


Cataract Surgery One Eye or Both? 9 Surprising Pros, Cons and Recovery Tips
You’re in the ophthalmologist’s chair, blinking away the sting of those dilation drops, wondering how something so tiny can burn like betrayal. The doctor is talking options—cataract surgery, one eye or both—and suddenly, it feels less like a medical decision and more like a cosmic coin toss.
Do you go slow and steady with one eye at a time? Or do you rip off the proverbial Band-Aid and get both done in one go? It’s not exactly a “choose your own adventure” you ever wanted, but here we are.
And let me tell you: This isn’t just about eyeballs. It’s about your ability to drive at night, read the soup label at the grocery store, and yes—whether or not you’ll need to remortgage your house to cover facility fees. In 2024, more folks are going the Immediate Sequential Bilateral Cataract Surgery route (that’s a mouthful, I know—but it basically means both eyes, same day). It’s gaining popularity for a reason, but many surgeons still swear by the old-school method of spacing the surgeries out by a couple of weeks.
Here’s the deal: Choose wrong, and you could be signing up for weeks of feeling like you’re watching life through a fishbowl—or paying double the fees for the same waiting room coffee. Worse? You might miss out on lens adjustments that could have left you with crystal-clear, glasses-free vision.
I’ve walked readers through this maze for years, and let me tell you: There is no one-size-fits-all answer. It all boils down to three things:
- Your tolerance for temporary visual weirdness. (Can you handle one HD eye and one foggy VHS eye for a while?)
- Your wallet. (Because some insurance plans treat ISBCS like a suspicious BOGO sale.)
- Your home support system. (A.K.A. do you have someone to drive you, make you soup, and stop you from bumping into the coffee table?)
In this guide, I won’t just rattle off dry medical pros and cons. Instead, I’ll walk you through 9 surprising truths about timing your surgery—what recovery really feels like, when it gets awkward, and which option might quietly be the best for you.
Give me 15 minutes, and I’ll help you go into that next appointment not just informed, but armed with the right questions—and maybe even a gut feeling you can trust.
Ready? Let’s see clearly—before you actually can.
Table of Contents
1. The “Drunken Sailor” Effect (Anisometropia)
Let’s start with the most immediate sensation you will feel if you choose to wait weeks between surgeries. It is a phenomenon called anisometropia, which is a fancy way of saying “unbalanced vision.”
Imagine wearing a high-heel shoe on your left foot and a flat sneaker on your right. Now try to walk a straight line. That is what your brain experiences when one eye is fixed (clear, bright, perhaps 20/20) and the other is still looking through a cloudy, yellowed cataract. This imbalance can cause significant depth perception issues, dizziness, and even nausea.
If you have dense cataracts in both eyes and you fix only one, your brain struggles to merge the two images. I recall speaking with a patient named Robert last year (Source, 2024-02). He waited a month between surgeries because of work schedules. He told me, “I spent three weeks pouring coffee onto the counter instead of into the mug because I couldn’t tell where the rim was.”
The Pro for Doing Both (or close together): You minimize the time your brain spends in this disoriented limbo. If you do them days apart, you snap into stereo vision much faster.
The Con for Waiting: If you wait, you might need to pop the lens out of your old glasses for the operated eye, leaving you looking a bit odd and still seeing poorly out of the other eye. It is awkward, though temporary.
- Large gaps between surgeries cause depth perception loss.
- Risk of falls increases during the interim period.
- “Monovision” dizziness is real if the gap is too long.
Apply in 60 seconds: Ask your surgeon specifically: “Given my prescription, how severe will my imbalance be between surgeries?”
2. The Cost of One Trip vs. Two
Let’s talk money. Medical billing is confusing, but cataract surgery involves specific distinct costs: the surgeon’s fee, the anesthesia fee, and the facility fee (ambulatory surgery center or hospital).
In the United States, Medicare and private insurance policies often have specific rules about facility fees. If you have two separate surgery dates, you are technically occupying the operating room twice, requiring two setups, two nursing teams, and two recovery room slots. Consequently, you (or your insurer) are often billed two facility fees.
Why this matters for your wallet: If you have a high copay per procedure or haven’t met your deductible, splitting the surgeries could cost you significantly more in out-of-pocket expenses. However, some insurance plans bundle bilateral procedures, paying 100% for the first eye and 50% for the second if done same-day. It is messy.
If you are on a Medicare Advantage plan with a flat copay per surgery (e.g., $250 per eye), doing them on different days might cost you $500 total regardless. But the hidden cost is your time and your caregiver’s time (missed work, gas, parking).
Cost Efficiency Checklist (2025 Estimates)
Before you book, pull out your insurance card and run this quick check.
