
Medicare Coverage for Eylea Injections — The 20% Trap and How Plan G Saved Me
Medicare & Eylea Injections:
The Real Cost of the “20% Hit”
“`
The first time I heard “Medicare covers it,” I relaxed—until the bill quietly reminded me that “covered” can still mean a recurring 20% hit. For Eylea injections under Medicare Part B, that coinsurance isn’t a one-off nuisance; it can become a monthly budgeting ambush when wet AMD care stretches into seasons.
If you’re time-poor and trying to protect your vision without letting the math hijack your life, this is the missing middle between vague reassurance and scary invoices. Keep guessing and you risk two losses at once: delayed treatment decisions and avoidable out-of-pocket drift.
This post helps you map the real cost flow, ask the right retina clinic questions, and compare Original Medicare, Medigap Plan G, and Medicare Advantage with a calm, numbers-first lens. Here is the faster path to money clarity:
- ✓ Estimate your next visit in 60 seconds using a simple Part B baseline.
- ✓ Spot the common billing blind spots before they snowball.
- ✓ Decide if Plan G’s predictability fits your injection rhythm.
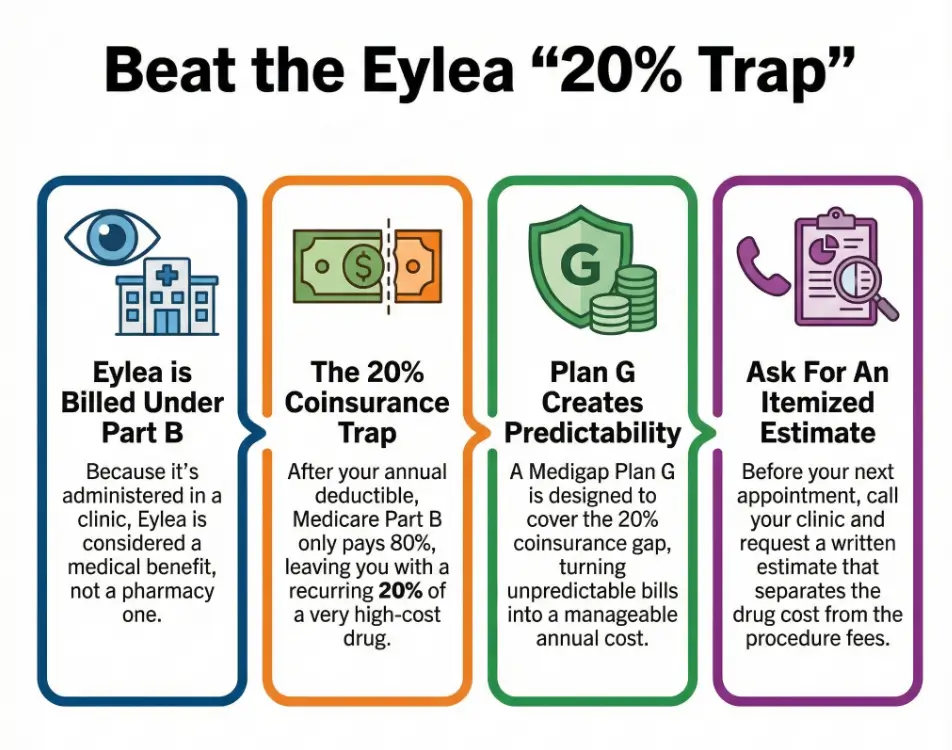
Table of Contents
The fast version if you’re panicking
If you only have three minutes, here’s the clean truth. Eylea (aflibercept) is commonly covered as a physician-administered drug under Medicare Part B when it’s medically necessary for conditions like wet AMD and certain retinal diseases. Part B typically leaves you with 20% coinsurance after the deductible. That number is easy to read and hard to live with when anti-VEGF injections repeat every month or two.
My first mistake was assuming “covered” meant “affordable.” The second was not asking the clinic for a pre-treatment estimate that separated the drug cost from the injection/office fees. The third was waiting too long to compare coverage tiers—Original Medicare alone versus a Medigap plan like Plan G.
- Ask for the drug + procedure breakdown.
