
Navigating the Unseen: A Guide to Charles Bonnet Syndrome
“The room can be completely familiar… and still your vision may suddenly add something that is not there.”
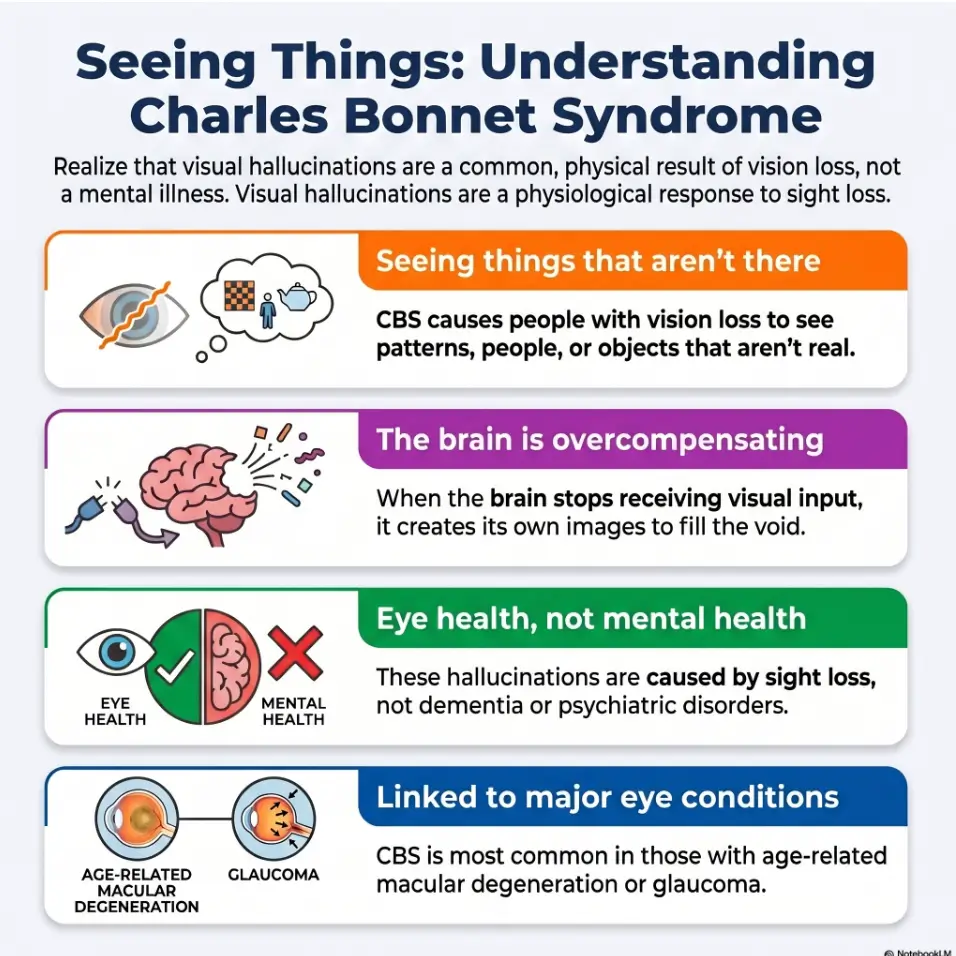
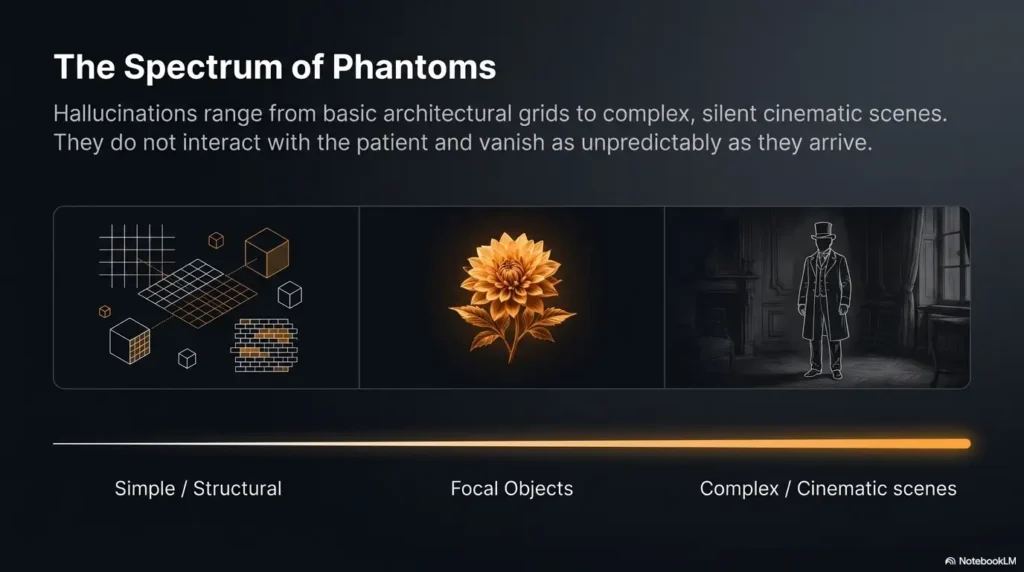
Charles Bonnet syndrome (CBS) is a vision-related condition where significant vision loss triggers visual hallucinations—patterns, faces, or animals that aren’t physically there. While many realize these images aren’t real, the experience can feel startling and deeply isolating.
The true burden is often the silence: the fear that speaking up might cost you your independence or the trust of those around you.
This guide is designed to help you differentiate between the symptoms of vision loss and red flags that require urgent medical care. We focus on practical patterns to help you:
- • Respond safely to visual disturbances.
- • Adjust lighting and home routines for comfort.
- • Support loved ones without panic.
- • Identify when to seek prompt clinical attention.
Table of Contents
Fast Answer
Charles Bonnet syndrome can cause people with significant vision loss to see patterns, faces, figures, animals, objects, or scenes that are not really there. It is usually visual only, and many people know the images are not real. Coping starts with reassurance, safer lighting, vision care follow-up, a symptom log, and knowing when symptoms need urgent medical help.
The most important first step is not to panic and not to hide it. New visual hallucinations should be discussed with an eye doctor or another qualified clinician, especially if the symptoms are sudden, changing, frightening, or connected with confusion, weakness, headache, fever, medication changes, a fall, or other body-wide symptoms.
- Notice whether the experience is visual only.
