


Living with Age-Related Macular Degeneration: A Senior’s Guide to Injections, Costs, and Daily Life
If you’ve ever looked at your calendar and thought, “Wow, I didn’t plan on becoming a regular at the eye clinic,” welcome to the club no one asked to join. Age-related macular degeneration (AMD) has a way of sneaking in like a quiet thief—first it nicks the fine print on your cereal box, then it starts messing with your confidence when you’re trying to read the thermostat.
This guide is for those of us who’ve sat in too many waiting rooms flipping through outdated magazines, and for the adult children Googling “macular degeneration injections” at 1 a.m. with one eye open and mild panic setting in.
We’re keeping it real here. No sugarcoating, no vague medical jargon. Just straight answers about what treatments actually do (and don’t), what those injections really feel like, and how much this all might cost in the real world—not just on paper.
You’ll also find tips on keeping daily life doable—whether that means organizing your meds without turning your kitchen counter into a pharmacy, or figuring out how to keep your independence without needing a PhD in insurance codes.
Bottom line? This is about helping you stay in control, ask the right questions at your next appointment, and live your life without letting AMD turn it into a part-time job. Let’s get into it—because your time (and vision) is too valuable to waste.
Table of Contents
What AMD really changes (and what it doesn’t)
AMD is a disease of the macula—the part of your retina responsible for sharp, central vision. In plain terms: faces, labels, text, and fine detail are the first things to get fuzzy, distorted, or missing. But here’s the piece that doesn’t get said enough: AMD typically does not erase your peripheral vision. That distinction matters because it reframes the goal. This isn’t a story of total darkness. It’s a story of adapting your “detail system” and protecting your independence.
My favorite way to explain this to friends is unscientific but accurate: it’s like a camera with a smudged center lens but a clean outer ring. You can still navigate a room, but reading spice labels becomes a scavenger hunt with higher emotional stakes than anyone deserves.
- Expect difficulty with reading, faces, driving, and fine contrast
- Use peripheral vision and tools to keep independence
- Track small changes early—it saves time and worry later
Apply in 60 seconds: Put a high-contrast label on two everyday items you frequently misread.
Show me the nerdy details
The macula contains a high density of cones needed for color and sharp resolution. Damage here produces distortion (metamorphopsia) and central scotomas even when overall “vision numbers” look deceptively stable.
Wet vs. dry AMD: fast clarity for busy brains
This is the fork in the road that shapes everything that follows.
- Dry AMD is more common. It tends to progress slowly, often over years. Some people remain stable for long stretches.
- Wet AMD is less common but more urgent. Abnormal blood vessels grow and leak, causing faster damage to central vision.
If your doctor is recommending injections, that usually means you have wet AMD or evidence of abnormal vessel activity. The emotional whiplash here is real: one week you’re squinting at a menu; the next week someone is discussing needles near your eyeball with the calm tone of a barista asking if you want oat milk.
A short personal note: I once heard a patient in the waiting room say, “I can handle taxes, grief, and my daughter’s new boyfriend. But the word ‘injection’ near my eye? That’s where I become a poet of panic.” Honestly, fair.
Injections: what to expect in 2025 (without the scary fog)
Anti-VEGF injections are the mainstay treatment for wet AMD. The goal is to stop or slow leaky blood vessels that threaten central vision. The most common medications include aflibercept, ranibizumab, bevacizumab, and newer options designed to extend dosing intervals for some patients.
The process is usually quick. The clinic uses numbing drops and antiseptic. You’ll feel pressure more than pain. The appointment may take 30–60 minutes, but the injection itself is often over in seconds. The waiting and mental buildup is the real boss fight.
Two practical truths that calm people down:
- You are not expected to be brave in a cinematic way. You just need to show up.
- The routine becomes familiar faster than you think—usually within 2–3 visits.
One gentle joke I’ve heard from a seasoned patient: “By the third injection, I was less afraid of the needle and more annoyed by the parking situation.” That’s not minimizing fear—it’s a sign of adaptation.