- Confirm the clinic bills the correct drug code.
- Compare Medigap and Medicare Advantage calmly, not mid-crisis.
Apply in 60 seconds: Call your clinic and request a written estimate for your next injection.
Why Eylea lands under Part B, not Part D
Eylea injections are typically administered in a retina clinic, so the drug is billed through the medical side, not the pharmacy side. That’s why Part B is the usual home. Clinics often bill Eylea using the HCPCS code J0178 (aflibercept, 1 mg), plus separate codes for the injection procedure and related visits. You don’t have to memorize these, but you should know the code exists—because it can change which bucket your bill lands in.
In plain language: the clinic buys the medication, stores it, and administers it. Medicare then reimburses the clinic under Part B rules. This setup is normal for anti-VEGF injections and is one reason your bill may show multiple line items even on a “simple” injection day.
When I finally asked for the itemized view, I stopped feeling like I was chasing a ghost. It also helped me ask better questions about coverage tiers and whether my supplemental plan could quiet the financial noise.
- Beginner lens: If the drug is given in-office, Part B is likely involved.
- Operator lens: Verify that the drug code and dosage units match your chart.
- Time saved: This one check can prevent hours of phone ping-pong.
The 20% trap: what it looks like in real life
The 20% coinsurance sounds modest until you multiply it by a high-cost biologic and a long treatment timeline. Even when everything is billed correctly, repeated injections can create repeated shocks. The emotional whiplash is real: you walk in worried about your vision, and you walk out worried about your credit card.
I remember one visit where my brain was still foggy from the bright lights and dilating drops, and the front desk casually mentioned what my share might be. That moment wasn’t dramatic—just quietly brutal. The fear wasn’t the single bill. It was the idea of this bill returning, again and again, like a calendar you can’t cancel.
- Do you have Medicare Part B active?
- Is Eylea documented as medically necessary for your diagnosis?
- Is your provider enrolled in Medicare and accepting assignment?
- Do you have a Medigap plan or other secondary coverage?
Next step: If you answered “no” to any item, request a benefits check before your next appointment.
Save this checklist and confirm the current coverage rules on the official Medicare pages.
Two small numbers matter here. First, the Part B deductible resets yearly. For example, in 2024 it was $240, and it often changes each year. Second, the frequency of injections varies by condition and response—some people start monthly, then extend. This means your annual out-of-pocket can swing widely even when the drug stays the same. If you want a zoomed-out context for the wet AMD injection schedule, it can help you sanity-check how fast the 20% stacks across a year.
If you’re time-poor, your best defense is not a spreadsheet marathon. It’s a two-call routine: one to your clinic billing team, one to your plan.
Plan G: why it was the simplest escape hatch
I’m not here to sell you a plan. I’m here to describe the mechanism that calmed my numbers and my nerves. Medigap Plan G is designed to cover most of the out-of-pocket gaps in Original Medicare, including the Part B coinsurance, after you meet the Part B deductible. That “after the deductible” detail matters—but it’s still a cleaner pattern than repeatedly paying 20% of a high-cost injection cycle.
What Plan G gave me wasn’t just savings. It gave me predictability. Instead of bracing for each visit like a financial ambush, I could anchor my year around one known deductible and a consistent premium. For a chronic, vision-threatening condition, that mental relief is not a luxury. It’s part of staying steady enough to show up for treatment.
I compared carriers in my state and asked for quotes that clearly stated the premium, household discounts (if any), and whether the plan was community-rated, issue-age-rated, or attained-age-rated. That felt like “insurance homework,” but it was high-leverage homework. I also kept a simple reference page on AMD treatment cost open so I could compare premium quotes against the real-world rhythm of care.
- It generally covers the Part B 20% coinsurance.
- You still pay the Part B deductible first.
- Predictability can be as valuable as raw savings.
Apply in 60 seconds: Ask for a Medigap quote that explicitly mentions Part B coinsurance coverage.
What to ask your retina clinic before dose one, 2025 (US)
This section is deliberately practical. In the U.S., the billing reality of anti-VEGF injections depends on how the clinic codes the drug, how they document medical necessity, and whether they accept Medicare assignment. The easiest savings are often not “cheaper drugs.” They’re clean paperwork and clean expectations.
