


Mastering the 3 P.M. Burn: A 7-Day Reset for Medication-Related Dry Eye
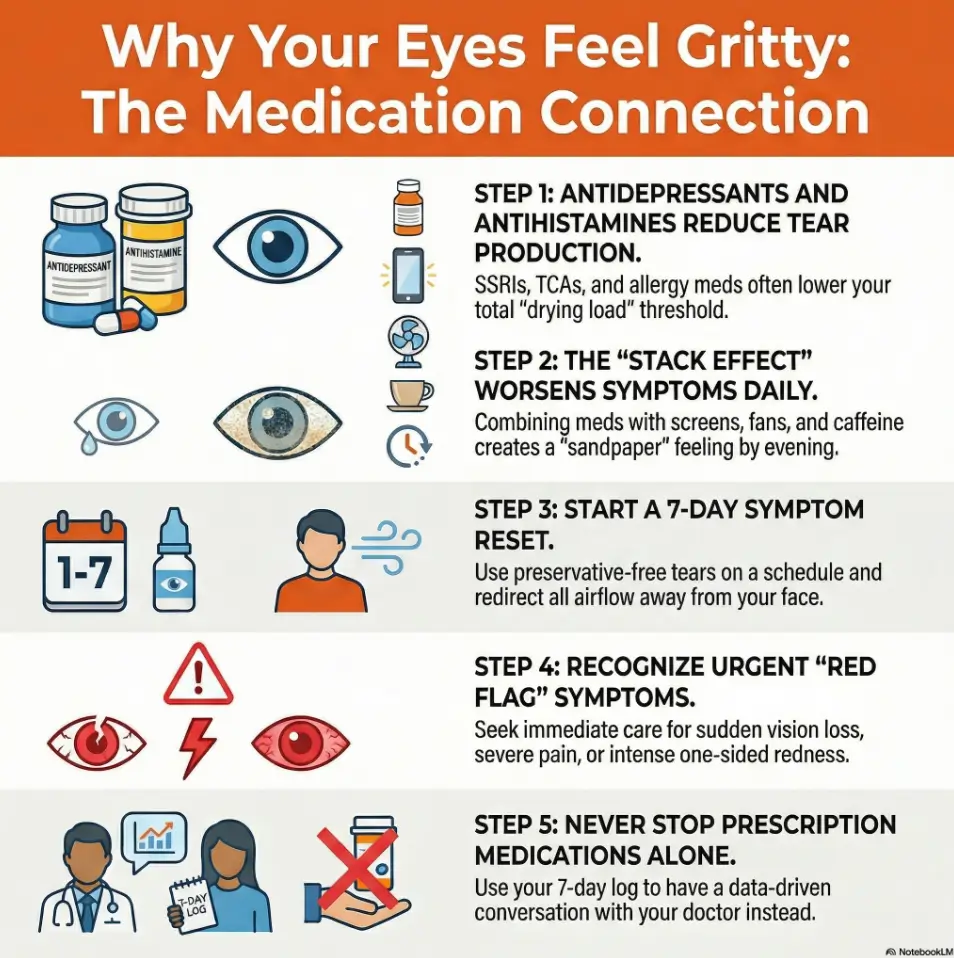
By 3 p.m., your eyes feel like fine grit under the lids, and by dinner they burn, blur, and water at the same time. This isn’t random fatigue. It is often the result of stacking factors like antidepressants, antihistamines, intense screen load, and dry indoor air. If this pattern sounds familiar, compare it with this focused breakdown of why burning eyes spike in the late afternoon.
The challenge is that symptoms mimic everything: allergies, lack of sleep, or contact lens issues. Most people lose weeks switching brands and guessing wrong while work accuracy slips and night driving becomes a stressor.
This guide helps you separate signal from noise in one week, without risky self-experiments or abrupt medication changes.
- ✔ Practical 7-Day Reset: Establish a baseline for your ocular health.
- ✔ Spot Red Flags: Identify medication-related triggers fast.
- ✔ Clinician-Ready Data: Build a timeline for safer, faster medical decisions.
No drama. No brand-hopping. Just a clear method you can run starting today.
Notice the timing. Spot the pattern. Simplify your next step.
Table of Contents
Start Here: Is It Drug-Linked Dry Eye or Something Else?