Show me the nerdy details
VEGF promotes new blood vessel formation. In wet AMD, inhibiting VEGF reduces neovascular leakage and retinal swelling, stabilizing the macula’s microenvironment and preserving photoreceptor function.
How often do injections happen—and for how long?
In the beginning, many treatment plans use a “loading phase,” often monthly injections for about 3 months. After that, your retina specialist may shift to:
- Treat-and-extend (gradually spacing visits if the eye stays stable)
- Fixed interval (every 4, 8, 12+ weeks depending on response)
- As needed in select cases, with careful monitoring
Here’s the part that matters for daily life planning: this is usually a long game. Some people need ongoing injections for years. The goal is to preserve vision and maintain function, not to promise a one-and-done cure.
Think of it like managing blood pressure. You don’t “finish” the condition. You build a stable routine that keeps your future self safer.
- Many start with monthly visits for ~3 months
- Intervals may extend to 8–12+ weeks
- Consistency protects your long-term independence
Apply in 60 seconds: Add a recurring calendar event titled “Vision protection day” so injections feel like a routine, not an emergency.

Costs, insurance, and out-of-pocket reality
Let’s talk about the part nobody wants to say out loud: the money math can be exhausting. Anti-VEGF drugs range widely in price depending on which medication your doctor uses and how your healthcare system or insurer reimburses it. In the U.S., for example, Medicare often covers approved treatments for wet AMD, but patients can still face coinsurance depending on supplemental coverage. In other countries, national health systems may cover specific drugs under eligibility criteria.
Even without listing exact price tags, what you need to know is this: the difference between medications can mean a meaningful difference in out-of-pocket costs. That’s not a reason to pressure your doctor; it’s a reason to ask a simple, respectful question:
“Is there a clinically appropriate option with a lower out-of-pocket burden for me?”
That single sentence can save hours of confusion and hundreds—or thousands—over a year.
Decision card: When A vs. B (time/cost trade-off)
- Potentially fewer visits per year
- Higher per-dose cost
- May reduce caregiver and transportation strain
- Lower per-dose cost
- Intervals may be shorter depending on response
- Can be a solid choice when clinically appropriate
Neutral next step: Ask your clinic for a written estimate that lists the drug name, expected interval, and your projected annual share.
Eligibility checklist for coverage and approvals
If your brain goes foggy the moment someone says “prior authorization,” you’re in good company. This is the part where even competent adults become helpless toddlers with paperwork.
Eligibility checklist (quick yes/no)
- Do you have a confirmed diagnosis of wet AMD? Yes/No
- Has imaging (like OCT or angiography) documented active leakage or abnormal vessels? Yes/No
- Has your doctor documented why this specific medication is appropriate for you? Yes/No
- Do you have your insurance details and any supplemental plan info ready? Yes/No
Neutral next step: If you answered “No” to any item, ask your clinic’s billing team for a one-page summary you can keep in your records.
Quote-prep list: what to gather before comparing
- Diagnosis wording from your visit summary
- Planned medication name
- Expected injection interval after the first 3 months
- Insurance plan and supplemental details
- Clinic’s billing contact email or phone
Neutral next step: Save a screenshot of your plan benefits and bring it to your next visit.
A 60-second annual vision budget estimator
This is a simple planning tool—not a bill prediction. The goal is to help you avoid financial surprises and set a calm baseline for the year.
Mini calculator (estimate your annual routine costs)
Estimated annual routine total: —
Neutral next step: Save this number and confirm your current benefits with your insurer or clinic billing team.
Daily life tweaks that truly help
AMD doesn’t just change what you see; it changes what you avoid. People stop reading menus, driving at dusk, or recognizing faces in crowded places—not because they can’t do it, but because the effort feels humiliating. That quiet avoidance is where life shrinks.
So we widen life again with small, stubborn tools.