Here’s my short script. I used it twice. Both times the call took under 10 minutes, and both times it prevented the “mystery bill” vibe.
- “Can you confirm you bill Eylea under Part B and accept assignment?”
- “Can you provide an estimate separating the drug from the injection and visit?”
- “What diagnosis code will you use for my case?”
- “Do you have a financial counselor who can check my secondary coverage?”
- “If my plan changes, who should I notify before the next dose?”
I also asked if they could note the exact brand planned for the next visit. That prevented a surprise switch that would have complicated my coverage check. If you’re newer to this world, a quick refresher on what AMD injections typically involve can make these calls feel less intimidating.
- Your Medicare card and any secondary insurance details.
- The clinic’s billing NPI and confirmation they accept assignment.
- The drug name, expected dosing interval, and HCPCS code if available.
- An estimate showing drug vs procedure cost lines.
Next step: Use these items to request a written quote that includes premiums and expected Part B cost-sharing.
Save this list and confirm plan pricing on the provider’s official page.
Yes, it’s awkward to ask. But it’s less awkward than trying to decode a bill when your vision is still blurry from dilation.
Mini calculator: estimate your next Eylea out-of-pocket
This is not a perfect prediction tool. It’s a quick reality check for time-poor people who want a ballpark before they pick up the phone. The idea is simple: your share under Part B is often about 20% of the allowed drug + procedure amount, unless you have secondary coverage that reduces it.
Save this estimate and confirm the allowed amount with your clinic’s billing office.
I used a similar back-of-the-envelope check before comparing premiums. It wasn’t sophisticated. It was sanity-saving.
Compare coverage tiers: Original Medicare, Medigap, MA
Think of this as a decision card you can hold in your head while you’re making dinner. The goal isn’t to become an insurance analyst. The goal is to avoid expensive surprises.
- A: Original Medicare only — best if you want broad provider access but can tolerate the 20% risk.
- B: Original Medicare + Plan G — best if you want predictable costs for frequent Part B services.
- C: Medicare Advantage — best if you prefer bundled benefits and are comfortable with network rules and prior authorization.
Time/cost trade-off: Plan comparisons can take 30–60 minutes, but may reduce recurring uncertainty for the entire year.
Save this card and confirm the current coverage tiers with your plan’s official summary of benefits.
What surprised me most was how often the “right” choice depended on treatment frequency. If you’re early in wet AMD management with monthly injections, the math leans differently than if you’re stable on an extended interval. That’s why timing matters: open enrollment windows are limited, but your retina plan can change quickly. A quick look at the typical extension patterns for wet AMD injections can help you choose coverage based on real cadence, not generic advice.
Also, do not ignore the human layer. Some Medicare Advantage plans are excellent. Some are administrative obstacle courses. If you’re already exhausted, simplicity is a legitimate medical-adjacent need.
Show me the nerdy details
Anti-VEGF therapy is often billed as a combination of drug acquisition/administration and professional services. Your out-of-pocket is influenced by the allowed amount, the clinic’s acceptance of assignment, secondary coverage rules, and annual deductible status. These mechanics are why two patients in the same waiting room can see very different bills.
Appeals, prior authorization, and the paperwork that actually matters
If you’ve ever had your vision threatened by a clock, you know paperwork can feel like an insult. Still, it’s part of the game. Medicare Advantage plans commonly use prior authorization pathways for high-cost therapies. Original Medicare does not usually run the same style of prior authorization, but documentation of medical necessity still matters.
I had one borderline moment where a plan change created confusion about my next injection timing. The fix wasn’t heroic. It was procedural: a short letter from the retina specialist confirming diagnosis, response to therapy, and the risk of delaying treatment.
- Ask for a short, specific medical-necessity note.
- Request the exact billed drug name and code on the estimate.
- Keep a simple log of injection dates and response notes.
This isn’t about becoming paranoid. It’s about being ready when a call center script doesn’t match your reality.
- Keep your diagnosis and injection history handy.