- Write down when and where it happens.
- Tell one trusted person and one clinician.
Apply in 60 seconds: Write one sentence: “I sometimes see ______, usually when ______.” Bring that sentence to your next appointment.
Safety / Disclaimer: Visual Hallucinations Deserve Calm, Not Guesswork
Visual hallucinations deserve a steady response. Not a dramatic one. Not a dismissive one. And definitely not the family-group-chat version where everyone becomes a neurologist before lunch.
This guide is educational. It can help you organize symptoms, understand common coping steps, prepare for a medical conversation, and make the home safer. It should not replace evaluation by an eye doctor, primary care clinician, neurologist, psychiatrist, emergency clinician, pharmacist, occupational therapist, or other licensed professional when symptoms raise concern.
Use This Guide for Coping, Not Self-Diagnosis
Charles Bonnet syndrome is associated with visual hallucinations in people with vision loss. That sounds simple on paper, but real life is rarely written in tidy clinic language. A person may have macular degeneration and also be taking several medications. A person may have glaucoma and also be sleep deprived. A person may have diabetic eye disease and also be fighting an infection. Several things can stand in the same hallway wearing similar coats.
That is why a clinician should help rule out other causes, especially when hallucinations are new, changing, frightening, or paired with confusion, weakness, headache, fever, fainting, medication changes, recent surgery, or a fall. The American Academy of Ophthalmology describes Charles Bonnet syndrome as visual hallucinations related to vision loss, but medical evaluation still matters because not every hallucination after vision loss is automatically CBS.