The 3-signal pattern: timing, triggers, and relief window
Most people track symptoms by intensity, not by timing. That is like reading sheet music but ignoring tempo. Dry-eye patterns tied to medication often have a steady rhythm: better in the morning, worse after screens, worse in dry indoor air, and cranky by evening. If symptoms ease after preservative-free tears and short screen breaks, that supports surface dryness rather than sudden structural disease.
One quick framework:
- Timing: When does discomfort start? Morning, afternoon, or all day?
- Triggers: Screen marathons, fans, vents, low humidity, contact lens wear.
- Relief window: What helps within 5 to 20 minutes?
Symptom fingerprint: gritty vs burning vs “sandpaper blink”
People describe this as “sand,” “ash,” “pins,” or “paper cut on blink.” Grittiness and fluctuating blur often point to tear-film instability. Burning can overlap with inflammation. Watery eyes can still mean dryness, because reflex tearing is poor-quality lubrication. That paradox confuses almost everyone the first time.
I once had a reader write, “My eyes are dry and watery at the same time, so I assumed it was impossible.” It is not impossible. It is common.
Let’s be honest… most people miss the timing clue
If the worst symptoms reliably show up between 3 p.m. and 10 p.m., that pattern matters. It often reflects cumulative evaporation, reduced blink rate, and medication effects stacked with environment. The clue is not drama. It is data.
- Track onset time for 7 days
- Log top 2 triggers only
- Record what relieves symptoms within 20 minutes
Apply in 60 seconds: Put a recurring 3 p.m. phone prompt: “Eyes 0-10, blur yes/no, trigger now?”
Mechanism First: How These Medications Dry the Ocular Surface
Anticholinergic load and reduced tear secretion
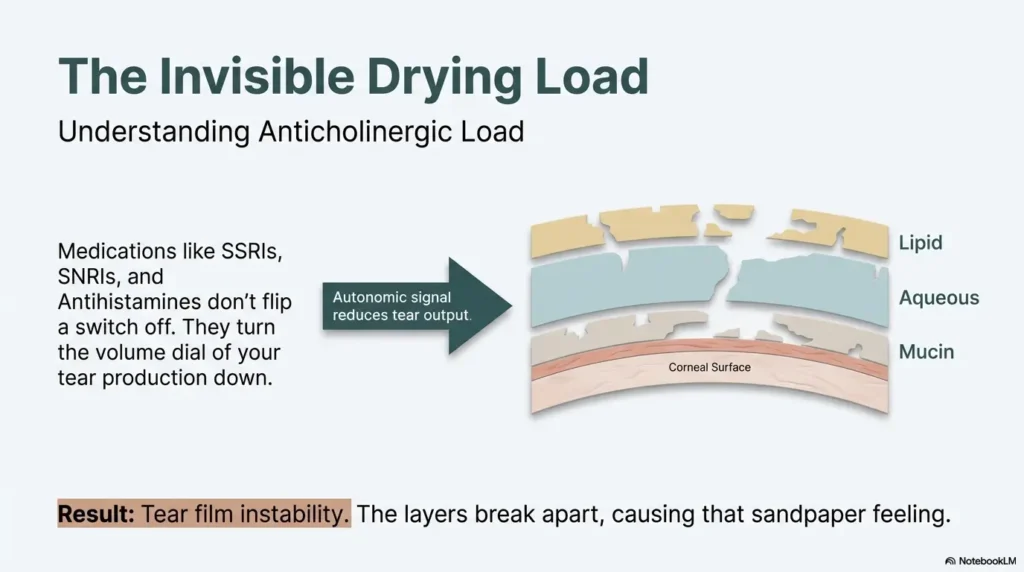
Not all dryness comes from one switch flipping off. For many people, tear production drops when medication burden nudges autonomic signaling toward less gland output. Anticholinergic effects are especially relevant here. Sometimes the culprit is not one medicine, but the total drying load across prescriptions and over-the-counter products.
Tear-film breakup: lipid, aqueous, and mucin imbalance
Your tear film is a layered system, not a puddle. If lipid quality is weak, tears evaporate faster. If aqueous volume drops, the surface dehydrates. If mucin behavior is off, tear spread gets patchy. The result can be identical symptoms from different mechanisms, which is why “just use any drop” often fails.
Why screens make medication dryness feel 2x worse
When attention narrows, blink rate falls. Less blinking means less tear distribution, faster breakup, and more friction at the ocular surface. Add medication-related vulnerability and you get the evening spiral: blur, burn, blink, repeat. If you want a practical companion guide, see this deep dive on digital eye strain patterns and screen-related dryness.
