


Family History of Eye Disease: 7 Life-Saving Lessons from My Dad’s Scary Glaucoma Wake-Up Call
The night my dad finally said the words—“Something’s wrong with my eyes”—wasn’t some dramatic, slow-motion movie moment. Nope. It happened while he was jabbing the TV remote like it had personally offended him.
“Why do they make these buttons so small?” he muttered, squinting like he was trying to read ancient hieroglyphics.
Now, if you’ve got glaucoma or serious eye problems in your family tree, you already know that particular kind of stomach-drop panic. It’s the quiet dread that sneaks in every time your mom misses a curb or your dad confuses a stop sign for a billboard. You start seeing things they don’t—and not in a psychic way.
This guide is here to help make sense of that fear. We’re going to walk through what a family history of eye disease actually means for your risk (spoiler: it’s more than just a footnote at the eye doctor’s office), how often your adult kids should get checked, and the exact questions that finally nudged my dad into that long-overdue eye exam. (Hint: guilt works. So does pretending you booked it for him “just in case.”)
We’ll get into the financial stuff—yes, including the maze that is Medicare—break down what genetics can and can’t tell you, and give you real-world checklists you can actually use today, not just pin to the fridge and forget about.
Oh, and don’t miss the quick 60-second risk estimator below. Because it’s way better to deal with this stuff now than to end up wondering why your dad’s been watching the Weather Channel in Spanish for the last three days. (True story.)
Table of Contents
Why a Family History of Eye Disease Changes Everything
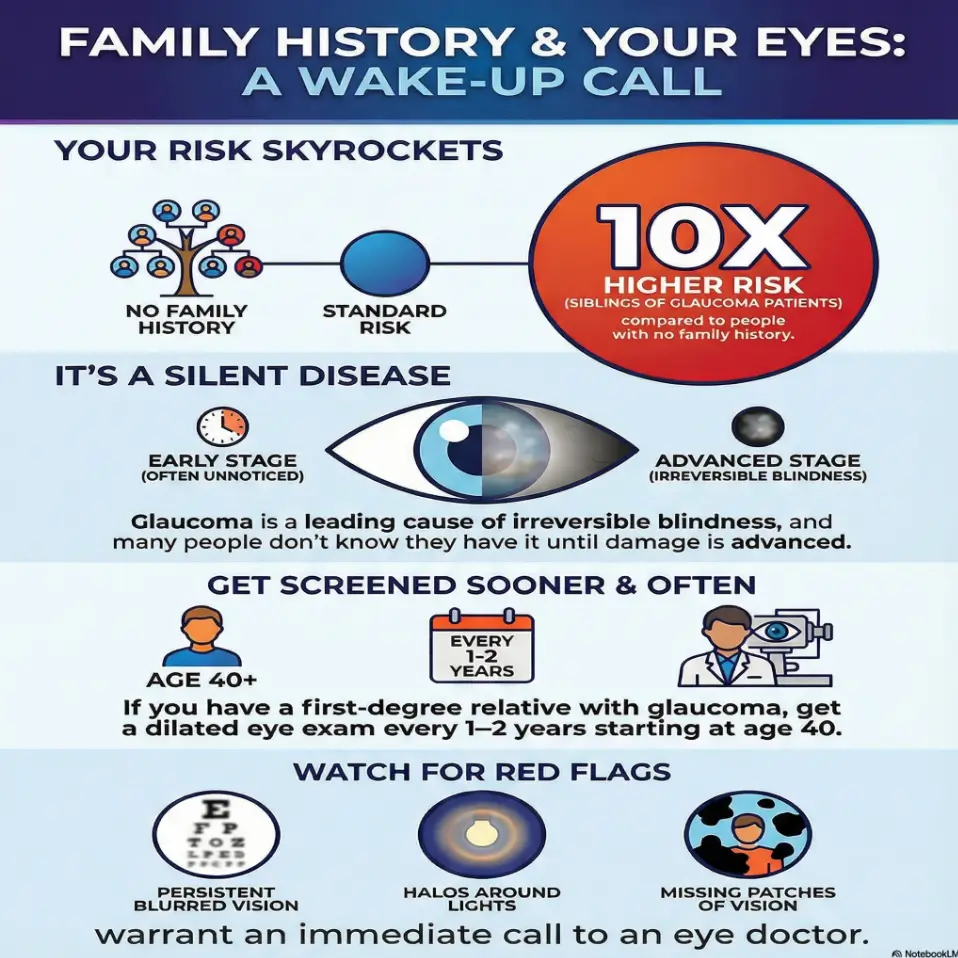
Let’s start with the uncomfortable truth: glaucoma and many serious eye diseases are both silent and hereditary. Globally, glaucoma is one of the leading causes of irreversible blindness, responsible for millions of people losing vision that will never come back. In the United States alone, about 3 million people live with glaucoma, and many don’t know they have it until damage is advanced.
