain.
Choose emergency care now for sudden loss, severe pain, curtain/shadow, acute neurologic symptoms.
Neutral next step: Pick one lane today and book it before bedtime.
Open loop: Could this be cataract, macular disease, or dry eye—or all three?
Overlap symptoms that confuse people
Dry eye, cataract, and macular disease can all present as blur. That overlap is why self-diagnosis feels impossible. Cataract often brings glare/halos and gradual decline; dry eye often fluctuates; macular disease can affect central clarity and distortion. But real patients rarely read like textbooks. If you notice strong night glare patterns, this companion piece on macular degeneration and night driving safety may help you separate concerns before your visit.
The “stacked causes” problem in real clinic visits
Many people over 60 have layered causes: mild cataract + dry eye + medication effects + screen fatigue. I remember one caregiver telling me, “We kept searching for the one villain.” The breakthrough came when the care team treated it as a stack instead of a mystery novel twist.
What no single symptom can diagnose
No single home clue can rule in or out retinal disease, glaucoma progression, or neurologic causes. That’s why comprehensive eye exams matter: surface assessment, refraction, pressure check, and posterior segment evaluation together. If neurologic warning patterns are in the picture, read vision loss after stroke as part of your red-flag awareness.
Short Story: The Tuesday Night Highway Test
At 7:40 p.m., he pulled over two exits early because road signs looked fogged, not dark, fogged. He blamed his glasses. Then he blamed his age. The next week, his daughter did something unglamorous: she lined up every bottle on the kitchen table, from blood pressure tablets to “harmless” allergy pills.
They logged two weeks of doses and symptoms. A pattern showed up: rough evenings on days with a specific PRN cold medicine, worse after indoor heat and long TV sessions. The eye exam found dry eye layered on early cataract. Nobody “failed” anything. They changed timing, switched one OTC habit, added preservative-free tears, and adjusted the room humidity. Three weeks later, he still had cataract, but he was no longer white-knuckling nighttime ramps. Sometimes progress is not dramatic. It’s just drivable.
Show me the nerdy details
Why overlap is hard: tear-film instability reduces optical quality dynamically, while lens opacity and macular pathology reduce image quality more structurally. Mixed pathology can produce both fluctuating and fixed blur in the same day. That is why exam sequencing and symptom timing logs are clinically useful.
Safer fixes your clinician may consider (without “just stop the med”)
Dose timing changes and alternative drug classes
Sometimes the win is pharmacologic choreography: shifting dose timing, reducing anticholinergic load where possible, or selecting an alternative class with less ocular dryness. This is especially relevant for allergy, sleep, and some mood regimens. The right move is individualized and should include your whole risk profile.
Preservative-free tears, lid care, environmental tweaks
For many people, this is the practical foundation: preservative-free lubricants, warm compresses/lid hygiene, blink pacing during screens, and humidity control. Not glamorous. Very effective when done consistently. Tiny habits beat heroic bursts. A deeper practical routine is available in this guide to preservative-free drops for seniors.
Prescription dry-eye options when OTC fails
If OTC care isn’t enough, clinicians may discuss anti-inflammatory drops, secretagogue approaches, punctal strategies, or device-based support depending on mechanism. Don’t wait until frustration becomes routine.
Here’s what no one tells you… tiny workflow changes beat heroic routines
I’ve watched people fail with “perfect plans” and succeed with one-minute rituals: tears before screens, blink reset at each phone alarm, CPAP mask leak checks, and room humidity targets. Choose boring consistency over dramatic intention.
- Medication review for class/timing opportunities
- Daily preservative-free lubrication strategy
- Environment fixes that reduce evaporation load
Apply in 60 seconds: Set a twice-daily reminder labeled “blink + tears + posture reset.”
Common mistakes checklist (printable decision aid)
“Stop / Start / Ask” framework for your next appointment
STOP (without guidance): abrupt discontinuation of blood pressure, mood, Parkinson’s, or glaucoma therapies.
START: symptom timeline, complete medication inventory, nightly driving note, hydration/environment notes.
ASK: “Can we reduce drying load while protecting my core condition outcomes?”
Red-flag symptoms that move you to same-day care
- Sudden one-eye vision loss or curtain/shadow
- Severe eye pain, nausea/vomiting with vision change
- New flashes/floaters with field loss
- Neurologic changes (weakness, speech issues, facial droop)
Medication reconciliation script for PCP + eye doctor
Use this script verbatim if useful: “I’m not asking to stop medications on my own. I’m asking for a safety review of my total regimen because my blur pattern and dryness have changed. Can we coordinate a plan that protects both vision function and my chronic-condition control?”
