


Navigating the Midnight Obstacle Course:
A Senior’s Guide to Safer Bedroom Night Routines
At 3:07 a.m., even a familiar bedroom can turn into a small obstacle course. The chair is not where the body remembers it. The bathroom light feels too bright. A slipper has migrated under the bed like it joined a tiny witness protection program.
For seniors with poor vision, a safer bedroom night routine is not about buying every gadget with a glowing button. It is about making the bed-to-bathroom path clear, lit, repeatable, and forgiving. When low vision, sleepiness, medication effects, dizziness, or clutter meet in the dark, guessing becomes expensive.
Here is the calmer truth:
- ✓ Most improvements are small.
- ✓ They work because they remove decisions.
- ✓ They protect dignity instead of replacing it.
This guide shows caregivers, spouses, adult children, and older adults how to reduce nighttime fall risks using practical layout changes, better lighting, stable footwear, high contrast, and a simple 10-minute safety walk. It draws on fall-prevention ideas from the CDC, National Institute on Aging, and low-vision home safety principles used by eye-care and occupational therapy professionals.
The Safer Night Routine Snapshot
A senior’s bedroom does not need to look clinical to become safer. The goal is a predictable chain: wake, reach, light, see, stand, step, bathroom, return. Every link should be easy to find by sight, touch, or habit.
lamp, glasses, phone, mobility aid
soft path lighting without glare
one clear lane to the door
same route, same objects, same landing spots
Table of Contents

The 3 A.M. Problem: Why Bedroom Safety Changes After Dark
Nighttime is not just “daytime with less light”
Night changes the room. Shadows thicken around furniture legs. A dark slipper blends into a dark rug. A shiny floor reflects a night light and looks briefly wet. For someone with cataracts, glaucoma, macular degeneration, diabetic eye disease, or reduced contrast sensitivity, these tiny distortions can become real hazards.
Sleep adds its own fog. The brain is not fully online. Balance may be slower. A person may be thinking about the bathroom, not the charging cable curled near the baseboard. The body walks from memory, but the room may have changed since bedtime.
The bathroom trip is the real danger zone
The highest-risk part of many bedroom night routines is not lying down or waking up. It is the chain of small transitions: sitting up, reaching for glasses, finding slippers, standing, turning, walking through the doorway, entering the bathroom, using the toilet, washing hands, and returning.
Each transition asks for vision, balance, strength, and judgment. That is a lot of committee work for 3 a.m.
Here’s what no one tells you…
Many nighttime falls are not theatrical accidents. They start with ordinary movements: stepping around laundry, reaching for a lamp, turning too quickly, misjudging the bed edge, or trying to “just make it” without turning on a light.
That phrase, “just make it,” deserves a tiny warning bell. It often appears right before the room wins.
- Make the path visible before bedtime.
- Keep the first reach items in the same place.
- Reduce glare and floor clutter together.
Apply in 60 seconds: Stand at the bedroom door tonight and remove the first object your eyes hesitate over.
Who This Is For, And Who Needs More Than a Checklist
Best fit: aging-in-place homes with manageable low vision
This guide is for homes where an older adult can usually move around with some independence but needs a safer, more predictable night setup. It is especially relevant for seniors living with cataracts, glaucoma field loss, macular degeneration, diabetic eye disease, stroke-related visual field changes, double vision, or general age-related low vision.
If glaucoma has reduced peripheral vision, bedroom corners and low objects can become harder to detect. A related guide on glaucoma field loss home safety can help families think beyond brightness and focus on what the eye may no longer catch from the side.
Not enough: when supervision or clinical support may be needed
A bedroom checklist is not enough when falls are frequent, dizziness is new or severe, transfers are unsafe, or the person wanders at night. Advanced dementia, fainting, sudden weakness, repeated near-falls, and inability to use a cane or walker safely all deserve more than furniture rearranging.
Home tweaks can reduce friction. They cannot diagnose fainting, medication interactions, stroke symptoms, infections, or sudden vision loss.
Caregiver note: safety without taking over the room
Caregivers often arrive with good intentions and a measuring tape. The older adult may see the measuring tape and hear, “Your room is no longer yours.” That emotional gap matters.