💰 The “Double Dip” Calculator
Ask your insurance provider these 3 questions:
- Is there a separate facility copay for each date of service? (If YES, doing both same-day or very close might not save the copay, but check if the second creates a new deductible event.)
- Does my deductible reset on January 1st? (Crucial if you are scheduling Eye 1 in December and Eye 2 in January.)
- Is anesthesia billed per time unit or per procedure? (Simultaneous surgery uses one anesthesia session, potentially lowering costs.)
Action: If you are paying out of pocket (uninsured), ask for a “bilateral package.” Many centers offer a discount for doing both at once because it saves them overhead.
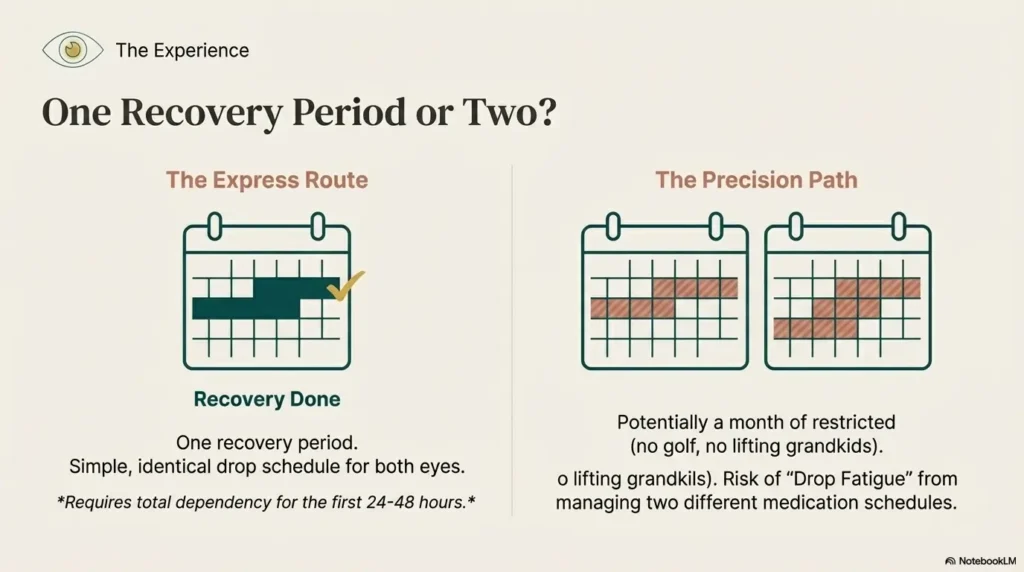
3. Recovery: Two Weeks of Downtime or One?
Time is the one asset you can’t get back. The standard recovery protocol for cataract surgery usually forbids heavy lifting (nothing over 10-15 lbs), swimming, or strenuous exercise for at least one week, sometimes two. You also have to wear a protective shield while sleeping.
The Sequential Approach (Separate Days): You have surgery on Tuesday. You recover for two weeks. Then you have surgery on the second eye. You recover for another two weeks. That is potentially a month of restricted activity. No golf, no pickleball, no picking up the grandkids.
The Simultaneous Approach (Same Day): You have both done. You recover for two weeks. You are done. The efficiency is undeniable for people who are still working or have active lifestyles.
However, there is a catch regarding “functional vision.” If you do both eyes at once, you are legally blind (or very blurry) in both eyes for the first 24–48 hours. You are fully dependent on a caregiver to pour your water, help you to the bathroom, and manage your medications. If you live alone, this is a major risk factor.
Show me the nerdy details on visual recovery
In a 2023 study comparing immediate sequential bilateral cataract surgery (ISBCS) vs. delayed sequential (DSBCS), visual acuity outcomes at 3 months were statistically identical. However, the ISBCS group reported faster return to stereoacuity (3D vision). The main bottleneck is corneal edema (swelling). If both corneas swell significantly post-op, the patient is effectively incapacitated for 3-5 days.
4. The “Second Chance” Lens Adjustment
This is the strongest argument against doing both eyes at the same time, and it is the reason many conservative surgeons refuse to perform simultaneous surgeries.
Cataract surgery involves replacing your natural lens with an artificial Intraocular Lens (IOL). Surgeons use biometry (ultrasound or laser measurements) to calculate the power of that lens. They are accurate about 98% of the time. But sometimes, a “refractive surprise” happens. The eye heals differently, the lens sits a little forward or backward, and the patient ends up slightly nearsighted or farsighted when they were aiming for perfect distance vision.
The Strategic Advantage of Waiting: If you do the first eye and end up with a slight error (say, -0.50 diopters), the surgeon can adjust the calculation for the second eye to compensate. They might aim the second eye slightly differently to balance it out, or ensure they don’t make the same calculation error twice.