- Ask your clinic for a template note if available.
- Document the medical risk of delay, not just inconvenience.
Apply in 60 seconds: Save your last two visit summaries in a single folder you can email quickly.
The hidden costs people forget: parking, companion care, time
When we talk about Eylea costs, we focus on the obvious line items. But real life has stealth expenses. The average injection day can eat 2–4 hours door-to-door depending on travel, waiting time, dilation, and post-visit recovery. If you need a family member to drive you, the cost isn’t just gas—it’s lost work hours and emotional bandwidth.
I once tried to “optimize” by scheduling a visit during a busy work week. I saved nothing. I just moved the stress into a new room. Now I treat injection days as medical half-days and protect my schedule accordingly.
- Time budget: Plan for a 3-hour block when possible.
- Comfort kit: sunglasses, lubricating drops, a snack.
- Coordination: confirm your ride before you confirm your meeting.
These details don’t show up in a fee schedule, but they decide whether treatment feels sustainable. If your family is trying to map risk across years—not just months—resources like family history of eye disease and blindness risk after 70 can add helpful context to your long-term planning conversations.
Short Story: The invoice that taught me to ask one better question (120–180 words) …
Short Story: I was sitting in my car outside the clinic, one eye still watering, when my phone buzzed with an online statement. The number wasn’t catastrophic, but it was sharp enough to ruin the rest of my afternoon. I remember thinking, “If this is the ‘covered’ version, what does ‘not covered’ even look like?” I went home, pulled up the statement, and saw three confusing lines that all sounded like the same thing.
The next morning I called the billing desk with a single question: “Can you separate the drug cost from the procedure and tell me the allowed amount for each?” The voice on the other end softened. Suddenly the bill had shape. I wasn’t guessing anymore. That ten-minute call didn’t just lower my anxiety—it made my Plan G decision obvious. When your vision is on the line, clarity is a form of care. …
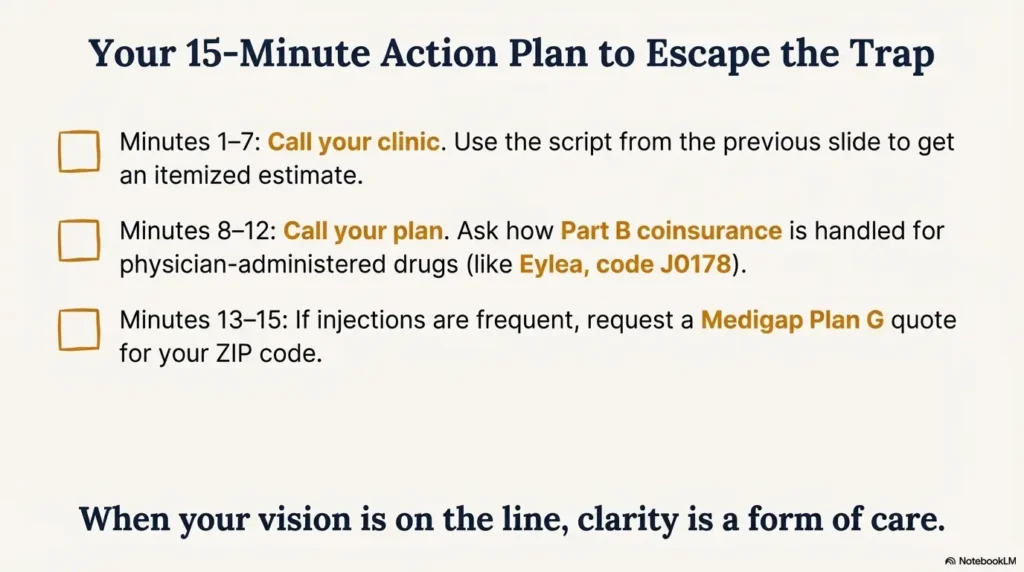
Your 15-minute action plan
This is the section I wish someone had handed me on day one. No grand speeches. Just the highest-leverage next moves.
| Item | Typical payer bucket | What you may owe | Notes |
|---|---|---|---|
| Eylea drug (aflibercept) | Medicare Part B | Often ~20% coinsurance | Secondary coverage may reduce this. |
| Injection procedure/visit | Medicare Part B | Coinsurance varies by allowed amount | Ask for an itemized estimate. |
| Part B deductible | Annual | You pay this first | Amount changes yearly. |
| Medigap Plan G premium | Private carrier | Monthly premium | Rates vary by ZIP, age, and carrier. |
Save this table and confirm the current fee and premium ranges on the provider’s official page.