Infographic: 3-Step Pathway for Blurry Vision After 60
Step 1 — Detect
Track 14 days: doses, blur timing, burning, night-driving confidence.
Step 2 — De-risk
Avoid abrupt stops. Remove daily redness-drop habit. Flag red-flag symptoms.
Step 3 — Coordinate
Bring one-page log to PCP + eye exam; optimize class/timing + ocular surface care.
Goal: safer vision function without sacrificing chronic-disease control.
FAQ
Can blood pressure medicine make vision blurry even if my numbers are controlled?
Yes, it can in some people, usually through dryness or ocular-surface effects rather than blood pressure failure. Controlled numbers and side effects can coexist. Discuss timing or class alternatives with your prescriber instead of stopping treatment.
Which allergy meds are most likely to dry my eyes?
Older sedating antihistamines are frequent offenders, but individual response varies. Bring exact product names (including OTC combinations) to your appointment, because “PM” and multi-symptom products often hide drying ingredients.
If I switch meds, how fast can dry-eye blur improve?
Some people notice change in days; others need several weeks, especially when multiple contributors exist. Expect staged improvement, not instant perfection.
Are preservative-free tears better for daily use?
For frequent daily use, many clinicians prefer preservative-free formulations to reduce surface irritation risk over time. Product fit still varies by person.
Can antidepressants cause both dry eye and focusing issues?
Yes, in some patients. Possible mechanisms include reduced tear support and accommodative comfort changes. Never stop psychiatric medication abruptly; coordinate changes with your prescriber.
Is nighttime blur a warning sign for driving safety?
It can be. Night blur, halos, and reduced contrast are practical function signals. If confidence drops, prioritize evaluation and consider reducing night driving until your plan is in place.
Should I see an optometrist, ophthalmologist, or my PCP first?
If symptoms are gradual and medication-linked, PCP plus eye care is ideal. If vision function is declining or diagnosis is uncertain, eye specialist evaluation should not be delayed. Emergencies go to urgent/emergency care immediately.
Can dehydration or diuretics make this worse?
Yes. Hydration status and diuretic effects can amplify dryness, especially with indoor heat and screen-heavy days. Mention both fluid pattern and medication schedule at your visit.
What should I bring to a medication-related eye visit?
Bring every prescription, OTC product, supplement list, dosing times, and a 14-day symptom timeline. Include night-driving notes and any recent dose changes.
When is blurry vision an emergency, not a dry-eye issue?
Sudden one-eye vision loss, curtain/shadow, severe pain, new flashes/floaters, trauma, or neurologic symptoms are emergency signs and should be treated as same-day urgent concerns.
Next step: do this in 20 minutes today
Gather every prescription/OTC/supplement into one list
One accurate list beats ten vague memories. Include PRN meds and “just seasonal” products.
Start a 14-day blur-and-burning symptom tracker
Track at three daily points: morning, afternoon, evening. Add medication timing and screen exposure notes.
Book one medication-review visit + one comprehensive eye exam
Two appointments, one shared goal: reduce drying burden while preserving your core disease control. If you want a visit-prep structure, this annual eye exam checklist for seniors can make the appointment more efficient.
- Inventory medications today
- Track symptoms for 14 days
- Coordinate PCP + eye care review
Apply in 60 seconds: Create a note titled “Vision + Med Review” and add your first three medications now.
When to seek help now (not later)
Sudden vision loss, curtain/shadow, severe eye pain, new flashes/floaters
These are emergency features, not dry-eye self-care territory.
One-sided symptoms with headache, nausea, neurologic changes
Urgent evaluation is essential when vision symptoms pair with neurologic or severe systemic signs.
Worsening night-driving visibility despite lubrication
Functional decline despite initial care warrants expedited re-evaluation. If driving confidence is slipping, review senior DMV vision renewal basics early so you can plan safely instead of reacting under pressure.
Conclusion
Let’s close the loop from the opening worry: if your sight feels fuzzy after 60, yes, medications may be part of the story, but rarely the whole story. The win is not fear. The win is sequence: observe, de-risk, coordinate. That sequence protects both your eyes and the conditions those medications were prescribed to treat in the first place.
In the next 15 minutes, do one concrete thing: start your 14-day log and book at least one appointment. Small, steady actions beat anxious guessing every time. You don’t need to be dramatic to be safe. You just need a plan you can actually follow.
Last reviewed: 2026-02.
This article is educational and not a substitute for personal medical care. Do not stop or change prescription medications without clinician guidance. Seek immediate care for sudden vision loss, severe pain, new flashes/floaters, or neurologic symptoms.