Research over the last decade has hammered home the same point: if glaucoma runs in your family, your risk jumps significantly. Some large studies suggest that more than half of glaucoma cases have a familial component, with siblings of glaucoma patients sometimes facing a tenfold higher risk compared with people without that family history.
That sounds terrifying, but here’s the good part: unlike my dad, you and your adult children can act early. The optic nerve damage from glaucoma is usually slow, and regular dilated eye exams can catch it when treatment can still protect vision.
In other words, family history isn’t a curse; it’s a warning light on the dashboard. Ignoring it is like driving with the oil light on for three years. Paying attention means your family can trade guesswork for a clear schedule, a budget, and a shared language for talking about eye health.
“Family history” isn’t just a box on a form; it’s free genetic information you’d pay thousands of dollars to get from a test kit.
- Risk is higher, especially for siblings and children.
- Damage is usually silent until it’s advanced.
- Regular dilated exams turn risk into a manageable plan.
Apply in 60 seconds: Write down every relative with glaucoma or serious eye disease and their age at diagnosis—this becomes your family eye-risk map.
Lesson 1 – My Dad’s Glaucoma Wake-Up Call (and What We Missed)
My dad’s “wake-up call” didn’t look like a medical drama. It looked like him holding his mug a little closer to his face and complaining about “cheap print” on cereal boxes.
For at least two years, he blamed everything except his eyes: the lighting, his age, the TV, even the dog running into him (“He’s getting clumsy”). We had an entire family tree dotted with glaucoma and macular degeneration, and still, nobody connected those dots out loud.
The real turning point came one night when he tried to read the microwave clock and said, half-joking, “It’s like someone erased the left side of the numbers.” That sentence made the hair on my arms stand up. A week later, a comprehensive dilated exam confirmed it: glaucoma with already measurable visual field loss.
Looking back, we missed three things:
- We treated “family history of eye disease” as a boring form question, not a real risk multiplier.
- We assumed he’d “notice” if something serious was happening.
- We had no shared plan—no schedule, no checklist, no money conversation.
He was scared. I was angry—mostly at myself. But his diagnosis also became an odd kind of gift: it forced us to build a system so my siblings and I wouldn’t repeat his story in 20 years.
Apply in 60 seconds: If someone in your family already has glaucoma, pick one concrete thing they taught you—an early warning sign, a delay, a money surprise—and write it down as “Lesson 1” in your phone notes.
Lesson 2 – What “Family History of Eye Disease” Actually Means
On forms, “family history of eye disease” is usually a tiny checkbox. In real life, it’s more like a probability upgrade.
For glaucoma and other serious eye diseases, risk tends to climb when you have:
- First-degree relatives (parents, siblings, children) with glaucoma, macular degeneration, or advanced diabetic eye disease.
- Relatives diagnosed at a younger age (for example, in their 40s or 50s instead of late 70s).
- Multiple relatives on the same side of the family with similar diagnoses.
Recent large studies continue to show that family history is one of the strongest risk factors for primary open-angle glaucoma, sometimes carrying more weight than eye pressure alone.
Here’s a simple way to translate “family history” into practical risk levels for your adult children:
- Low-to-moderate – One older relative (over 75) with cataracts only; no glaucoma or macular degeneration known.
- Moderate – One first-degree relative with glaucoma or macular degeneration diagnosed after 65, or multiple second-degree relatives (grandparents, aunts/uncles).
- High – One or more first-degree relatives with glaucoma or advanced eye disease, especially if diagnosed before 65, or known severe vision loss from eye disease.
Is this perfect? Of course not. Genetics is messy. But it’s enough to stop saying, “Well, it runs in the family,” and start asking, “So what does that mean for our exam schedule, insurance, and daily habits?”
Short answer: family history should pull your whole family toward earlier and more frequent exams, not just the person who’s already diagnosed.
Apply in 60 seconds: Grab a scrap of paper and draw a quick “eye family tree”: circle each person with glaucoma or major eye disease, and star anyone diagnosed before 65.