Five high-value adjustments
- Lighting upgrades: A bright, adjustable lamp can reduce frustration by an absurd amount.
- High-contrast settings on phones and tablets.
- Large-print labels for medications and pantry staples.
- Magnification tools for reading short bursts.
- Voice-first habits: audiobooks, smart assistants, dictation.
One personal micro-moment: I once watched someone with AMD label spices in bold black letters. It looked like an overachieving kindergarten craft project. It also turned dinner from stressful to joyful in about 10 minutes. That’s a trade I will take every time.
- Lighting is your first upgrade
- Contrast beats tiny fonts
- Voice tools reduce fatigue
Apply in 60 seconds: Turn on bold text and high contrast on your phone right now.
Show me the nerdy details
Contrast sensitivity often declines with macular disease. Enhancing luminance and edge definition reduces cognitive load and improves functional reading speed more than many people expect.
Short Story: The appointment that rewired my fear (120–180 words) …
Short Story: I met a retired teacher in the injection waiting room who carried a small notebook labeled “Tiny Wins.” She wasn’t dramatic about it. She just wrote one line after every visit. “Drove myself here.” “Asked the scary question.” “Read a grandkid’s text without help.” On the day I was visibly nervous, she slid the notebook toward me like it was a secret menu item.
She said the first injection felt like stepping onto a stage without rehearsal. The second felt like a chore. The third felt like insurance for the life she still wanted. She didn’t pretend it was easy; she just refused to let fear become the main character. When the nurse called her name, she stood up, smiled, and said, “Let’s protect the plot.” I stole that line for my own brain and I’m not sorry.
A quick regional reality check: U.S. Medicare vs. South Korea’s system
If you’re reading this in the U.S., coverage for AMD injections often hinges on documented wet AMD activity and the specifics of your Medicare plan plus any supplemental insurance. Your clinic’s coding and documentation can meaningfully affect what you owe.
If you’re reading from South Korea, the National Health Insurance system has historically covered anti-VEGF treatment under defined clinical criteria and documentation requirements. In practice, that means the biggest “cost leverage” may come from meeting eligibility rules, keeping imaging and visit records organized, and confirming how many injections are covered within a given period under current policy — and noting any family history of eye disease that clinicians ask about.
Neutral next step: Ask your clinic for a concise statement of your diagnosis, imaging results, and the medication plan to keep coverage conversations simple and accurate.
What to watch between visits (so you don’t spiral)
Not every odd visual moment is an emergency, but some changes deserve fast attention.
- Sudden increase in distortion (straight lines bending more)
- New dark or blurry spot in central vision
- Rapid drop in reading clarity over days
- New difficulty recognizing faces
A simple at-home habit like using an Amsler grid can help you notice changes earlier. The key is not to turn this into a daily anxiety ritual. Think of it as checking the smoke detector—not staring at the toaster waiting for drama. And don’t skip regular dilated eye exams—they catch quiet shifts you might miss.
A practical cost-and-visit planning table
Exact prices vary by country, insurer, clinic, and medication. But the structure of your planning can still be consistent. Use this to estimate your time and logistics load for the year.
| Year | Typical visit rhythm | Time commitment | Budget notes |
|---|---|---|---|
| 2025 | Loading phase + treat-and-extend for many | Often 6–12 visits/year depending on response | Out-of-pocket varies widely by medication and coverage |
| 2026 | Stabilization phase for responders | Some may extend to 8–12+ week intervals | Transportation and caregiver time become key hidden costs |
Neutral next step: Download or copy this table into your notes and confirm your current coverage details with your provider’s billing team.
A caregiver playbook that won’t burn you out
Adult children often become the quiet operations team for AMD care. You schedule, drive, read forms, and absorb fear that isn’t even yours. It’s love, but it’s also labor.
Three small structures can keep this sustainable:
- One shared note with medication name, last injection date, next planned interval.
- One clinic contact saved for billing questions.