The Key Safety Line: Vision Only
One practical safety line is this: many descriptions of Charles Bonnet syndrome emphasize that the experience is visual. The person may see patterns, faces, people, animals, buildings, flowers, insects, children, landscapes, grids, lights, or moving scenes. Many people know that the images are not real, even if the images look vivid.
If the person is also hearing voices, smelling things that are not present, feeling touched, becoming confused, losing track of where they are, acting on commands, or becoming convinced that the images are physically real, do not file it away as “just CBS.” That does not mean disaster. It does mean the situation needs a more careful medical review.
When to Seek Help
Contact an eye doctor, primary care clinician, or urgent medical service if hallucinations begin suddenly, come with neurological symptoms, follow a fall or head injury, appear after a medication change, include non-visual sensations, or make the person unsafe at home or while driving.
Urgent symptoms include one-sided weakness, facial drooping, slurred speech, severe headache, seizure-like activity, fever, fainting, chest pain, sudden confusion, sudden vision change, or a recent head injury. In those cases, the goal is not to debate labels. The goal is to get the person assessed.
- Visual-only symptoms may fit CBS, especially with known vision loss.
- Confusion, weakness, fever, fainting, or speech changes need prompt help.
- Medication changes should be reviewed instead of guessed around.
Apply in 60 seconds: Put “visual only?” at the top of your symptom note. It is a small question with big safety value.
Start Here: The Brain Fills in the Quiet Places
When vision fades, the world does not simply become dimmer. It can become less complete. Edges blur. Faces lose detail. Shadows become suspicious. The wallpaper, once obedient, starts keeping secrets. In that quiet, the visual brain may begin generating images of its own.
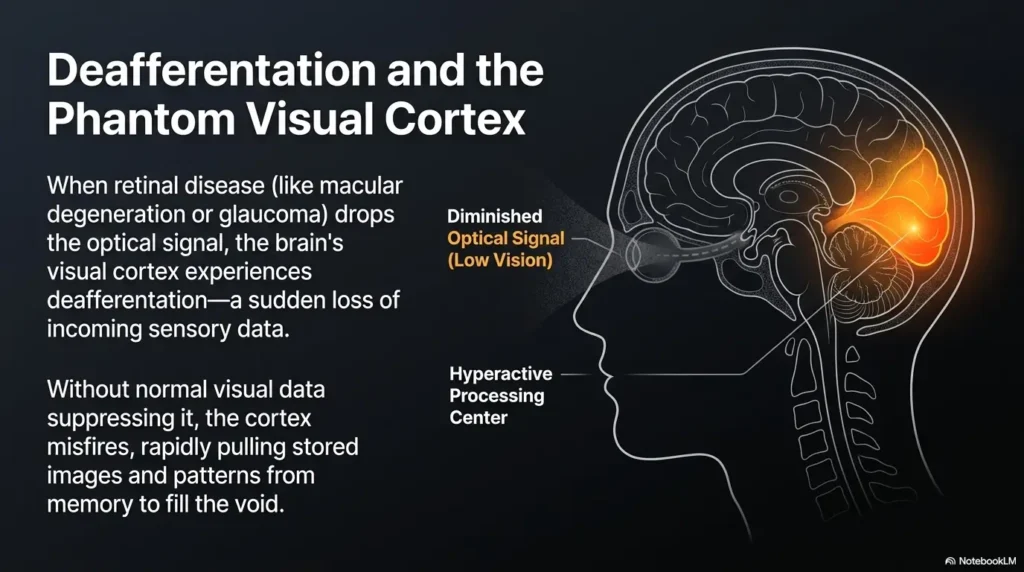
This is one common way to explain Charles Bonnet syndrome: when the eyes send less information, the visual parts of the brain may produce images without an outside object causing them. Clinicians sometimes call this a visual release phenomenon. The phrase sounds like a tiny orchestra being let out of a locked room. Not inaccurate, really.