Now the checklist:
- Minute 1–3: Find your last bill and locate the drug line item.
- Minute 4–7: Call the clinic and ask for the next-visit estimate with drug/procedure separation.
- Minute 8–12: Call your plan and ask how Part B coinsurance is handled for anti-VEGF injections.
- Minute 13–15: If you’re considering Medigap, request a Plan G quote that includes your ZIP and enrollment window details.
When I did this in one sitting, I stopped feeling like my finances were being run by a random-number generator.
FAQ
Does Medicare cover Eylea for wet AMD?
Often, yes—when your retina specialist documents medical necessity, Eylea is typically treated as a Part B-covered, in-office administered drug. Apply in 60 seconds: Ask your clinic to confirm the diagnosis and drug code they will bill for your next visit. If you want a simple baseline explanation you can share with family, the broader guide on AMD injections can be a helpful companion.
Why is my bill so high if Part B covers it?
Part B coverage usually still leaves you with coinsurance and a yearly deductible. With repeated injections, that 20% can add up fast. Apply in 60 seconds: Request a written estimate that splits the drug cost from the procedure cost.
Will Plan G always wipe out the 20%?
Plan G is designed to cover most Part B coinsurance after the Part B deductible is met, but details can vary by timing, enrollment status, and carrier rules. Apply in 60 seconds: Ask for a Plan G quote and confirm it covers Part B coinsurance for physician-administered drugs.
Is Medicare Advantage a good option for Eylea?
It can be, especially if your plan has strong specialist networks and clear prior authorization pathways. But networks and rules matter. Apply in 60 seconds: Check whether your current retina clinic and preferred hospital are in-network before switching.
What if my plan denies coverage or delays approval?
You may need a brief medical-necessity letter stating diagnosis, treatment response, and the risk of delay. Apply in 60 seconds: Ask your specialist’s office for a one-page letter template you can reuse.
Can I switch from Eylea to another anti-VEGF to save money?
Treatment choice is clinical first. Cost differences exist, but switching should be guided by your specialist and your coverage rules. Apply in 60 seconds: Ask your doctor to document why the chosen drug is best for your specific case.
Your 15-minute action plan
If you’re already thinking, “Okay, but what do I do before my next appointment?”—this is the clean, doable path. It’s designed for people who are tired, busy, and still determined to protect both sight and sanity.
- Step 1: Confirm Part B status and whether your clinic accepts assignment.
- Step 2: Get a written pre-treatment estimate for the next dose.
- Step 3: Run the mini calculator above to sanity-check the number.
- Step 4: If injections are frequent, compare Original Medicare + Plan G versus your current setup.
When I finally followed these steps, the 20% stopped feeling like a shadow following me to every appointment.
Last reviewed: 2025-12; sources: Medicare.gov, CMS fee schedule pages, AAO clinical education.
Conclusion
The 20% trap isn’t a moral failing or a budgeting flaw. It’s a design feature of Part B cost-sharing that becomes emotionally heavy when treatment is frequent and non-optional. What changed everything for me was not a miracle discount. It was asking the billing questions early and choosing a coverage tier that respected the reality of ongoing injections. Plan G didn’t erase the seriousness of my condition—but it reduced the financial static enough for me to focus on healing. If you’re building a broader prevention and monitoring routine alongside treatment, tools like an annual eye exam checklist for seniors can help you stay organized without turning your life into a medical admin job.
Your next step within 15 minutes: call your clinic for an itemized estimate, then call your plan to confirm how your Part B coinsurance is handled for Eylea. If you’re in a window to enroll in Medigap, request a Plan G quote with your ZIP and compare it against your expected injection frequency. Clarity first—panic never helps your vision.