Show me the nerdy details
Dry eye is often a mixed mechanism condition involving reduced tear volume and/or increased evaporation. Practical management works best when symptom timing is paired with mechanism clues such as evaporative triggers, blink behavior, and medication profile.
Antidepressants Under the Microscope: Which Classes Raise Risk
SSRIs/SNRIs: common pattern and symptom variability
Some patients on SSRIs or SNRIs notice fluctuating dryness, blur that comes and goes, or increased sensitivity to screen time. Others feel almost nothing ocularly. Both are normal outcomes. Biology is not polite enough to be uniform.
A practical point: side effects can appear after initiation, dose adjustment, or during periods of sleep disruption and heavy digital load. The medication may be stable, but your context changes.
TCAs and higher anticholinergic burden
Tricyclic antidepressants can carry stronger anticholinergic effects for some people, which may increase dryness burden. This does not mean bad medication. It means your eye surface may need a more structured support plan while mental-health treatment goals remain protected.
Dose changes, recent starts, and delayed symptom onset
People expect immediate cause and effect. Real life is messier. Sometimes dry-eye symptoms surface weeks later because additional factors enter the frame: allergy season, dehydration, new HVAC airflow, or contact lens overuse. The timeline can be delayed without being imaginary.
Decision Card: When to discuss medication alternatives
- A: Symptoms mild, manageable with scheduled tears and environment fixes → continue current plan, monitor 7 days.
- B: Daily functional impact (reading, driving at night, lens intolerance) despite consistent reset plan → book prescriber review.
Neutral action: Bring your exact symptom timeline, not just “my eyes are bad.”
Antihistamines and the “Allergy Paradox”: Breathing Better, Seeing Worse
First-gen vs second-gen antihistamines: practical differences
First-generation antihistamines are more likely to feel drying and sedating for many users. Second-generation options are often better tolerated, but less drying does not mean never drying. If your nose finally calms down while your eyes feel scratchier, you are not making it up. A side-by-side comparison can help here: how common allergy medications differ for dry-eye symptoms.
Oral vs topical allergy meds and ocular side effects
Oral agents affect the whole system. Topical products may localize effects, but preservatives and frequency still matter. Some users do well with tailored combinations, others need simplification. Pharmacy and clinician review is the fastest path out of trial-and-error chaos.
Why seasonal dryness can persist after pollen season
Because the drivers can persist: indoor air, chronic screen load, eyelid margin inflammation, and ongoing medication profile. Seasonal trigger, year-round aftermath. That pattern is common in practice and deeply frustrating if you expect symptoms to vanish with the pollen count.
- Breathing better can coexist with ocular dryness
- Route and formulation matter
- Simpler regimens often improve adherence
Apply in 60 seconds: Write down every allergy product you use, including as-needed items, then bring that list to your review.
Stack Effect Alert: When Multiple Mild Drying Factors Become One Big Problem
Polypharmacy + caffeine + indoor air + low blink rate
One factor is a drizzle. Five factors are a storm. Medication effects can combine with caffeine load, low humidity, forced-air vents, and concentrated screen work. None of these alone feels dramatic. Together, they can wreck your evening comfort and visual confidence. If caffeine is a major variable for you, it may also be useful to review safe caffeine boundaries in eye-risk contexts.
Contact lenses, CPAP airflow, and nighttime lagophthalmos
Contact lenses can amplify friction if the tear film is unstable. CPAP leaks may direct airflow toward the eyes at night. Partial eyelid closure during sleep can leave the surface exposed. Each piece is subtle. Combined, they explain the worse every evening, worse every morning cycle. If you use CPAP, this focused troubleshooting page on CPAP mask leak into the eyes is worth bookmarking.
Here’s what no one tells you… tiny contributors can snowball by evening
I remember a week when everything looked off by 8 p.m. The fix was not heroic. It was boring and effective: vent redirection, scheduled tears, screen blink cues, and lens-hour reduction. Symptoms dropped in days, not months.
Mini Calculator: Your Daily Dryness Load (quick estimate)
Give 1 point for each: screen >6 hours, direct fan/vent exposure, caffeine >2 servings, contact lens wear >8 hours, antihistamine use, antidepressant use, indoor humidity likely low.
0–2: low stack | 3–4: moderate stack | 5+: high stack likely driving symptoms.