Charles Bonnet Syndrome Is Not “Going Crazy”
For many people, the first fear is not the image itself. It is what the image might mean. “Am I losing my mind?” “Will my family trust me?” “Will the doctor think I am confused?” “Will someone take away my independence?”
Those fears are understandable. Visual hallucinations are startling because they seem to violate the basic contract of daily life: I open my eyes, and the world reports back. But in Charles Bonnet syndrome, the issue is often not moral weakness, imagination, attention-seeking, spiritual failure, or “going crazy.” It is a known phenomenon associated with reduced visual input.
I have watched families relax when someone finally says, “This can happen with vision loss.” The room changes. Shoulders come down. The person stops performing normality and starts describing reality. That shift matters because shame wastes energy that could be used for safer routines.
Why Patterns, Faces, and Scenes Can Appear
Some people see simple visual effects: lines, dots, grids, tiles, geometric shapes, lace-like patterns, shimmering colors, or repeated designs. Others see formed images: people sitting in a chair, children playing, animals moving across the floor, flowers on the wall, insects, vehicles, buildings, or full scenes.
The images may last seconds, minutes, or longer. They may appear in dim light, bright glare, quiet rooms, familiar rooms, or moments of fatigue. Some people find them merely odd. Others find them deeply distressing, especially at first. The content can be ordinary, beautiful, strange, annoying, or frightening. The emotional reaction can change day by day.
The key is not to judge the person by what appears. A person is not responsible for the content of an involuntary visual hallucination. That sentence may seem obvious, but for a frightened reader, it can be a rope across a river.
What Makes This Topic So Hard to Talk About
Many people stay silent because they fear being dismissed, labeled, or treated as less capable. Older adults may worry that one honest sentence will be used against them: no more driving, no more living alone, no more privacy, no more ordinary trust. Caregivers may also panic because they do not know the difference between visual hallucinations linked with vision loss and symptoms that suggest delirium, dementia, medication problems, or neurological illness.
So everyone freezes. The person seeing things says nothing. The family notices unease but avoids asking. The doctor visit focuses on eye pressure, injections, lenses, drops, or scan results. The strange images remain backstage, rearranging the furniture.
This guide takes the opposite approach: name the symptom plainly, respond without drama, protect dignity, and build a small safety system around real life.
Show me the nerdy details
Charles Bonnet syndrome is often explained as a mismatch between reduced visual input and continued activity in visual processing areas of the brain. The person is not choosing the images. The experience can be vivid because the brain is not merely showing “weak imagination”; it is generating visual content through pathways normally involved in perception. That is why reassurance alone may help fear, but it may not immediately stop the images.
Who This Is For, and Who It Is Not For
This guide is for the person who sees something, knows something is strange, and is trying to decide whether to whisper it or bury it. It is also for the daughter, son, spouse, friend, neighbor, aide, or grandchild who wants to help without becoming a household detective with a clipboard and a worried forehead.
This Is For People With Vision Loss Who See Things Others Do Not
This article may help if you have macular degeneration, glaucoma, diabetic retinopathy, cataract-related visual changes, retinal disease, optic nerve disease, or low vision from another cause, and you are seeing visual images that other people do not see.
Maybe you see patterns on blank walls. Maybe people appear at the edge of the room. Maybe animals, flowers, faces, or unfamiliar figures show up when you are tired. Maybe it happens at night, during television, after waking, while sitting quietly, or while moving through a familiar hallway. Maybe it happened once and now you are waiting for it to happen again, which is a special little torture invented by the anxious brain.
This guide can help you form language around the experience. It can also help you decide what to track, what to change at home, what to ask your eye doctor, and what symptoms should not be ignored.
This Is Also for Caregivers Who Need Better Words
If someone you love says they see something you do not see, your first words matter. “There is nothing there” may be factually true from your perspective, but it can land like a door closing. A better beginning is, “I believe you are seeing that. I do not see it, but I want to make sure you feel safe.”
That sentence does two things at once. It validates the person’s experience without confirming that the image is physically present. It also moves the conversation toward safety instead of argument.