Start with the senior’s routine. Ask where the hand naturally reaches. Notice which objects feel comforting. Then adjust the path around those habits whenever possible. Independence is not a decoration. It is part of the safety plan.
Money Block: Is a Home Checklist Enough?
Answer yes or no:
- Has there been a fall, head impact, fainting, or injury in the last 6 months?
- Does the senior feel dizzy when standing at night?
- Does the person grab walls or furniture to walk?
- Are medications causing drowsiness, urgency, or balance changes?
- Is vision changing quickly or suddenly?
If all are no: begin with the room setup and 10-minute route test.
If any are yes: improve the room, but also ask a clinician, eye doctor, pharmacist, physical therapist, or occupational therapist for a fall-risk review.
Neutral action line: Write down the yes answers and bring them to the next appointment.
Start Beside the Bed: The Reach Zone That Prevents Panic
Put the first five items where the hand naturally lands
The night routine begins before the feet touch the floor. The first reach should be calm and predictable. Put the lamp switch, glasses, phone, tissues, and mobility aid where the hand naturally lands from the sleeping position.
For some people, that means the left side of the nightstand. For others, a wall-mounted lamp switch is easier than a tiny knob. The right answer is not the prettiest arrangement. It is the one that works while half-awake.
A dedicated guide to low vision bedside organization can help families set up a nightstand that is practical without becoming a drawer-shaped junk storm.
Make the nightstand boring, stable, and ruthless
A safe nightstand is not a museum of sentimental objects. It should be heavy enough not to slide, uncluttered enough to scan, and simple enough to use by touch. Remove glass decorations, loose coins, tiny pill bottles, wobbly trays, and mystery cords.
Keep water only if it is safe and practical for that person. If medication belongs at the bedside, make sure it is clearly organized and approved by the clinician or pharmacist. For low-vision medication routines, low vision medication safety matters because the wrong bottle at night is not a small error.
One touch, one result
Objects should behave the same way every night. A touch lamp should turn on reliably. A flashlight should be in the same tray. A phone should charge in the same cradle. Glasses should sit in a high-contrast case, not vanish on a dark tabletop.
Think of the reach zone like sheet music. The notes should not move between performances.
Short Story: The Lamp That Moved Three Inches
Marianne’s father insisted he knew his bedroom “with his eyes closed,” which was almost the problem. After cataract surgery in one eye and worsening glare in the other, he still reached for the old lamp by memory. One night, a visiting grandchild moved the lamp three inches to make room for a book.
At 2:40 a.m., his hand swept the table, knocked over a water glass, and he stood up too quickly because the noise startled him. No fall happened, but the whole family heard the warning. The fix was not dramatic. They placed the lamp switch in the exact same reach spot, moved the water to a lidded cup, used a pale tray on the dark table, and gave the phone its own charging stand. The lesson was quiet but firm: for low vision, consistency is not fussiness. It is a handrail made of habit.
Light the Path, Not the Whole Room
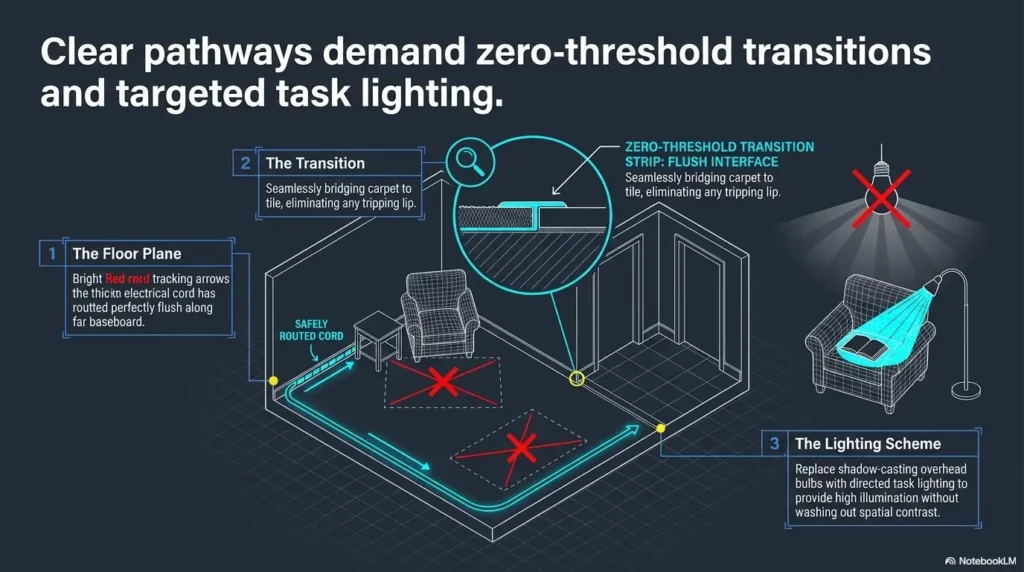
Use layered lighting instead of one harsh overhead blast
Better night lighting does not mean flooding the bedroom with brightness. Harsh overhead light can create glare, deep shadows, and a sudden “stage spotlight” effect. A layered setup usually works better: bedside lamp, low-glare night light, hallway guide light, and gentle bathroom entry lighting.
