


Your contacts don’t “randomly get sensitive.”
They usually hit a predictable wall—fine at 9 a.m., then a slow, hot slide into burning by 4–6 p.m.
Miebo for MGD evaporative dry eye in contact lens wearers is built for that exact pattern: tear film that dries down too fast once screens, HVAC, wind, and low blink rate stack up. Keep guessing, and you’ll keep paying—in shorter wear time, more rescue drops, and the quiet risk of pushing through pain that should be a stop sign.
This post gives you a clean, 7-day end-of-day burn log, contact-lens timing rules that won’t sabotage results, and the common mistakes that create “it didn’t work” stories. (If your plan also includes foundations like a 15-minute night routine for dry eyes, you’ll get a cleaner signal, faster.)
Miebo (perfluorohexyloctane) is a prescription eye drop designed to reduce tear evaporation—often a key driver in MGD-related evaporative dry eye. If your eyes feel okay early but burn by late afternoon in contacts, Miebo may help by improving tear-film “stay time.” The cleanest way to know is a 7-day end-of-day burn log while keeping your lens brand/solution stable and using Miebo exactly as prescribed.
- This is general information, not medical advice. Follow your prescriber’s directions and the official labeling.
- Stop contact lens wear and seek same-day care for severe eye pain, light sensitivity, sudden vision changes, significant redness, discharge, trauma, or a “something stuck” sensation that won’t clear.
Table of Contents
End-of-day burning: why 3–8 p.m. is the clue
That “fine until afternoon, then burning” pattern is not random. It often points to tear evaporation plus accumulated stress: screen time, HVAC, low blink rate, and lenses sitting on a tear film that’s already working overtime. If you’ve ever taken your lenses out at 6 p.m. and felt immediate relief—like your eyes exhaled—your body is giving you timing data.
The timing pattern: morning okay → afternoon burn
Evaporative dry eye can feel like a slow leak. The tank starts full, then drains faster than it should. Morning comfort doesn’t rule dry eye out; it can actually be part of the signature. One of my own “tell” moments was realizing I could predict discomfort by checking the clock—like my eyes had a calendar appointment with misery.
The environment stack: screens + HVAC + low blink rate
- Screens: many people blink less, and incomplete blinks matter for meibomian gland function. (If your day is screen-heavy, the “why” often overlaps with digital eye strain patterns that worsen with low blink rate.)
- HVAC & car vents: moving air accelerates evaporation.
- Dry winter air: your tear film is negotiating with physics all day.
- Track the time symptoms start
- Note triggers (vents, screens, outdoor wind)
- Don’t change 5 variables at once
Apply in 60 seconds: Write down “first burn time” today (e.g., 4:30 p.m.).
Open loop: If it’s not evaporation… what is it, and how can you tell fast?
Keep that question. We’ll answer it in the “fast sort” section with a simple decision tree that separates MGD-likely patterns from allergy, solution sensitivity, lens fit, and urgent red flags.

Miebo first, plainly: what it’s built to do
Miebo is a prescription eye drop (perfluorohexyloctane) designed to address a specific failure mode: tears evaporating too quickly. That’s it. Not a mood. Not a personality. Not a magical reset button. It’s a tool for a particular mechanism—especially relevant when meibomian glands (the oil-producing glands along your lid margin) are underperforming.
The evaporation problem: when the lipid layer underperforms
Your tear film isn’t just “water.” It’s a layered system, and the oily layer helps slow evaporation. In MGD, that oil layer can be reduced or altered, making tears dry up faster—often worse in wind, air conditioning, and heavy screen days. (For some people, hydration and fat intake timing also matters—see diet for dry eyes after LASIK for a practical food-and-fluids angle that pairs well with an evaporation plan.)
What perfluorohexyloctane is trying to change (tear-film “stay time”)
Mechanistically, think “slower dry-down.” Practically, think: “My eyes feel less raw by evening,” or “I can wear lenses longer before discomfort starts.” Also important: the FDA-approved labeling for Miebo includes a contact lens instruction (remove lenses before use and wait before reinsertion). If you’re a lens wearer, that detail is not optional trivia—it’s part of safe use.