Caregivers do not need to become experts overnight. They need a few useful questions: Is it visual only? Do you know it is not real? Is it blocking your path? Did it start suddenly? Are you confused, weak, feverish, dizzy, or recently injured? Did any medication change? Has your vision worsened?
This Is Not for Ignoring Red Flags
This guide is not a permission slip to avoid care. It is not a replacement for an eye exam, primary care visit, medication review, neurological assessment, mental health care, emergency evaluation, or occupational therapy advice when those are needed.
It is also not meant to diagnose someone from a kitchen table conversation. Families sometimes want a quick answer because uncertainty is uncomfortable. But the safest answer is often layered: “This may fit Charles Bonnet syndrome, and we still need to rule out other causes.” That is not indecision. That is good risk management with its shoes tied.
- Patients need language that does not shame them.
- Caregivers need questions that do not interrogate.
- Clinicians need clear details, not polished speeches.
Apply in 60 seconds: Replace “Are you hallucinating again?” with “Have the images been showing up more often this week?”
The First Conversation: What to Tell Your Eye Doctor
The first conversation does not need to be elegant. It only needs to be honest enough to open the right door. You do not need a poetic description of the figure near the hallway. You do not need to know whether it was a hallucination, illusion, floater, shadow, migraine aura, medication effect, sleep-related image, or something else. That is precisely why the appointment exists.
You need to bring the raw material: what you saw, when it happened, how long it lasted, what else was happening in your body, and whether you knew it was not real.
Bring the Details, Not Just the Label
It is tempting to walk into the appointment and say, “I think I have Charles Bonnet syndrome.” That can be useful, but the details matter more than the label. A clinician can work better with a pattern than with a conclusion.
Try to document:
- What the images look like: patterns, faces, people, animals, objects, lights, scenes, or movement.
- When they happen: morning, evening, night, after waking, during quiet sitting, while walking, or while watching television.
- How long they last: seconds, minutes, longer stretches, or repeated episodes.
- Whether you know they are not real while they are happening.
- Lighting conditions: dim room, glare, shadows, bright window, nighttime route, bathroom mirror, or screen use.
- Recent changes: vision changes, new glasses, surgery, injections, new medications, dosage changes, illness, sleep loss, stress, or a fall.
- Impact on function: walking, bathing, cooking, driving, sleeping, reading, mood, or anxiety.
This is not about creating a perfect diary. A two-minute note can be enough. Doctors are used to imperfect information. Frankly, most of medicine runs on people trying to remember Tuesday while sitting on crinkly paper under fluorescent lights.
Say the Embarrassing Part Plainly
Many people soften the symptom because they are embarrassed. They say, “My eyes are playing tricks,” or “I see shadows,” or “Sometimes the room looks funny.” Those phrases are understandable, but they may not be specific enough.
Here is a simple script:
“Since my vision changed, I sometimes see patterns or figures that I know are not real. Could this be Charles Bonnet syndrome, and what else should we rule out?”
That sentence is strong because it gives the clinician four useful pieces of information: vision changed, visual images occur, insight is present, and the patient wants other causes considered. It is not dramatic. It is not self-diagnosing. It is clean, like a well-labeled drawer.
Ask About Low Vision Support, Not Only Eye Disease
Many eye visits focus on disease monitoring: scans, pressures, injections, drops, surgery options, progression, and follow-up schedules. Those things matter. But a person living with low vision also needs help with the daily environment. The question is not only, “What is happening to my eye?” It is also, “How do I live more safely with the vision I have now?”
Ask about low vision rehabilitation, magnification, contrast, task lighting, glare control, mobility training, occupational therapy, home safety, and whether any local vision services or nonprofit resources are available. The National Eye Institute explains that low vision care may include devices, training, and strategies to help people use remaining vision more effectively.
Quote-Prep List: What to Gather Before Comparing Low Vision Services
If you are looking into low vision services, occupational therapy, home safety support, or assistive devices, gather the basics before you compare options. This prevents the classic “buy first, understand later” routine, which has emptied many drawers and wallets.