Neutral action: If score is 5+, run the 7-day reset before assuming treatment failure.
Who This Is For / Not For
Best for: adults with new or worsening daily grittiness after medication changes
If your symptoms are persistent, function-limiting, and seem linked to medication timing, this framework is for you. It is built for self-triage and better clinical conversations, not self-diagnosis theater.
Not for: emergency eye symptoms or sudden severe visual change
Do not delay urgent care for sudden vision drop, severe pain, one-sided intense redness, trauma, or major light sensitivity. Those are same-day issues, not watch and wait issues.
Also not for: self-discontinuation plans without prescriber input
Stopping psychiatric medication suddenly can rebound symptoms or trigger withdrawal effects. Eye discomfort deserves action, but not at the cost of destabilizing core treatment.
Eligibility Checklist: Is this 7-day reset appropriate for you?
- [ ] Symptoms are chronic/daily, not sudden catastrophic
- [ ] No severe pain or sudden major vision loss
- [ ] Willing to log symptoms for 7 days
- [ ] Willing to discuss medications with clinician before any changes
Neutral action: If any emergency box is unchecked, seek urgent eye evaluation now.
Don’t Do This #1: Stopping or Splitting Prescription Doses on Your Own
Why abrupt changes can backfire (mood, allergy rebound, withdrawal)
Trying to fix the eyes fast by dose-splitting on your own can destabilize mood treatment, worsen anxiety, or cause discontinuation symptoms. It can also create false data: if five variables change at once, no one can tell what helped.
Safer conversation starters for your next medication review
- “My symptom peak is 4 p.m. to 10 p.m. after screen-heavy days. Can we review side-effect burden?”
- “Could regimen timing be adjusted without hurting treatment goals?”
- “Are lower-drying alternatives appropriate for me?”
How to ask for alternatives without derailing your treatment goals
Lead with function: reading, driving, work accuracy, contact-lens tolerance, and sleep quality. Clinicians can better balance trade-offs when impact is concrete. My eyes hurt is valid; I can no longer tolerate 2 hours of evening screen work is actionable.
Show me the nerdy details
In medication side-effect management, controlled changes preserve interpretability. One variable at a time improves safety and makes clinical decision-making faster.
Don’t Do This #2: Redness-Relief Drop Loops and Random Eye-Drop Mixing
Rebound redness and preservative irritation traps
Redness-relief drops can create a loop: quick cosmetic improvement, then rebound redness, then more use. Meanwhile, frequent preserved drops can irritate the surface. You feel treated but not better.
Preservative-free tears vs gels vs ointments: when each fits
General pattern: preservative-free tears for daytime lubrication, gels for longer surface time, ointments mainly at bedtime when blur is acceptable. If you use multiple products, simplify the schedule so adherence survives real life. For brand-agnostic setup ideas, see a practical guide to preservative-free eye drops and this 15-minute nighttime routine for dry eyes.
The label check that prevents accidental overuse
Read the front and the active ingredient line. Two different brand names can hide similar vasoconstrictors or preservatives. Many people accidentally double up.
Coverage Tier Map: Lubrication Strategy
- Tier 1: Daytime preservative-free tears on schedule
- Tier 2: Add gel for long screen blocks
- Tier 3: Night ointment if morning irritation dominates
- Tier 4: Persistent symptoms, medication review + eye exam
- Tier 5: Specialist plan for refractory disease
Neutral action: Start at the lowest tier that matches your pattern and reassess after 7 days.
Common Mistakes That Keep Symptoms Stuck
Treating allergy only, ignoring tear-film instability
Clearing the nose does not automatically stabilize the tear film. Both can matter. Many people over-focus on one and under-treat the other.
Using drops reactively instead of on a schedule
Reactive use is like watering a plant only after leaves curl. Scheduled lubrication often performs better for persistent symptoms than rescue-only dosing.
Running fans/vents directly at face during screen work
Airflow is a silent saboteur. Redirecting a vent can feel absurdly simple, but it can materially cut evening irritation.
Waiting months before reviewing meds and symptom logs
Delay creates noise. After a short, consistent trial, escalate with clear data. Faster decisions, fewer guesswork cycles. A printable template like this symptom diary format can make your tracking cleaner.