Motion-sensor lights can help when they are placed low and aimed away from the face. They should reveal the route, not interrogate the sleeper.
If bright automatic lighting becomes uncomfortable, the placement may be wrong. A guide on what to do when a motion sensor light is too bright can help adjust the angle, warmth, and location before abandoning the idea.
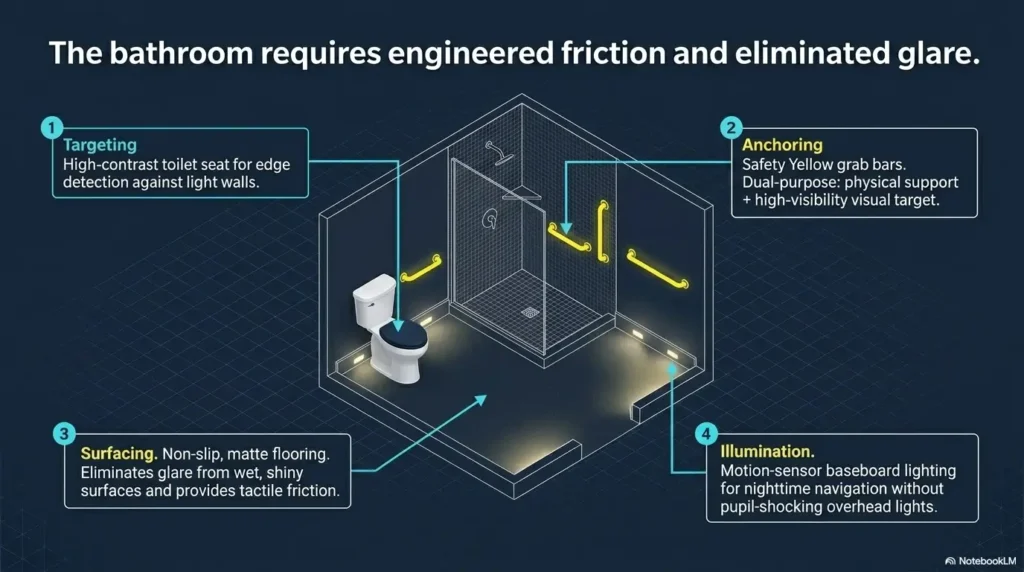
Avoid glare, mirror flash, and shiny-floor confusion
The American Academy of Ophthalmology advises improving home lighting for low vision and reducing glare from reflective surfaces. In the bedroom, that means watching for shiny floors, glossy furniture, uncovered bulbs, mirrors reflecting lamps, and bright bathroom light bouncing back toward the bed.
Glare is not just “too much light.” It is light in the wrong place, arriving at the wrong angle, with too much visual noise around it.
Don’t do this: the dark room, bright bathroom trap
A common setup creates a dark bedroom and a bright bathroom. The older adult wakes, walks in dimness, then opens the bathroom door into a burst of light. That abrupt change can cause squinting, disorientation, and a brief loss of detail.
A better plan is a gentle gradient. Soft bedside light. Low hallway light. Bathroom light that starts low or is guided by a warm night light. If choosing between red and amber options, a comparison of red vs amber night light can help families think about comfort, visibility, and sleep disruption.