What it won’t fix alone (and why that’s not a “failure”)
- Poor lens fit or a lens material your eyes simply don’t love
- Overwear (hours matter more than willpower)
- Deposits from stretched replacement schedules
- Untreated allergy or lid margin inflammation (if antihistamines are part of your life, it’s worth understanding how they can play with dryness—compare options in dry eye: Claritin vs Zyrtec vs Allegra.)
Show me the nerdy details
If you want a clinician-style anchor, the “tear breakup time” concept is often used when evaluating tear film stability. A short breakup time can reflect instability that feels like late-day burning, especially with environmental triggers and contact lens wear.
Contact lenses + MGD: the friction point competitors skip
Here’s the messy truth: contacts can be both a miracle and a magnifier. They sit in the tear film, interact with it, and raise the cost of small problems. A “mild” tear instability can become “why do I hate my life at 5 p.m.?” once you add lenses.
Tear film + lens = thinner margin for error
When your tear film is already evaporating quickly, a lens can make dryness feel louder. The feeling isn’t always “dry.” It can be burning, stinging, or a hot, tight sensation that makes you blink like you’re trying to reboot your eyeballs.
The four accelerators: wear time, lens type, solution sensitivity, deposits
- Wear time: the difference between 10 hours and 14 hours can be dramatic.
- Lens type: daily disposables often reduce deposit/solution issues for some people.
- Solution sensitivity: if symptoms spike after insertion, don’t ignore the bottle.
- Deposits: “I can stretch these” is a plot twist your eyes rarely enjoy.
Pattern interrupt: Let’s be honest… your lens schedule may be the biggest variable
If you’re wearing lenses past the point of comfort because you’re busy, driving, or just stubborn (hi, it’s me), no prescription drop can outwork relentless overwear. You don’t need guilt—you need a plan that respects time, work, and your cornea. (If you also use daily glaucoma meds, the interaction between drops and lenses deserves its own attention—see glaucoma drops and contact lenses timing considerations.)
Money Block: Eligibility checklist (lens-wearer edition)
- Yes/No: Is burning worst late day (not immediately after insertion)?
- Yes/No: Do wind, car vents, or AC make it worse?
- Yes/No: Do you feel better within 10 minutes of removing lenses?
- Yes/No: Are you replacing lenses on schedule?
Next step: If you answered “Yes” to 3+, you’re a strong candidate for an evaporation-focused plan—bring this checklist to your eye visit.
Is it really MGD? A fast sort before you spend a month
Before you invest weeks in a new drop, do a quick sort. “Dry eye” is a bucket label. Your job is to figure out which subtype is driving the burn—or whether something else needs attention first. The National Eye Institute notes that dry eye can involve either not making enough tears or tears that “dry up too fast.” That second pathway matters a lot here.
Lid clues + tear breakup time basics (what a routine exam can confirm)
An eye doctor can look at your lid margins, glands, and tear film stability. Ask about tear breakup time testing and whether your presentation suggests evaporative dry eye. (If your symptoms are chronic and you’re a contact-lens wearer, it’s a reasonable question—no need to whisper.) If you want a simple “what to bring / what to ask” structure, an annual eye exam checklist is a surprisingly useful template—even if you’re not a senior.
Allergy vs dry eye: when burning rides with itch + seasonality
Allergy often brings itch and swelling; dry eye often brings gritty/burning and fluctuating vision. But overlap is real. If your worst days track pollen seasons or you rub your eyes like you’re trying to start a fire, your plan may need an allergy branch—not just an evaporation branch.
Open loop: If watery eyes are your main symptom—can it still be evaporative?
Yes. Watery eyes can be a reflex response to irritation. The “watery” part doesn’t guarantee good lubrication. This is exactly why a quick exam matters: it replaces guessing with a mechanism.
- MGD often worsens with wind/HVAC
- Allergy often worsens with itch/seasonality
- Lens fit/solution can create sharp timing clues
Apply in 60 seconds: Circle one: “burning,” “itch,” or “pain + light sensitivity.” That word changes the plan.
The 7-day Miebo test: prove it (or stop guessing)
If you do one thing from this article, do this: run a simple 7-day test that protects you from placebo, chaos, and wishful thinking. The goal is not perfection. The goal is a cleaner signal. (If you prefer something printable—especially if you’re tracking for a parent—use a printable symptom diary and treat it like your data anchor.)