Lesson 3 – How Often Your Adult Children Really Need Eye Exams (2025)
This is the part everyone secretly wants: “Just tell me how often my kids need to go in.”
Most major eye health organizations agree on a simple pattern: if you’re over 60 or have a family history of glaucoma, a comprehensive dilated eye exam every 1–2 years is a bare minimum. If you’re already at higher risk—because of diabetes, very high pressure, or existing optic nerve changes—your doctor may want to see you yearly or even more often.
Here’s a practical starting point for adults with a family history of serious eye disease (especially glaucoma):
- Ages 20–39: Eye exam every 3–5 years if you’re otherwise healthy; every 1–2 years if you have risk factors like diabetes or strong family history.
- Ages 40–59: Eye exam every 2 years; every year if you have a first-degree relative with glaucoma or other serious eye disease.
- 60+: Eye exam every 1–2 years for everyone; yearly or more if you have family history, diabetes, or already-documented eye changes.
Short Story: After my dad’s diagnosis, I texted my siblings a simple message: “Dad’s glaucoma is real. We’re officially a high-risk family. Please schedule a full eye exam this month.” One brother replied with a thumbs-up emoji and a photo of his crowded calendar. Two weeks later he ended up in the exam chair, annoyed but compliant.
The optometrist found borderline high pressure and early nerve changes—not a crisis, but enough to change his follow-up plan from “see you in a few years” to “let’s do this annually.” He walked out a little shaken but weirdly grateful. That one text turned a vague family fear into three concrete appointments and a shared sense that we were, finally, taking our eyes seriously.
Apply in 60 seconds: Text your closest at-risk relative: “We’re officially a high-risk eye family. When was your last dilated exam?” The awkward silence is data.
Lesson 4 – Money, Insurance, and Glaucoma Screening Costs in 2025 (US)
Eye disease risk is scary enough; the bill can feel even worse.
Let’s ground this in real numbers. In the US, a comprehensive eye exam without insurance typically costs somewhere between $100 and $200, with many sources quoting averages around $150–$180. Vision insurance or employer plans often drop the out-of-pocket cost to roughly $10–$40 per visit.
For glaucoma itself, treatment costs rise sharply as disease progresses—early-stage care may average a few hundred dollars per year, while advanced or end-stage disease can cost several times more when you add testing, medications, and possible surgery.
Here’s where your family history becomes a financial planning tool:
- If you know you’re high risk, budgeting for annual exams makes more sense than skimping until something goes wrong.
- Medicare Part B covers annual glaucoma screening for people at high risk—this explicitly includes those with a family history of glaucoma, diabetes, or certain racial/ethnic risk factors.
- Vision plans, Medicare Advantage, and some Medicaid programs can reduce both exam and treatment costs; the trick is knowing which codes and benefits to ask about.
Money Block – Coverage Tier Map for Eye Exams & Glaucoma Screening (US, 2025)
| Tier | Who You Are | Typical Out-of-Pocket | Key Action |
|---|---|---|---|
| Tier 1 | No insurance, under 60, mild risk | $100–$200 per exam | Price-shop clinics and retailers; ask for “comprehensive dilated exam” cost. |
| Tier 2 | Vision plan through employer | $10–$40 copay | Confirm frequency (often 1 exam/year) and which providers are in-network. |
| Tier 3 | Medicare Part B, high-risk (family history/diabetes) | 20% of approved amount after deductible | Ask for “Medicare glaucoma screening benefit” and verify coding before the visit. |
| Tier 4 | Medicare Advantage / premium vision plan | Varies; often low exam copay | Check if both routine exams and medical glaucoma visits are covered. |
Neutral tip: Save this table and confirm the current fee schedule and benefit details on your plan’s official website before booking.
Show me the nerdy details
Cost estimates above mash together several recent sources on eye exam pricing and glaucoma’s economic burden in the US. They reflect typical ranges, not guarantees, and real-world bills vary by state, provider type, and how your visit is coded (routine vision vs medical). The big picture is stable, though: catching glaucoma early usually costs far less per year than treating it late, especially once surgery, frequent imaging, and vision-rehabilitation services enter the picture.
Apply in 60 seconds: Look at your card: do you have a vision plan, Medicare Part B, or neither? Note the phone number on the back and bookmark it as “Eye coverage” on your phone.