Show me the nerdy details
Low vision safety depends on more than brightness. Contrast sensitivity, glare recovery, adaptation between dark and light, visual field loss, and depth perception all affect how a person reads a room at night. A brighter bulb may help one task while making another task worse if it creates reflection on tile, glossy furniture, or a mirror. The practical method is to test lighting from the senior’s actual path: sitting on the bed, standing, turning, entering the bathroom, and returning. The best light is the one that reveals edges without shining into the eyes.
- Use soft layers instead of one harsh overhead light.
- Aim lights at floors and edges, not faces.
- Reduce reflections from mirrors, shiny floors, and glossy surfaces.
Apply in 60 seconds: Turn on the current night lighting and look for the brightest glare spot from the bed.
Build a One-Lane Walking Route from Bed to Door
Clear the floor like a runway, not a storage shelf
The safest walking route is boring. That is a compliment. From the side of the bed to the door, remove throw rugs, shoes, laundry baskets, pet toys, cords, fan bases, low stools, storage bins, and decorative objects.
Do not tuck cords under rugs. That hides one hazard by creating another. Route cords along walls and secure them safely. Keep phone chargers and lamp cords out of the footpath.
Mark edges with contrast, not chaos
Low vision often makes edges harder to read. Use contrast where the body makes decisions: bed frame edge, door threshold, bathroom doorway, step-up, chair corner, walker handle, and light switch area.
Contrast does not need to look loud. A pale strip on a dark edge or a dark strip on a pale edge can do the job. The point is to make the edge answer before the foot has to ask.
Bathroom contrast can be especially useful. If the toilet blends into the floor or wall, a guide on toilet seat contrast color may help make the destination easier to locate without turning the room into a color experiment gone rogue.
The floor should not ask questions
At night, a senior should not have to wonder whether a dark shape is a slipper, a rug pattern, a pet, or a shadow. The floor should be plain, open, and easy to read.
Patterned rugs, high-contrast busy flooring, and glossy tile can create visual confusion. Where possible, simplify. The most elegant bedroom safety upgrade may be an empty path.
Money Block: Bedroom Route Decision Card
| Choice | Use it when | Trade-off |
|---|---|---|
| Remove rug | The rug is loose, curled, dark, or in the walking lane. | Less cozy, much clearer path. |
| Secure rug | The rug is necessary and can be fully secured. | Needs regular checking for lifted edges. |
| Move furniture | The walker, cane, or body has to swerve. | Takes effort once, pays off nightly. |
Neutral action line: Choose the option that makes the path easiest to follow when sleepy, not the one that looks best at noon.
Fix the Slipper Problem Before It Fixes You
Bedside footwear should be boringly excellent
Good nighttime footwear is not glamorous. It fits well, has a back, grips the floor, and stays where it belongs. It should be easy to put on without bending dangerously or hunting under the bed.
Loose slippers, floppy slides, and worn soles can turn a bathroom trip into a balance test. Nobody asked for an Olympic event in the hallway.
Socks alone are not a plan
The CDC identifies foot pain and poor footwear as fall-risk factors. At night, socks can be especially risky on smooth floors or stairs. Even socks with grips may not solve problems if they twist, fit poorly, or make the person feel less stable.
If foot pain, numbness, neuropathy, swelling, or arthritis affects walking, footwear choices may need input from a clinician, podiatrist, or physical therapist.
Put footwear in the same landing spot every night
Low vision routines work best when location becomes part of memory. Put slippers or shoes in the same place every night, ideally beside the bed where the feet naturally land.
Use a small high-contrast mat or tray only if it does not create a trip hazard. The goal is a landing zone, not a floor decoration with ambitions.
- Choose nonslip soles and a secure back.
- Avoid loose slippers and slick socks.
- Keep footwear in the same bedside landing spot.
Apply in 60 seconds: Check the soles of the current slippers and remove them if they are smooth, stretched, or floppy.
Common Mistakes That Make Night Routines Riskier
Mistake 1: adding gadgets before removing hazards
A new motion light will not fix a curled rug. A fall alert button will not prevent a stumble over a fan cord. Start with hazards, then add tools.