- Your main diagnosis or reason for vision loss, if known.
- Current glasses, magnifiers, lighting tools, and devices used.
- The 3 hardest tasks: reading mail, cooking, bathing, stairs, phone use, medication labels, or driving decisions.
- Where hallucinations show up most often, especially if they affect walking or night routines.
- Insurance questions, referral requirements, and transportation limits.
Neutral action line: Before buying another device, ask whether the service can evaluate your actual home tasks, not just your eye chart.
Coping Starts Small: Change the Scene Before You Fight the Image
The first instinct may be to fight the image. Stare at it. Prove it wrong. Argue with it internally. Call someone into the room to confirm that reality is still under management. All of that is human. It is also exhausting.
A more useful first approach is to change the scene. Think of it less as wrestling a ghost and more as adjusting the room’s volume. The image may not vanish every time, but you can often reduce fear, interrupt the moment, and regain control of the next action.
Adjust Light Like a Dimmer, Not a Weapon
Some people find that changing lighting helps. If the room is dark, turn on a light. If glare is sharp, soften it. If a bright window is creating confusing contrast, shift your chair. If a hallway feels visually noisy at night, add consistent low-level lighting. For some homes, choosing between a red vs amber night light for low vision can make nighttime orientation feel less harsh while still keeping the path readable. The point is not to blast the image into submission with a lamp. This is not a courtroom interrogation of the wallpaper.
Instead, use light as a cue to the brain and body: the environment has changed; we are safe enough to re-orient. For low vision, consistent lighting is often more useful than dramatic lighting. Sudden glare can be as confusing as darkness, especially when a motion sensor light feels too bright and turns a quiet hallway into a tiny stadium.
Blink, Look Away, Move, Re-Anchor
Simple interruption techniques may help some people. Try blinking slowly, closing and opening the eyes, looking toward another object, turning your head, changing seats, standing up if safe, or moving into another room. Some people find that reaching for a familiar object, such as a textured blanket, armrest, table edge, or cane, helps re-anchor attention.
Do not treat these techniques as guaranteed cures. Treat them as experiments. One person may find that bright light helps. Another may need dimmer light. One may prefer music. Another may need quiet. The useful question is not, “What works for everyone?” It is, “What reliably lowers fear and improves safety for me?”
Here’s What No One Tells You: Boredom Can Be a Trigger
Quiet, passive moments can make visual hallucinations more noticeable for some people. A person may sit alone after dinner, with low light, little conversation, and tired eyes. The brain, never one to waste an empty stage, begins producing visual theater.
That does not mean people should stay busy every second. Rest matters. But it may help to build a low vision activity menu for vulnerable times:
- Audio books or familiar radio programs.
- Phone calls with a trusted person.
- Tactile hobbies, such as folding towels, sorting safe household items, knitting, or simple handwork.
- Guided music, prayer, meditation, or breathing exercises.
- Short, safe walks in a familiar route when appropriate.
I once heard a caregiver describe her mother’s evening routine as “the haunted hour.” Not because anything supernatural was happening, but because loneliness, dim light, and fatigue always seemed to meet at 7:30 p.m. They did not cure the hallucinations overnight. They changed the hour: brighter lamp, cup of tea with a lid, favorite radio show, phone nearby, walking path cleared. The room became less theatrical.
Mini Calculator: Your “Vulnerable Moment” Score
Use this quick check to identify when an episode may be more likely to feel frightening or unsafe. Count 1 point for each “yes.”
- Is the room dim, glaring, or full of shadows?
- Are you tired, lonely, stressed, or recently awakened?
- Are you walking, bathing, cooking, using stairs, or moving at night?
Score: 0 means lower concern for that moment. 1 means adjust the environment. 2 or 3 means pause and make safety the priority before continuing.
Neutral action line: If your score is 2 or higher, change light, sit down if needed, and delay the task until you feel steadier.
- Adjust lighting gently.
- Re-anchor with a familiar object or task.
- Build safer routines around predictable trigger times.