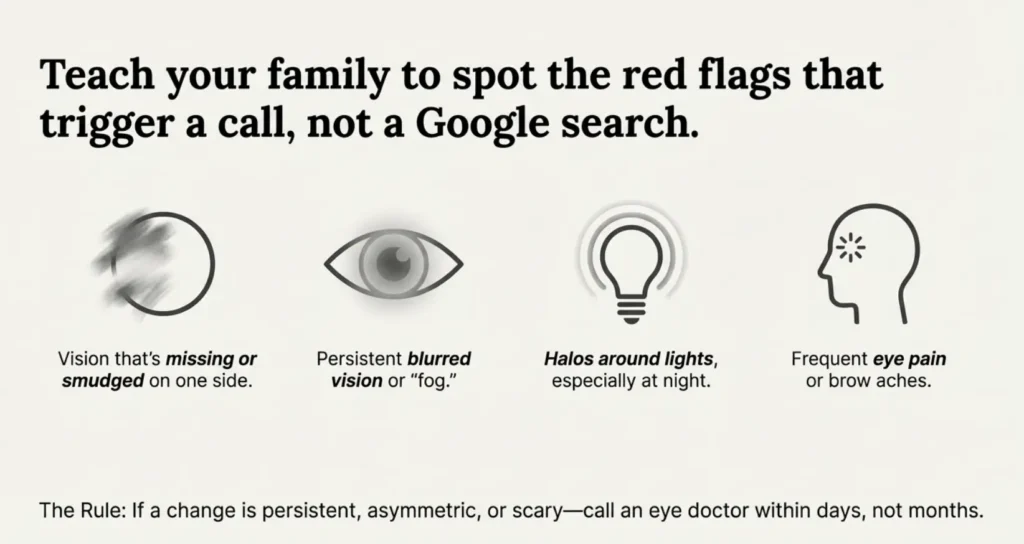
Lesson 5 – Teaching Your Family to Spot Red-Flag Symptoms Early
Here’s the trap: glaucoma is often called the “silent thief of sight” for a reason—many people notice nothing until damage is significant. That said, there are warning signs your family should treat as “call the eye doctor, not Dr. Google.”
Red flags that deserve attention:
- Vision that seems missing or smudged on one side (like my dad’s microwave digits).
- Persistent blurred vision or “fog” that doesn’t clear with blinking.
- Halos around lights, especially at night.
- Frequent eye pain, headaches, or brow aches with no clear cause.
- Sudden changes in vision, like a curtain, dark patch, or tunnel vision.
For your adult kids, the messaging sweet spot is: “We don’t want to panic over every dry-eye day. But if you notice changes that are persistent, asymmetric, or scary, call an eye doctor within days—not months.”
For your older relatives, especially those over 70, combine symptom awareness with routine exams. If you want a deeper dive into age-related risk, you can send them to this article on how often older adults should get dilated eye exams:
Apply in 60 seconds: Pick one red-flag symptom and tell your family group chat: “If anyone ever notices this, we agree you’ll call an eye doctor within a week, okay?”
Lesson 6 – Building a Family Eye-Health Plan in 60 Minutes
Think of this as your family eye-health “fire drill”. One quiet evening, you sit down with a calendar, insurance cards, and maybe one slightly suspicious teenager, and you build a simple plan around four pillars:
- Who’s high risk? Use your family tree notes: anyone with first-degree relatives who have glaucoma, macular degeneration, or severe diabetic eye disease goes on the “high-risk” list.
- Who has a doctor? Some relatives already have an optometrist or ophthalmologist; others haven’t had an exam in a decade. Make a list.
- Who has coverage? Note who has employer insurance, Medicare, Medicaid, or no coverage yet.
- Who’s overdue? Anyone over 40 who hasn’t had a proper exam in 2+ years (or 1+ year if high risk) gets a star next to their name.
Money Block – 60-Second Eligibility Checklist (US Medicare Focus)
You’re likely eligible for Medicare-covered glaucoma screening if:
- You have Medicare Part B and at least one of the following:
- Family history of glaucoma (parent, sibling, child).
- Diabetes.
- Are Black and 50+ or Hispanic and 65+.
Yes to Part B + any bullet? Ask for “the annual glaucoma screening benefit” when booking.
Neutral tip: Save this checklist and confirm the current eligibility rules on Medicare’s official site or your plan portal—they can change year to year.