That order matters: clear, light, stabilize, then consider devices.
Mistake 2: trusting memory more than layout
A room can be familiar and still unsafe. Vision changes. Balance changes. Medications change. A grandchild visits and drops a backpack. A pet decides the hallway is a luxury sleeping platform.
Layout should carry the routine when memory is tired.
Mistake 3: placing the phone where it looks neat, not where it is reachable
A phone across the room may look tidy. After a fall, it might as well be on the moon. Keep the phone reachable from the bed and, when possible, consider a wearable emergency device for people at higher risk.
For seniors with low vision, a wallet card emergency info template can also help responders or neighbors quickly understand contacts, conditions, and medication concerns.
Mistake 4: assuming the senior will “just call out”
Calling out depends on hearing, proximity, pride, awareness, and a door being open. At night, confusion or embarrassment may delay asking for help.
Plan for realistic behavior. People do not become perfectly practical at 3 a.m. They become themselves, but sleepier.
Money Block: Quote-Prep List for Home Safety Help
If you plan to compare a handyman, occupational therapist home visit, aging-in-place consultant, or medical alert service, gather these first:
- Room photos taken at night with current lights on.
- List of recent falls, near-falls, dizziness, or nighttime confusion.
- Current mobility aids: cane, walker, grab bars, bed rail, raised toilet seat.
- Vision diagnosis or main visual difficulty, such as glare, field loss, or low contrast.
- Medication timing concerns to discuss with a clinician or pharmacist.
- Budget range and whether changes must be temporary, renter-friendly, or permanent.
Neutral action line: Get two opinions for bigger home changes, especially anything drilled, wired, or medically recommended.
The Bathroom Route: Where Bedroom Safety Must Continue
Match bedroom lighting to bathroom lighting
The bathroom route should feel like one connected path. If the bedroom is dim and the bathroom is bright, the transition may be jarring. Try a soft bathroom night light, a dimmable fixture, or motion lighting that does not shine directly into the eyes.
For glare-sensitive eyes, light temperature can matter. Some families find warmer bulbs more comfortable. A guide to 2700K vs 3000K for glare-sensitive eyes may help when the room feels either too yellow, too harsh, or oddly washed out.
Clear the doorway, threshold, and mat zone
The National Institute on Aging recommends checking fall risks room by room, including floors, lighting, bathrooms, and pathways. For the bedroom-to-bathroom routine, pay special attention to the doorway, threshold, bath mat, toilet area, and sink area.
Bath mats should not bunch, slide, or hide threshold changes. Bathroom floors should be dry. If the tub or shower area is part of the nighttime route, anti-slip placement matters. The guide on anti-slip shower strips placement can help prevent the common mistake of putting traction only where it looks symmetrical.
Make the return trip just as safe
The return trip gets less attention, but it may be riskier. The person may be colder, sleepier, or more rushed to get back under the covers. The same lighting, footwear, and clear path must work both ways.
Do not judge the route only from bed to bathroom. Test bathroom to bed, too.
The Bedroom Night Safety Loop
Pause before standing
Lamp, glasses, phone
Soft path, low glare
Footwear, balance, aid
One clear lane
Same safe path back
Use it: If any step feels uncertain, fix that step before adding more equipment.
Medication, Dizziness, and the Night Routine Nobody Wants to Discuss
Ask whether nighttime timing increases fall risk
Some medications can contribute to drowsiness, dizziness, urgency, blurred vision, or slower reaction time. This can include sedatives, sleep aids, some antidepressants, some blood pressure medicines, and other drugs, but the exact risk depends on the person and prescription.
Do not stop or move medications casually. The safer move is to ask a clinician or pharmacist whether nighttime symptoms could be related to timing, dose, interactions, dehydration, or bathroom urgency.
Don’t move medications casually
Medication organization is a safety issue, especially for low-vision seniors. If pill bottles look similar, labels are hard to read, or instructions are confusing, fix that system during the day before it becomes a night problem.
Tools like a one-page medication list template and a low vision medication tracker printable can make conversations with doctors and pharmacists clearer.