- One “good day” ritual after appointments—lunch, a walk, or a small treat that reframes the day as life-first.
Humor helps more than we admit. I’ve seen a family call injection days “macula maintenance Mondays,” even when it wasn’t Monday. The point wasn’t accuracy. The point was control.
Show me the nerdy details
Caregiver strain often comes from unpredictable schedules and unclear expectations. A stable treat-and-extend plan, when clinically appropriate, can reduce logistic burden and improve adherence.
Side effects, red flags, and when to call
Most people experience mild irritation, tearing, or a gritty sensation for a day or two. Occasional small floaters can happen. But you should contact your clinic urgently if you notice:
- Severe pain
- Significant redness with worsening vision
- Light sensitivity that escalates
- A sudden curtain-like shadow
These can be signs of uncommon but serious complications that need fast evaluation.
A moment to ground your decisions in trusted guidance
When the internet gets loud, your best anchor is plain-language guidance from major eye and public health institutions. If you want a deep, reputable overview you can share with family, this is a good starting point.
Driving, reading, and the identity shock
For many seniors, the most painful loss isn’t the blur—it’s the symbolism. Driving represents autonomy. Reading represents selfhood. When either becomes hard, people can feel like they’re “shrinking.”
Two gentle truths that preserve dignity:
- Choosing not to drive at night is strategy, not surrender.
- Switching formats is not “giving up reading.” It’s expanding it.
A friend once said, “I didn’t quit books. I just changed the instrument.” She moved to audiobooks, then to large-print, then to short essays with strong contrast. Her reading life became different, not smaller.
- Use daylight driving rules
- Adopt multi-format reading
- Ask for vision rehab early
Apply in 60 seconds: Download one audiobook you’ve always wanted to read but never had time for.
Vision rehab and low-vision tools worth knowing
Low-vision rehabilitation can be the difference between “I can’t do this anymore” and “I can do this differently.” This may include occupational therapy strategies, devices, and training that helps your brain and environment cooperate.
High-value tools include:
- Electronic magnifiers
- Text-to-speech apps
- High-contrast keyboards and labels
- Task lighting and glare control
Time saved is real here. A properly set-up home environment can cut daily frustration by 15–30 minutes, which quietly adds up to better mood and more energy for the things you actually enjoy. Keep preventative care steady with an annual eye exam checklist for seniors so changes get caught early.
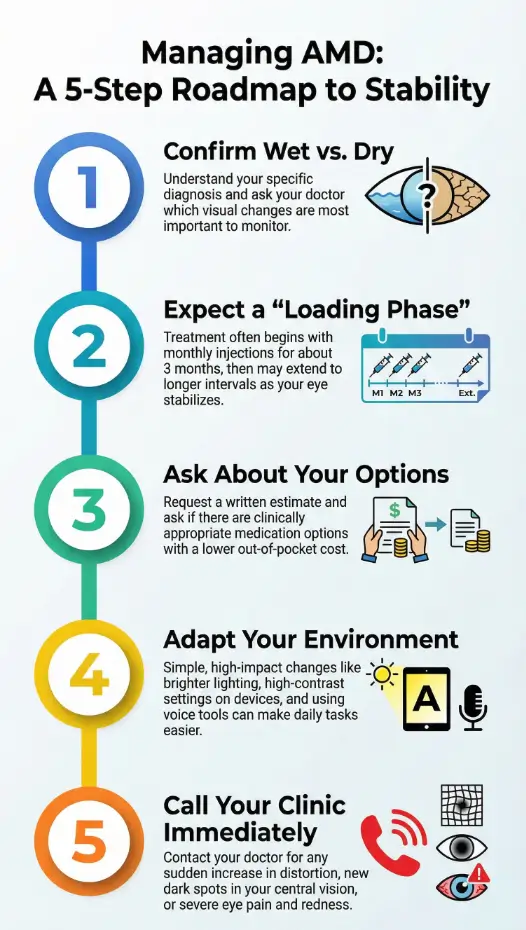
Infographic: the calm roadmap from diagnosis to daily stability
- Confirm wet vs. dry
- Get imaging summary
- Ask “What changes fast?”