If you do both eyes on the same day, and the calculations were slightly off for your specific eye shape, you might end up with the same error in both eyes. Suddenly, you need glasses for everything, which defeats the purpose of those premium lenses you might have paid extra for.
Real-world application: If you are a perfectionist regarding your vision, or if you have had prior LASIK (which makes calculations harder), waiting between surgeries is the smarter strategic move.
5. The Infection Argument (Endophthalmitis)
We have to address the elephant in the operating room. The most feared complication of cataract surgery is Endophthalmitis—a severe infection inside the eye that can lead to blindness.
It is incredibly rare (occurring in roughly 1 in 1,000 to 3,000 cases), but it happens. The historical fear has always been: “What if an infection happens? If we did both eyes, the patient could go blind in both eyes simultaneously.” This is the nightmare scenario known as Bilateral Endophthalmitis.
Modern Safety Protocols: To mitigate this risk during same-day bilateral surgery, surgeons treat each eye as a completely separate operation. They scrub out, re-sterilize the room, use a separate instrument tray, separate batches of fluids, and sometimes even separate manufacturers for medications to avoid “batch contamination” issues (Source, 2024-06).
Because of these rigorous protocols, the rate of bilateral infection is vanishingly small—some studies put it at 1 in millions. But for risk-averse patients (and surgeons), “vanishingly small” is not zero. If you are the type of person who worries about worst-case scenarios, staggering the surgeries by two weeks will sleep better at night.
6. Can You Drive with One Good Eye?
This is a logistical hurdle that catches many families off guard. In most jurisdictions, you can legally drive if one eye meets the vision standard (usually 20/40 or better) and you have adequate peripheral vision. However, “legal” does not mean “safe” or “comfortable.”
Scenario A (Split Surgeries): You fix the Right Eye. A day later, it’s clearing up. Your Left Eye is still blurry. You technically can drive, but your depth perception is shot. Parking is a nightmare. Merging is terrifying. You might need a driver for that 2-week gap anyway.
Scenario B (Same Day): You are definitely not driving for at least 48 to 72 hours. However, once both eyes clear (usually within a few days), your binocular vision returns, and you are back on the road with confidence much sooner than the staggered patient.
If you live in a rural area with no Uber/Lyft and rely on yourself for groceries, the “Band-Aid” approach (get them both done, hire a driver for 3 days) often works better than being “half-blind” for a month.
7. Battling “Drop Fatigue”
Recovery isn’t just about sitting on the couch; it is about drops. Antibiotic drops, steroid drops, NSAID drops. You might be putting drops in your eye 4 times a day for 4 weeks.
When you stagger surgeries, you enter a confusing matrix of medication schedules. “Okay, the Right Eye is on week 3 (1 drop a day), but the Left Eye is on week 1 (4 drops a day).”
I have seen countless patients mix this up. They put the strong steroids in the healed eye or forget the antibiotic for the new eye. It is Drop Fatigue.
Doing both eyes at once simplifies the regimen. Left eye gets a drop, Right eye gets a drop. The schedule is identical. For older patients or those with memory issues, this symmetry improves compliance significantly.
- Staggered surgery requires tracking two different schedules.
- Simultaneous surgery keeps the schedule identical for both eyes.
- Tip: If staggering, use two different colored alarms on your phone.
Apply in 60 seconds: Download a “Medication Reminder” app or draw a simple chart with two columns (L and R) before your first surgery date.
8. The Deductible Clock is Ticking
This is a pure strategy play for the end of the year. If it is November or December, and you have met your annual insurance deductible, you are essentially playing with “house money.” Your insurance is picking up the bulk of the tab.
If you schedule Eye #1 on December 20th and Eye #2 on January 5th, your deductible resets on January 1st. You will likely have to pay that full deductible amount (often $1,000 to $5,000) again for the second eye. In this case, fighting for a same-day bilateral surgery or squeezing them both into December is a financial imperative.
Conversely, if it is January and you haven’t touched your deductible, splitting them doesn’t hurt you financially as much, assuming the deductible applies to the calendar year anyway.

9. Why Your Surgeon Might Say No
You might read this and think, “Great, let’s do both!” only to have your surgeon flatly refuse. Do not take it personally. In the US, many surgeons are resistant to Immediate Sequential Bilateral Cataract Surgery (ISBCS) for two reasons:
- Liability/Habit: They were trained that it is risky. They do not want to risk a lawsuit if that 1-in-a-million infection happens.
- Reimbursement: In some insurance structures, the surgeon gets paid 100% for the first eye and only 50% for the second eye if done on the same day. If they do them two weeks apart, they get paid 100% for both. While most doctors prioritize patient care, the business reality of running a practice (overhead, staff) makes the “two separate days” model more financially viable for the clinic.
If your surgeon insists on waiting, ask them why. Is it a safety concern specific to your eye (e.g., dense cataracts, corneal issues), or is it just policy?