Let’s be honest…
“I only got up for a second” is the sentence that defeats many safety plans. The body does not give bonus stability for short trips. A six-step walk can still include dizziness, glare, a slippery sock, and a badly placed laundry basket.
Build the routine for the worst version of the night: sleepy, hurried, dim, and slightly annoyed.
Money Block: Night Risk Mini Calculator
Use this simple score to decide whether the routine needs a basic cleanup or a deeper review.
Estimated routine risk score: Not calculated yet.
Neutral action line: Treat this as a conversation starter, not a medical diagnosis.
Make the Room Easier to Read for Poor Vision
Use contrast where decisions happen
Contrast belongs where the person must choose, reach, step, or turn. Add contrast to the bed edge, chair seat, door frame, light switch, walker handle, bathroom doorway, and phone charging station.
A black remote on a dark blanket is a vanishing act. A white tissue box on a pale nightstand is not far behind. Give important objects backgrounds that help them stand out.
Reduce visual noise on surfaces
Visual clutter can be exhausting. Busy bedding, patterned rugs, crowded nightstands, glossy paint, and decorative objects can make a room harder to interpret quickly.
If glare is part of the problem, consider matte surfaces when possible. The difference between matte vs glossy paint can be surprisingly practical for low-vision rooms, especially when lamps or windows create reflections.
Keep essential objects in fixed homes
The phone lives in its stand. Glasses live in the contrast tray. The cane lives beside the bed. Slippers live at the foot landing. Flashlight, remote, emergency button, and tissues each have a home.
When objects have fixed homes, the room becomes easier to trust. That trust lowers panic, and lower panic often means safer movement.
- Use contrast at edges and reach points.
- Choose simpler surfaces where possible.
- Give each essential item a fixed home.
Apply in 60 seconds: Put the phone, glasses, and flashlight on a tray that contrasts with the nightstand.
Caregiver Check: Test the Routine in the Dark Before It Matters
Walk the route at senior eye level
Do not audit the room like a healthy adult strolling through with ceiling lights on. Sit on the bed. Reach for the lamp. Find the glasses. Put on the footwear. Stand slowly. Walk to the bathroom. Return.
Then do it with the actual night lighting. You may discover that the “clear path” is clear only if you are wide awake and built like a mountain goat.
Watch for the almost fall
Near-falls matter. Wall-touching, furniture grabbing, hesitation, shuffling, turning in several tiny steps, or saying “I’m fine” too quickly can all be signals.
Keep a simple note of what you observe. If patterns repeat, bring them to a clinician, physical therapist, or occupational therapist. A doctor appointment note-taking system can help families report the pattern without turning the visit into a foggy memory contest.
The tiny audit that beats the expensive panic buy
A 10-minute route test can reveal hazards before families buy equipment that does not match the real problem. Maybe the issue is not the lack of a medical alert device. Maybe it is the lamp switch, the loose rug, and the bathroom glare.
Start with what the route tells you.
When to Seek Help: Red Flags That Need More Than Home Tweaks
Call a clinician after new or repeated falls
Home changes are helpful, but some warning signs need medical attention. Call a clinician promptly after a fall with injury, head impact, fainting, severe dizziness, new weakness, new confusion, sudden vision change, or repeated falls.
Sudden changes in vision should not be treated as normal aging. A guide to senior vision changes warning signs can help families decide when an eye concern should move from “watch it” to “schedule care.”
Ask for a fall-risk review
The CDC encourages older adults and families to talk with a doctor about fall risk and medicines that may cause dizziness or drowsiness. This is especially important when poor vision overlaps with blood pressure changes, sleep medication, neuropathy, or recent illness.
A fall-risk review may include vision, medication timing, balance, strength, blood pressure, footwear, assistive devices, and home hazards. It is not an accusation. It is maintenance for the human operating system.
Bring in the right pro when the room keeps failing the person
If the room remains unsafe after basic fixes, consider the right professional. A primary care clinician can review health risks. An eye doctor can assess changing vision. A pharmacist can review medication timing and side effects. A physical therapist can assess balance and mobility. An occupational therapist can look at the actual home routine.
If low vision is making daily tasks harder beyond the bedroom, a list of low vision OT questions can help families make the most of a professional visit.