- Schedule tears, don’t chase pain spikes
- Remove airflow stressors
- Escalate with a clean 7-day log
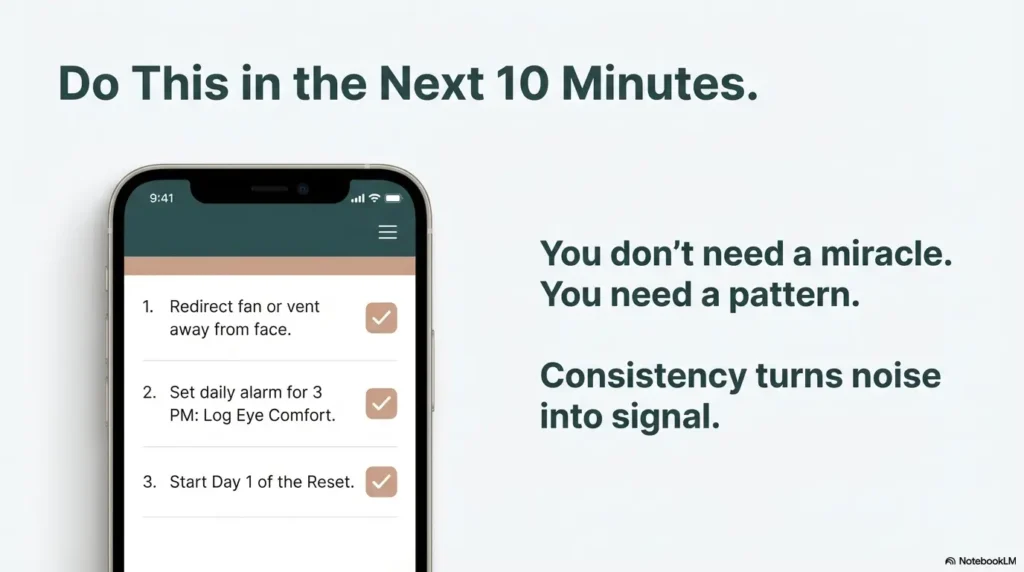
Apply in 60 seconds: Move your fan/vent direction now so airflow no longer hits your eyes.
7-Day Reset Plan: One Week to Clarify the Pattern
Day 1–2: baseline log (symptoms, meds, screen hours, environment)
Track three moments daily: morning, mid-afternoon, evening. Record symptom score (0 to 10), blur yes/no, burning yes/no, lens tolerance, screen hours, and notable exposures (fan/vent, dry room, long drive).
Day 3–5: targeted changes (humidification, blink breaks, drop timing)
Introduce only 2 to 3 interventions:
- Preservative-free tears on schedule
- 20-second blink/visual breaks every 20–30 minutes during focused screen tasks
- Humidity and airflow correction
Keep medication regimen unchanged unless directed by your clinician.
Day 6–7: decision threshold for clinic escalation
If symptoms improve by 30% or more and function returns, continue and discuss optimization at routine follow-up. If no meaningful improvement, bring the log to primary care, pharmacy consultation, or ophthalmology/optometry review. If you often wake up already irritated or blurry, also review morning blurry-vision patterns and likely causes.
Quote-Prep List: What to gather before your visit
- Complete medication and supplement list
- All eye products (bottles/tubes)
- 7-day symptom timing log
- Typical screen/work schedule
- Contact lens wear pattern
Neutral action: Put these in one bag tonight so your visit starts with clarity.
Short Story: The Tuesday-to-Tuesday reset that changed the conversation
On a gray Tuesday, one reader sent a familiar message: “I’m either dry or blurry, and by 8 p.m. I’m done.” She used an antidepressant, a seasonal antihistamine, contact lenses, and worked six to eight screen hours daily. Instead of changing everything, she changed three things for one week: preservative-free tears at fixed times, airflow redirected away from her face, and a simple 3-point symptom log.
By Thursday, evenings were still rough but less chaotic. By Sunday, blur spikes shortened. At her appointment on the next Tuesday, she brought real data, not vague frustration. Her clinician adjusted the plan safely and preserved her treatment goals. The breakthrough was not a miracle product. It was sequence, consistency, and clean information.
When to Seek Help: Red Flags and Smart Escalation
Same-day care: pain, light sensitivity, unilateral severe redness, vision drop
These are not wait and see symptoms. Immediate evaluation helps rule out dangerous causes that can masquerade as dry eye early on.