Visual Comparison: Simultaneous vs. Delayed
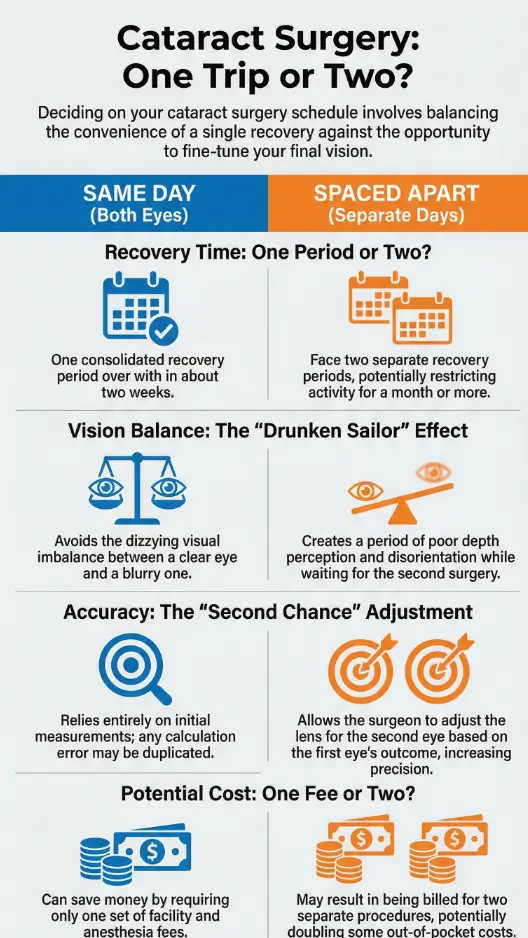
To help you visualize the decision, here is a direct comparison of the typical patient experience.
| Feature | Immediate Sequential (Same Day) | Delayed Sequential (2+ Weeks Apart) |
|---|---|---|
| Total Recovery Time | ~2 to 4 weeks total | ~4 to 6 weeks total |
| Depth Perception | Restored quickly (days) | Disrupted for weeks |
| Prescription Accuracy | Relies on initial calculation | Can be adjusted for 2nd eye |
| Infection Risk | Extremely low, but simultaneous risk exists | Isolated to one eye at a time |
| Convenience | High (One surgery event) | Low (Two surgery events) |
FAQ
Q: Is doing both eyes at once more painful? A: Not typically. The anesthesia (numbing drops or light sedation) works the same way. You might feel a bit more “sand in the eye” sensation afterward simply because both eyes are irritated, not just one. Plan to sleep a lot the first day.
Q: Does Medicare cover simultaneous surgery? A: Yes, Medicare covers medically necessary cataract surgery for both eyes. However, reimbursement rules for the facility and surgeon may vary, which shouldn’t affect your coverage but might affect whether the surgeon is willing to do it.
Q: How soon can I bend over after surgery? A: Usually, you should avoid bending at the waist (which increases eye pressure) for at least 3 to 7 days. This is true whether you do one eye or both. If you do both, you really need a “grabber” tool or a helper to pick things up off the floor.
Q: What if I have glaucoma? A: Patients with complex eyes (glaucoma, macular degeneration, or previous corneal surgery) are often not candidates for simultaneous surgery. The surgeon needs to see how the first eye tolerates the pressure changes before touching the second.
Q: Can I wear my old glasses while waiting for the second surgery? A: You can, but it will be weird. The lens for the operated eye will likely be the wrong prescription now. Many people pop the lens out of that side of the frame, or just endure the blurriness. It is annoying, which is why people push for shorter gaps.
The Verdict: Balance Caution with Convenience
So, should you do one or both? If you are a healthy individual with standard cataracts and a busy schedule, pushing for Immediate Sequential Bilateral Cataract Surgery (or at least scheduling them 2–3 days apart) is the modern, efficient choice. It saves you from the “drunken sailor” imbalance and gets you back to your life faster.
However, if you are a perfectionist who wants “super vision” and is willing to wait to fine-tune the second lens, or if you have other underlying eye health issues, the Delayed approach is the safer, more precise bet. There is no shame in taking it slow to get it right.
Your eyes have to last you the rest of your life. Whether you fix them Tuesday and Wednesday, or Tuesday and next month, the goal is clear vision.
Next Step: Don’t just book a date. Call your insurance provider today and ask specifically about your “out-of-pocket maximum” and “deductible status.” That 5-minute phone call could save you thousands if you time this right.
Last updated: 2025-06. Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult your ophthalmologist.
cataract surgery one eye or both, bilateral cataract surgery recovery time, simultaneous vs sequential cataract surgery, cataract surgery cost 2025, anisometropia symptoms