Show me the nerdy details
Medicare’s glaucoma screening benefit is a medical service, not a routine vision exam. That means it’s billed differently and may involve different copays or coinsurance than a standard “check my glasses prescription” visit. The exact coding (and your out-of-pocket share) depends on whether the visit is primarily screening or active disease management. This is why it helps to ask explicitly how your exam will be billed before you go in.
For families outside the US, the logic stays the same even if the bureaucracy changes: who is high risk, who is overdue, and who has access to subsidized exams. In countries with national health systems, your general practitioner or local clinic can usually clarify how often high-risk adults should be seen and where low-cost screening is available.
Apply in 60 seconds: Make a three-column note: “High risk / Has doctor / Overdue.” Put each family member in at least one column and circle the first person you’ll help.
Lesson 7 – When to Push for a Second Opinion or Specialist
Once serious eye disease enters your family vocabulary, you’ll eventually hit the awkward moment: “My doctor says it’s normal aging, but my gut isn’t sure.”
Here are times when a second opinion from another optometrist or a fellowship-trained ophthalmologist is completely reasonable:
- There’s a strong family history of glaucoma, but you’re told “everything is fine” without a clear explanation of optic nerve appearance, eye pressure, or visual field results.
- You’re seeing new visual changes (missing patches, fog, halos) and are told “it’s probably just age” without any dilated exam or imaging.
- Your exam intervals feel too long for your comfort (for example, “come back in five years” despite high-risk status).
Money Block – Decision Card: Optometrist vs Ophthalmologist vs Emergency Room
- Optometrist (routine/monitoring): Great for annual exams, monitoring stable risk, and flagging suspicious changes.
- Ophthalmologist (medical/surgical): Best when glaucoma is suspected or diagnosed, or when you need detailed imaging and treatment decisions.
- Emergency room / urgent care: Sudden severe pain, nausea, halos, or sudden major vision loss—do not wait for a routine appointment.
Neutral tip: Save this card and ask your current provider which category your current situation belongs to—get that answer in writing if possible.
If you want help sorting “normal aging” from “please check this thoroughly,” this article about glaucoma versus normal aging signs can give your family more language to use with doctors:
Apply in 60 seconds: If something about your last eye exam felt rushed or vague, jot down three questions you’ll ask clearly at your next visit.
Infographic – Family History Roadmap: What to Do at Every Decade
Family History of Eye Disease Roadmap
20s–30s
- Ask parents/grandparents about diagnoses.
- Get a baseline exam by 30 (or sooner if high risk).
- Start a shared “family eye history” note.
40s–50s
- Schedule exams at least every 2 years.
- High-risk: move to annual exams.
- Discuss insurance and coverage tiers.
60s–70s
- Annual dilated exams for everyone.
- Use Medicare/other coverage for screening.
- Watch for red-flag symptoms daily.
80+
- Ensure exams remain yearly (or as advised).
- Plan support for transport and follow-up.
- Talk openly about fall risk and low-vision aids.
Use it like this: Find your age box, then add one line for your unique risk (family history, diabetes, or other conditions). That’s your starting plan.
Money Block – 60-Second Family Glaucoma Risk Estimator (Not Medical Advice)
This simple tool is for conversation, not diagnosis. It just helps your family talk about risk and exam timing.
This calculator doesn’t diagnose or rule out disease. It’s a conversation starter to bring to your eye-care professional.
Neutral tip: Screenshot your result and show it at your next appointment; ask if your exam schedule matches your risk.
Apply in 60 seconds: Plug in your age, relatives, and last-exam year in the mini calculator, then write down one concrete follow-up step.
FAQ
1. If glaucoma runs in my family, what age should my kids start getting eye exams?
For most children, basic vision screening starts in early school years anyway. In families with serious eye disease, it’s wise to mention your family history to your pediatrician or pediatric eye doctor and ensure a more formal exam happens in late childhood or early teens.
From around age 18–20, your kids should have a proper comprehensive eye exam, and if they’re high risk, every 1–2 years after that. The exact timing depends on other factors like diabetes or high prescriptions, so use this as a baseline, not a rigid rule. In the next 60 seconds: Add a reminder to your calendar for your child’s next exam window and note “family history of eye disease” in the description.
2. How often should someone with a family history of eye disease get a dilated exam?
For adults with a meaningful family history—especially first-degree relatives with glaucoma or other serious eye diseases—annual or every 1–2-year dilated exams are usually recommended once they reach midlife. Younger adults may be able to stretch to every 2–3 years if they’re otherwise low risk, but many eye doctors now prefer yearly exams for anyone with significant risk factors.