- Document falls and near-falls.
- Ask about medication side effects and timing.
- Use professionals when the routine stays unsafe.
Apply in 60 seconds: Write down the last fall, near-fall, or dizzy spell with the date, time, and what happened right before it.
FAQ
What is the safest bedroom setup for a senior with poor vision at night?
The safest setup usually has a clear path from bed to door, a reachable lamp or switch, stable footwear, phone access, high-contrast object placement, and no loose rugs, cords, or clutter in the walking lane. The room should be easy to navigate while sleepy, not just tidy during the day.
Are motion-sensor night lights good for seniors with low vision?
They can be helpful when placed along the bed-to-bathroom path and aimed away from the eyes. The best motion lights are soft, reliable, and positioned to reveal edges and floor hazards. If they are too bright or create glare, they may need a warmer bulb, lower placement, or a different angle.
Should seniors with poor vision sleep with a light on?
It depends on comfort, sleep quality, and safety needs. A soft path light may be better than a bright room light because it supports orientation without flooding the room. If the person wakes often or feels disoriented, test low-glare lighting that shows the floor, doorway, and bathroom entrance.
What should be on a senior’s nightstand for safety?
Useful items include a lamp control, glasses, phone, emergency contact method, tissues, water if appropriate, and only essential medications if a clinician or pharmacist agrees with that setup. Keep the surface uncluttered and use contrast so items do not disappear into the tabletop.
Are throw rugs dangerous in a senior bedroom?
Loose throw rugs can be risky, especially at night. Curled edges, sliding mats, dark colors, and rugs placed in the walking lane can increase trip risk. If a rug is necessary, it should be secured and checked often. In many bedrooms, removing it is the safer choice.
How can caregivers make nighttime bathroom trips safer?
Start by lighting the route, clearing the floor, placing stable footwear in the same spot, keeping the phone reachable, reducing glare, and testing the route after dark. Also ask whether medications, dizziness, urgency, or foot pain are making the trip riskier.
When should poor night vision be checked by an eye doctor?
Schedule an eye evaluation if night vision worsens, glare becomes difficult, familiar spaces become harder to navigate, prescriptions seem outdated, or vision changes suddenly. Sudden vision loss, new double vision, flashes, a curtain-like shadow, or eye pain should be treated urgently.
Is a bed rail a good idea for seniors with poor vision?
A bed rail may help some people with positioning, but it can create hazards if used incorrectly or if the person tries to climb over it. Ask a clinician or occupational therapist before adding one, especially if there is confusion, weakness, or unsafe transfers.
What is the fastest bedroom safety fix to do tonight?
Clear one path from the bed to the bathroom, put the phone and lamp within reach, remove loose rugs or cords, and place stable footwear where the feet land. That small reset can make the next nighttime trip calmer and safer.
Next Step: Do the 10-Minute Bed-to-Bathroom Safety Walk Tonight
Start from the pillow, not the doorway
The safest audit begins where the routine begins. Sit on the bed. Reach for the lamp. Find the glasses. Place feet into footwear. Stand. Walk to the bathroom. Use the same lighting the senior would use at night. Then return to bed.
Notice every snag: the reach that feels awkward, the shadow that hides an edge, the slipper that shifts, the doorway that feels narrow, the bath mat that moves, the phone that is too far away.
Remove three hazards before buying anything
Pick three hazards tonight. Remove a loose rug. Move a cord. Clear a laundry pile. Replace unstable slippers. Shift the lamp. Add contrast to the bed edge. Move the phone closer. Reduce a glare source.
Small fixes done tonight are better than perfect plans saved for a someday that keeps rescheduling itself.
Leave tomorrow a safer room than tonight
The 3 a.m. problem is not really about darkness. It is about a sleepy person being asked to solve too many small problems at once. A safer bedroom night routine makes the room answer first: the light is reachable, the path is clear, the footwear is waiting, the bathroom route is visible, and help is within reach.
Within the next 15 minutes, do one complete bed-to-bathroom safety walk and remove the first three hazards you find. That is not a renovation. It is a quieter night, built one practical choice at a time.
Last reviewed: 2026-05.