Pick one outcome: burning at 6 p.m. (0–10) or hours until discomfort
Choose one metric and stick to it. I like “burning at 6 p.m.” because it’s easy and brutally honest. If you’re rarely in lenses at 6 p.m., use “hours until discomfort starts.”
Freeze your variables: same lens, same solution, same wear window
This is the part people skip—and then blame the drop. Keep your lens brand, solution, wear time, and environment as stable as possible for 7 days. You’re trying to answer one question at a time, not solve your entire life in a week.
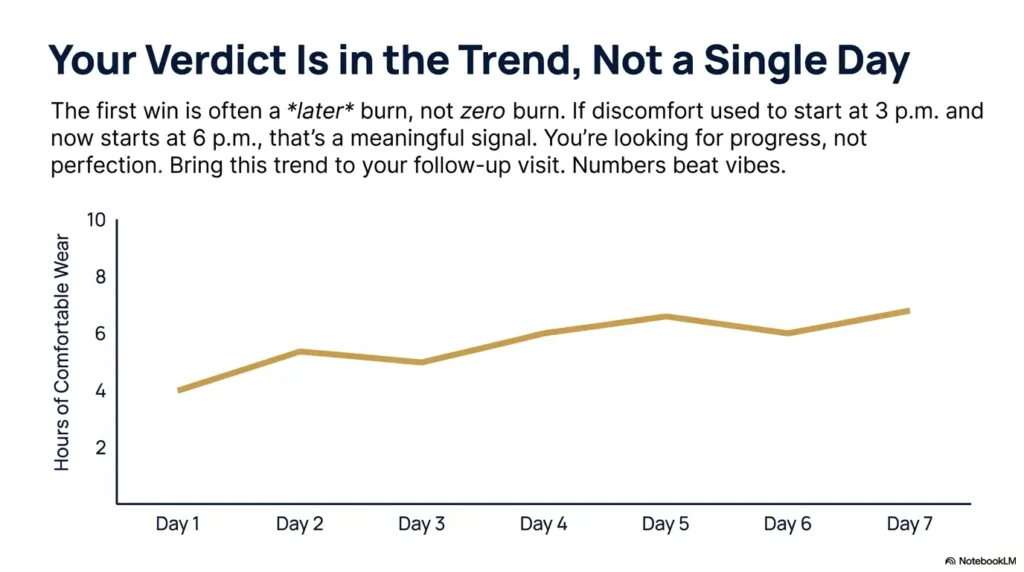
Open loop: What should improve first—intensity, onset time, or rescue-drop frequency?
Often, the first improvement is later onset: the burn starts at 6 p.m. instead of 3 p.m. That’s meaningful. It’s also easy to miss if you’re only asking, “Did it vanish?” Track what changes first—then you can tune the rest.
Money Block: Mini calculator (comfort time gain)
Estimate how much “comfortable lens time” you regained after 7 days.
Estimated gain: —
Next step: Save the result and bring it to your follow-up visit. Numbers beat vibes.
Timing with contacts: don’t sabotage your own results
This section is here because the internet is full of vague advice like “use it as directed.” You deserve something more usable than that. Here are the practical timing principles that keep your trial clean and your eyes safer.
Consistency beats “whenever it burns” (why rescue-only use fails)
Random, reactive use makes your results muddy. If you only reach for a treatment at peak discomfort, you never learn whether it prevents the problem from building in the first place.
Spacing rules if you use other drops (avoid stacking too close)
If you’re also using preservative-free artificial tears, allergy drops, or other prescriptions, don’t pile them on back-to-back without guidance. A simple rule of thumb many clinicians use is spacing drops so each one has a chance to do its job (ask your prescriber for the spacing they prefer). If you’re choosing your “rescue” option, preservative-free eye drops are often the safer default when frequency creeps up.
Pattern interrupt: Here’s what no one tells you… success may look like later burn, not zero burn
The first win may be: “I made it through my commute and my last meeting without wanting to scrape my eyeballs with a spoon.” That’s not poetic. It’s progress.
Show me the nerdy details
For contact lens wearers, labeling often includes guidance about removing lenses and waiting before reinsertion. This is about both safety and ensuring the medication is used as intended on the ocular surface rather than interacting unpredictably with lenses.