The safest rule: ask your provider, “If I were your sibling with this family history, how often would you bring me in?” In the next 60 seconds: Write down the date of your last dilated exam and count how many years it’s been; if it’s more than two, plan to call a clinic.
3. Does Medicare cover glaucoma screening if I have a family history?
Yes—if you have Medicare Part B and are considered high risk, Medicare generally covers one glaucoma screening exam every 12 months. High-risk groups include people with a family history of glaucoma, diabetes, and certain racial or ethnic risk groups, but you’ll still be responsible for a portion of the cost after the Part B deductible.
It’s important that the visit is coded correctly as a glaucoma screening or medically necessary exam, not simply a routine vision check. In the next 60 seconds: Flip your Medicare card and call the member services number to ask, “Am I listed as high risk for glaucoma, and what’s my expected copay for a screening exam?”
4. What symptoms mean I should call an eye doctor immediately?
While many glaucoma cases are silent, certain symptoms deserve urgent attention: sudden severe eye pain, halos around lights with nausea, rapid vision loss, or a “curtain” or dark patch falling over part of your sight. These can indicate acute glaucoma or other emergencies like retinal detachment.
Even less dramatic but persistent changes—like one-sided blur, tunnel vision, or frequent unexplained headaches—warrant a prompt phone call. When in doubt, call; eye professionals would rather see you for a false alarm than for late-stage damage. In the next 60 seconds: Save your eye doctor’s phone number in your favorites under “Eye emergency” so you’re not hunting for it when you’re scared.
5. Can lifestyle changes really lower glaucoma risk, or is it all genetics?
Genetics and family history play a powerful role, but they’re not the only story. Good blood pressure control, diabetes management, avoiding smoking, wearing eye protection, and keeping regular exams can all influence how quickly or severely eye disease progresses. You can’t meditate your way out of glaucoma, but you can avoid making things harder for your optic nerve.
Think of it this way: genes set the floor, but habits help set the ceiling. In the next 60 seconds: Choose one small habit—like a 10-minute walk after dinner or scheduling your diabetes check-up—that makes your overall eye and vascular health a little friendlier.
6. What if my parent refuses to get an eye exam even with a strong family history?
This is painfully common. Instead of arguing about risk percentages, try anchoring the conversation in what they want to protect: driving, reading, or watching grandchildren grow up. Share one concrete story (maybe this one) about someone who caught a problem early and kept independence longer.
Offer to handle the logistics—finding a clinic, booking the appointment, driving them there. Sometimes the barrier is fear of bad news or cost; naming those fears out loud can shrink them. In the next 60 seconds: Draft a short text like, “I know exams are annoying, but your eyesight matters so much to me. Can I book us a check-up together?” and send it.
Conclusion – Your Next 15 Minutes
When my dad finally sat in the exam chair and heard the word “glaucoma,” he looked less afraid of going blind and more afraid of having waited too long. That’s the quiet cruelty of family history: it’s information we often ignore until it hurts.
You now know three things many families never connect:
- Glaucoma and other serious eye diseases are common, often silent, and strongly influenced by family history.
- Regular, properly timed dilated exams—especially from midlife onward—are the closest thing we have to a safety net.
- Money, insurance, and logistics are real obstacles, but they’re easier to face before vision is lost than after.
If you want to go deeper into how age and family history shape risk, this guide on age-related eye disease can help you see the bigger picture:
Here’s a simple 15-minute plan you can start right now:
- Spend 3 minutes listing relatives with glaucoma or serious eye disease.
- Spend 5 minutes using the roadmap and mini calculator to gauge your risk level.
- Spend 7 minutes looking up one nearby eye clinic that takes your insurance—or, if you’re uninsured, one low-cost or community option.
None of this replaces medical advice, and it doesn’t guarantee perfect eyesight into your 90s. But it does something quieter and, in its own way, more powerful: it moves your family from fatalism (“it runs in the family”) to agency (“we run toward yearly exams, not away from them”).
If my dad could add one more lesson, it would probably be this: “Don’t wait until the numbers on the microwave go half-missing. Go before you’re sure you need it. That’s when it counts.”
Last reviewed: 2025-12; informed by major eye-health organizations, glaucoma research updates, and current Medicare guidance in 2024–2025. Always confirm details with your own eye-care professional and insurance provider.
Family history of eye disease, glaucoma family history, dilated eye exam schedule, Medicare glaucoma screening, blindness risk after 70