Prompt visit (1–2 weeks): persistent symptoms despite reset plan
If consistent self-care for 7 days does not improve function, escalate promptly. Bring your log and product list. The combination speeds useful decisions and avoids repetitive trial-and-error.
What to bring: medication list, symptom diary, drop products, timing notes
Think of your visit as a case handoff. Organized input improves care quality.
Infographic: 3-Step Medication-Related Dry-Eye Triage
Step 1: Pattern Check
Timing + triggers + relief window for 7 days.
Step 2: Reset Plan
Scheduled PF tears, blink breaks, airflow/humidity fixes.
Step 3: Escalate Smartly
No improvement or red flags → same-day or prompt clinic review.
Next Step: Do This Today in 10 Minutes
Build a one-page Medication + Symptom Timing sheet for your next visit
One page. Three daily check-ins. Two top triggers. One relief pattern. That is enough to change the quality of your appointment.
Pick one preservative-free tear schedule and test consistently for 7 days
Not ten products. One plan. Consistency turns noise into signal.
Book a medication review if symptoms persist past the 1-week reset
If your eyes still feel like fine grit in a contact lens case, escalate. Protect treatment goals and visual comfort at the same time. You are not choosing one over the other. If contact lenses are part of the friction loop, this can help: contact-lens dry-eye management options.
- Protect your mental-health treatment continuity
- Lower ocular surface stress systematically
- Escalate quickly if red flags or non-response appear
Apply in 60 seconds: Set tomorrow’s first reminder: “Start Day 1 eye log.”
FAQ
Can antidepressants cause dry eye even after months of stable use?
Yes, they can. Stable medication can meet unstable context: heavier screen use, seasonal allergy burden, sleep disruption, or drier indoor air. Symptoms may surface later even without a recent prescription change.
Are antihistamines or decongestants worse for eye dryness?
It depends on product class, route, dose, and your baseline tear-film vulnerability. Many people find some formulations more drying than others. A medication review with your pharmacist or clinician is the safest way to personalize this.
Should I stop my antidepressant if my eyes feel gritty every day?
No. Do not stop abruptly without prescriber guidance. Use a 7-day log and bring concrete symptom timing to your review so you can adjust safely while protecting core treatment goals.
Which artificial tears are best for medication-related dry eye?
For frequent use, preservative-free tears are often a good first step. Gels and nighttime ointments can help when symptoms persist, especially later in the day or upon waking. Matching product type to timing matters more than brand hopping.
Can dry eye from medication become permanent?
Not always. Many people improve with targeted management and medication optimization. Persistent cases do occur, which is why early structured tracking and timely escalation are important.
Why are my eyes worse at night even if mornings feel okay?
Cumulative evaporation, reduced blinking during concentrated tasks, indoor airflow, and medication-related vulnerability can stack through the day. Evening worsening is a common pattern.
Do blue-light glasses help medication-related dry eye symptoms?
They may reduce visual strain for some users, but they do not directly fix tear-film instability. Treat them as optional comfort tools, not primary dry-eye treatment. If sleep timing is also off, this companion article on blue-light glasses and insomnia adds useful context.
Is contact lens wear safe while adjusting dry-eye treatment?
Sometimes yes, but tolerance can drop during flare periods. Reducing wear time and using a clinician-approved lens and lubrication strategy is often safer than forcing full-day wear.
Can allergy eye drops and antidepressants interact with each other?
Potentially, depending on ingredients and overall regimen complexity. Bring all products to your review, including nonprescription drops, so interaction and side-effect burden can be assessed accurately.
When should I see an ophthalmologist vs primary care?
If symptoms are persistent or function-limiting despite a short reset plan, either primary care or optometry/ophthalmology can start evaluation. Go same-day for red-flag symptoms like severe pain, sudden vision loss, trauma, or marked light sensitivity.
Conclusion: Close the Loop, Keep the Plan
We started with a simple question: why do your eyes feel gritty all day. The answer is usually not one villain. It is a pattern, often medication plus environment plus behavior, repeating like a chorus you never asked to hear. The good news is practical: you can interrupt that chorus this week without risky self-experiments.
Your next 15-minute move is clear: build the one-page timing sheet, run the 7-day reset, and schedule a medication-aware review if symptoms persist. Keep your treatment goals intact. Protect your vision comfort with the same seriousness you give every other part of your health. If reading-heavy days are your biggest trigger, this guide on dry eyes from prolonged reading is a useful next stop.
Last reviewed: 2026-02.