Common mistakes that create “Miebo didn’t work” stories
Let’s prevent the future you from writing an angry note in your phone titled “THIS DID NOTHING.” Most “it didn’t work” stories are actually “my experiment was un-runnable.” Here’s how to keep yours runnable.
Mistake #1: Changing lens brand/solution + drops at the same time
If you switch lenses, solutions, and start a new prescription in the same week, you’ll never know what helped—or what hurt. Change one variable at a time. You’re not being slow. You’re being scientific.
Mistake #2: Ignoring lid routine while expecting a drop to do everything
MGD is often a gland-flow problem. If your clinician has you doing warm compresses or lid hygiene, treat that as the foundation, not an optional side quest.
Mistake #3: Powering through discomfort in lenses (risk > convenience)
I’ve done it. You’ve done it. We’ve all tried to “just get through the day.” But contact lens pain can be a red flag for corneal irritation. The heroic move is sometimes taking the lenses out. (If nighttime dryness is part of your pattern—waking up gritty, not just ending the day gritty—check whether CPAP mask leak into the eyes is quietly drying you out while you sleep.)
- Keep lens brand and solution stable for 7 days
- Track one metric consistently
- Respect pain as a stop sign
Apply in 60 seconds: Put a sticky note on your mirror: “One variable this week.”
Two “don’t do this” scenarios (loss-prevention)
Because the cost of getting this wrong isn’t just discomfort. It can be delayed care. Here are two scenarios where “wait it out” is the wrong personality trait.
Don’t keep lenses in with pain + light sensitivity
Light sensitivity plus pain is not a “normal dry eye day.” Remove lenses and seek same-day evaluation. Even if it turns out to be minor, you’re protecting your cornea and your future ability to wear contacts comfortably.
Don’t self-treat discharge/redness as “just dry eye”
Significant discharge, marked redness, or sudden one-eye symptoms can suggest infection or inflammation that needs a different plan. Treat it as its own lane.
MGD stack that pairs well (when drops aren’t enough)
Most people with MGD do best with a stack—a small set of actions that work together. Think of it as a budget-friendly system: a few consistent moves that prevent late-day collapse.
Home base: heat + lid hygiene (what it’s trying to change)
Warm compresses and lid hygiene aim to improve gland flow and reduce lid margin buildup. If you do them inconsistently, results are inconsistent. (Annoying but true.) I once did “two perfect days” and expected a miracle by Friday. Spoiler: my glands were not impressed.
Escalation options: thermal pulsation / IPL—who they’re for
If conservative care isn’t enough, clinics may discuss in-office therapies like thermal pulsation or intense pulsed light (IPL) for appropriate candidates. These are not one-size-fits-all; they belong in a clinician-guided decision, often after confirming MGD severity and tear film behavior.
Where Miebo fits: evaporation control alongside gland support
If your dominant problem is rapid evaporation, an evaporation-targeted drop can complement gland-focused care. The best outcomes usually come from matching the tool to the mechanism—then actually using the tool long enough to measure it.
Money Block: Decision card (When A vs B)
| If your pattern is… | Prioritize… | Why |
|---|---|---|
| Late-day burning + wind/HVAC triggers | Evaporation-focused plan + MGD routine | Mechanism match: tears drying too fast |
| Immediate sting after insertion | Solution/lens evaluation | Timing suggests chemical/fit issue |
| Itch + seasonal flares | Allergy branch (clinician-guided) | Different driver, different tools |
Next step: Pick one “prioritize” lane and commit to it for 7 days before switching lanes.
Side effects + “It stings”: what’s normal vs not
Any new eye drop can come with an adjustment period. The goal is to distinguish “brief awareness” from “this is worsening my situation.” Words matter here—how you describe it helps your clinician help you.
Brief awareness vs persistent burning (how to describe it accurately)
- Brief awareness: mild sensation that fades quickly
- Persistent burning: lingering discomfort, increasing redness, or worsening symptoms
- Functional impact: “I had to remove lenses early” is a clinically useful sentence
When symptoms worsen instead of improve (what to report)
If symptoms intensify, your eyes look significantly red, or vision changes, contact your prescriber. Bring your log. The combination of timing + symptom change is more useful than a vague “it felt weird.”