- Expect 3-month loading phase
- Shift to treat-and-extend if stable
- Track dates in one note
- Request written estimates
- Check coinsurance rules
- Compare clinically appropriate options
- Lighting + contrast first
- Label meds and pantry
- Use voice tools
- Sudden distortion increase
- New central dark spot
- Severe pain or redness
Neutral next step: Save this roadmap, then ask your clinic to confirm your current schedule and coverage requirements.
What to do when vision changes fast
When wet AMD flares or new bleeding occurs, hours and days matter more than weeks. You don’t need to diagnose yourself—you just need a plan.
- Call your retina clinic and say: “I have a sudden change in central vision.”
- Note the date and what you observed (distortion, new spot, rapid blur).
- If your clinic is unreachable and symptoms are severe, seek urgent eye evaluation.
This is not catastrophizing. This is the grown-up version of wearing a seatbelt.
Official professional guidance for injections and follow-up care
For a reputable clinical overview you can bring to an appointment, this professional resource is a steady reference point.
Coverage and benefits context for readers navigating U.S. insurance
If you’re dealing with Medicare or supplemental policies, reviewing official benefit explanations can reduce surprises and help you ask sharper questions.
FAQ
Do AMD injections hurt?
Most people describe pressure more than pain because of numbing drops. The anxiety beforehand is usually worse than the injection itself. Apply in 60 seconds: Ask your clinic what comfort steps they use so you walk in with a clear expectation.
How many injections will I need?
Many patients start with about 3 monthly injections, then move to a customized schedule. Some continue for years to keep the disease controlled. Apply in 60 seconds: Write down your last injection date and ask your doctor what your likely interval is after the loading phase.
Can dry AMD turn into wet AMD?
Yes, it can. That’s why monitoring and reporting new distortion or central blurring matters. Apply in 60 seconds: Keep an Amsler grid or a simple “straight-line check” routine once or twice a week.
Will Medicare or insurance cover my injections?
Coverage often depends on documented wet AMD activity and the specific medication plan. Supplemental insurance can change your out-of-pocket share. Apply in 60 seconds: Request a written estimate based on your exact drug and interval.
What if I miss an injection appointment?
One missed visit isn’t automatically catastrophic, but repeated delays can raise the risk of vision loss. Contact your clinic quickly to reschedule. Apply in 60 seconds: Set a backup transportation plan for injection days.
Are there lifestyle changes that help?
Healthy diet patterns, smoking avoidance, and managing cardiovascular risk can support overall eye health. For some forms of dry AMD, specific eye vitamins may be discussed with your clinician. If you live with diabetes, it’s also worth knowing the basics of diabetic retinopathy so you can track both conditions wisely. Apply in 60 seconds: Ask your doctor whether a vitamin formula is appropriate for your specific stage.
Your next 15 minutes: a calm, smart plan
If AMD has made your world feel smaller, here’s the quiet truth that deserves the last word: your future is still negotiable. Injections are not a punishment; they’re a strategy to protect the details that make life feel like yours—faces, books, recipes, street signs, your grandkid’s grin.
Close the loop from the fear in the intro: the calendar doesn’t mean you’re losing. It means you’re fighting with a plan.
Your 15-minute next step: Open your notes app and create a simple “AMD one-pager” with (1) your diagnosis type, (2) medication name, (3) last injection date, (4) next appointment, and (5) a billing contact. Bring it to your next visit. You’ll save 20–30 minutes of confusion and feel noticeably more in control. If you prefer a ready-made format, use this printable symptom diary for seniors as your template.
Last reviewed: 2025-12; sources: National Eye Institute, American Academy of Ophthalmology, Medicare public guidance. Age-related macular degeneration, AMD injections, anti-VEGF cost, low vision tools, senior eye care