Cost barrier in the US: what to ask about (PA, savings, alternatives)
Prescription dry eye treatments can involve insurance steps like prior authorization. Ask your clinic what they usually submit, what alternatives they consider if coverage is denied, and what timeline they expect. (This is not being difficult. This is being an adult with a budget.)
Who this is for / not for (quick self-sort)
This is the part where you either lean in or happily exit. Both are wins.
For: “My eyes burn at the end of the day”
- Contact-lens wearers with suspected/confirmed MGD and evaporative triggers (wind, screens, AC)
- People who can commit to a 7-day stable trial (same lens, same solution)
- Anyone who wants a measurable outcome, not a vibe
Not for: “This feels different”
- Severe one-eye pain, major redness, discharge, or light sensitivity
- Possible infection, corneal injury, or trauma
- Anyone planning to freestyle dosing or layer multiple drops without guidance
Short Story: The day I stopped “toughing it out” (120–180 words) …
It was a Wednesday, and I was doing the classic thing: pretending my eyes were “fine” because my calendar was not. By 3 p.m., the burning was there—subtle at first, then sharp enough that I started blinking like a stressed cartoon character. I kept the lenses in anyway, because I had one more meeting and I didn’t want to be the person who “couldn’t handle contacts.”
At 5:30 p.m., I finally took them out in the car and felt instant relief—followed by the uncomfortable realization that I’d normalized pain. The next day I did something small but grown-up: I set a hard removal time and tracked when symptoms started. That one change didn’t fix everything. But it stopped me from treating my cornea like a disposable part. And weirdly, it made every other treatment easier to evaluate.
FAQ
Can I use Miebo while wearing contact lenses?
Follow the official labeling and your prescriber. The FDA labeling includes instructions for contact lens wear (removing lenses before administration and waiting before reinsertion). If your clinician gave you different instructions for your specific situation, follow them.
How long does it take to notice improvement with Miebo?
Some people notice changes in comfort timing (burn starts later) before they notice dramatic changes in symptom intensity. Track a single metric for 7 days to avoid guessing; then discuss the trend with your clinician.
Does Miebo work for evaporative dry eye from MGD?
Miebo is designed to reduce tear evaporation, which is a key mechanism in evaporative dry eye and often overlaps with MGD. Whether you feel meaningful improvement depends on your gland function, environment, lens wear habits, and whether other drivers (allergy, fit, solution) are also present.
Why do my eyes burn more at the end of the day with contacts?
Late-day burning often reflects accumulated tear film stress: evaporation, reduced blinking during screen time, airflow exposure, and the added friction of contact lens wear. The “when it starts” clue can help narrow the likely driver.
Is end-of-day burning more likely dry eye or allergies?
Dry eye often presents as burning/gritty sensation and fluctuating vision; allergy often brings itch and seasonal patterns. Overlap is common. If you have significant itch, swelling, or clear seasonal triggers, ask your clinician whether an allergy branch should be part of your plan.
Can I combine Miebo with preservative-free artificial tears?
Many people use multiple therapies, but spacing and sequencing should follow clinician guidance. If you’re combining products, ask your prescriber for an exact spacing plan so you don’t sabotage comfort or your trial results.
What should I track to know if Miebo is helping?
Pick one: “burning at 6 p.m.” (0–10) or “hours until discomfort starts.” Keep lens brand/solution stable for 7 days. Bring the log to your follow-up.
What if Miebo stings or makes my eyes feel worse?
Brief awareness can happen with new drops, but persistent burning, increasing redness, discharge, or vision changes deserve a call to your clinician—especially for contact lens wearers. When in doubt, remove lenses and get evaluated.
When to seek help (same-day vs soon)
This is the “protect your future eyes” section. A good rule: discomfort is common; pain plus red flags is not.
Seek same-day urgent care if you have:
- Severe eye pain or pain that escalates rapidly
- Light sensitivity (photophobia)
- Sudden vision change
- Significant redness with discharge
- Trauma or suspected foreign body
Book soon (this week) if:
- End-of-day burning persists despite reduced wear time and stable lens hygiene
- Frequent contact lens intolerance episodes
- Symptoms fluctuate wildly with screens/HVAC and don’t respond to basic changes
Money Block: Quote-prep list (what to bring to your visit)
- Your 7-day symptom log (time of onset + score)
- Lens brand, replacement schedule, and solution name
- Any allergy meds (oral or eye drops)
- Where you work (screens/HVAC) and typical wear hours
Next step: Put this list in your phone notes so you don’t rely on memory in the exam chair.
Next step: one concrete action
Here’s your 15-minute plan. It’s not dramatic. It’s effective.
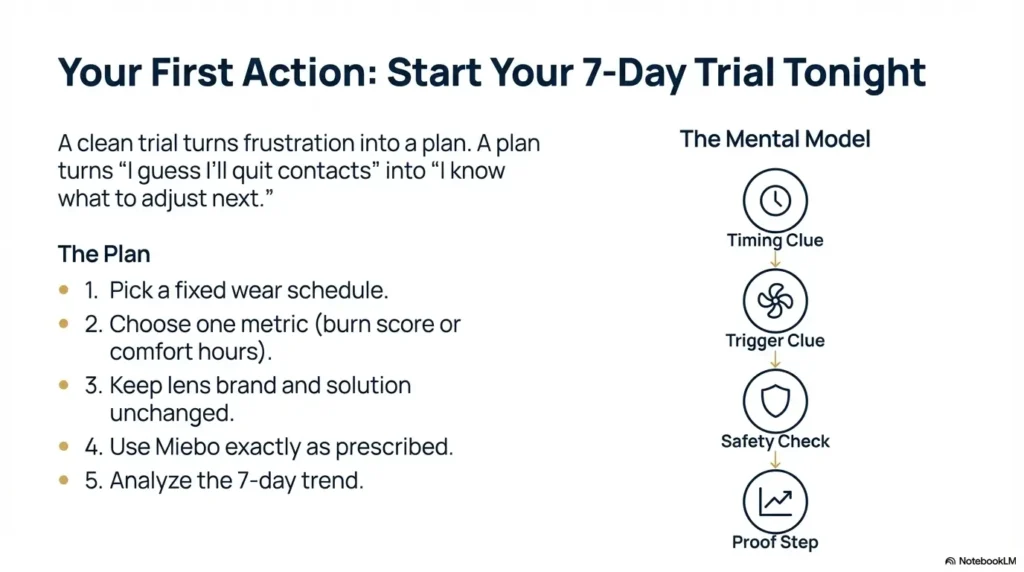
Do the 7-day “End-of-Day Burn Trial” tonight
- Pick a fixed wear schedule (insert at X a.m., remove at X p.m.).
- Choose one metric: burning at 6 p.m. (0–10) or hours until discomfort.
- Keep lens brand and solution unchanged for 7 days.
- Use Miebo exactly as prescribed by your clinician.
- Bring the trend (not just feelings) to your follow-up.
- One metric
- Stable variables
- Honest red-flag thresholds
Apply in 60 seconds: Set a daily alarm: “Log burn score.”
Close the loop: a honest conclusion
So—does Miebo reduce end-of-day burning in contact lens wearers with MGD evaporative dry eye? The honest answer is: it can, when evaporation is the dominant driver and the rest of your lens ecosystem isn’t quietly sabotaging you. Your win might not look like “perfect eyes.” It might look like two more comfortable hours, fewer rescue drops, and a night that doesn’t end with you staring into the bathroom mirror bargaining with your tear film.
If you want one reliable truth to leave with, it’s this: measure the thing you care about. A 7-day log turns frustration into a plan, and a plan turns “I guess I’ll quit contacts” into “I know what to adjust next.”
Timing clue
Burning worst at 3–8 p.m.?
→ Likely evaporation lane
Trigger clue
Worse with HVAC/screens/wind?
→ Strengthens MGD suspicion
Safety check
Pain + light sensitivity/discharge?
→ Same-day evaluation
Proof step
Run 7-day burn log with stable variables
→ Decide: continue / adjust / escalate
Use this: If you can’t place yourself in a box, that’s your cue to get an exam rather than guessing.
For general education on dry eye and symptoms, the American Academy of Ophthalmology is a solid starting point. For an easy overview of how doctors test tear film stability (including tear breakup time), the National Eye Institute explains it in plain language.
Last reviewed: 2025-12.