Apply in 60 seconds: Choose one “vulnerable hour” and add one steady cue: light, sound, phone call, or safe activity.
Don’t Do This: The Mistakes That Make Fear Louder
Fear has a way of hiring bad advisors. It tells people to hide symptoms, argue with the image, test themselves repeatedly, or let family members overcorrect every sentence. The result is usually more anxiety, not more safety.
Mistake 1: Hiding It Until Anxiety Takes Over
Silence can turn a visual symptom into a private courtroom. The person becomes the judge, defendant, witness, and exhausted jury. Every new image becomes evidence. Every quiet evening becomes a test. Every doctor visit becomes a missed chance.
Telling one trusted person can reduce the burden. Telling one clinician can create a care pathway. The conversation may feel embarrassing for 30 seconds. Hiding may cost weeks or months of unnecessary fear.
A useful first sentence is: “I need to tell you something odd, and I do not want you to panic.” That gives the listener a job: stay calm. Families sometimes need instructions printed in large emotional font.
Mistake 2: Arguing With the Image All Day
Some people try to stare down the image or prove it wrong. They inspect the corner, check the wall, turn the light on and off, ask others repeatedly, or become trapped in a loop of testing. A little checking is understandable. All-day checking can make the symptom the center of the room.
A calmer strategy is to label, check safety, re-anchor, and return to the task. For example: “That may be a visual symptom. I am seated. I am safe. I will turn on the lamp and listen to the radio.” This is not pretending. It is refusing to let the image become the boss of the afternoon.
Mistake 3: Letting Family Members “Correct” Too Harshly
Caregivers may think they are helping by saying, “No, there is nothing there,” over and over. But blunt correction can feel humiliating, especially when the person already knows the image is not real. It can also make them less likely to share future symptoms.
Better: “I believe you are seeing it. I do not see it. Are you safe where you are?” That sentence is a bridge. It does not endorse the image as real. It respects the person’s experience and moves toward safety.
Decision Card: Correct the Image vs Support the Person
When the person is calm and safe: Use gentle language. Ask what they see, whether it is bothering them, and whether changing light or activity would help.
When the person is frightened or moving: Focus on safety first. Encourage sitting, better lighting, clear path, and medical follow-up if symptoms are new or unusual.
Time trade-off: A 20-second validating response can prevent a 20-minute argument.
Neutral action line: Practice one response before the next episode, so fear does not write the script for you.
- American Academy of Ophthalmology: What Is Charles Bonnet Syndrome?
- National Eye Institute: Vision Rehabilitation
- NHS: Charles Bonnet Syndrome
The Pattern Log: A Calm Notebook for a Strange Symptom
A symptom log sounds boring. Good. Boring is exactly the energy we want here. Charles Bonnet syndrome can feel strange enough without giving it a velvet notebook and a dramatic title. A simple log turns fog into usable information.
Track the Image Without Feeding the Fear
Create a short pattern log with columns for time, place, lighting, activity, emotion, sleep, medication changes, and what helped. You can use paper, a large-print notebook, a voice memo, a caregiver’s note, or a phone reminder. If you prefer a ready-made structure, a printable symptom diary for seniors can make the habit feel less like homework and more like a calm handrail. The format matters less than the habit.
Keep entries brief:
- “Tuesday, 8 p.m., living room, dim light, saw patterned shapes on wall, lasted 2 minutes, knew unreal, lamp helped.”
- “Friday morning, after poor sleep, saw small dog near kitchen, startled me, sat down, disappeared.”
- “Sunday night, bathroom route, dark hallway, saw person shape near door, felt unsafe, added night light.”
The log gives the doctor better information. It also gives the person a handle. Instead of “This is happening all the time,” the note may show “mostly evenings, mostly dim rooms, worse after poor sleep.” A pattern is not a cure, but it is a map. Even a rough map is better than wandering through emotional fog in slippers.
Separate “Interesting” From “Unsafe”
Some images are odd but harmless. A patterned wall, a silent figure, or a passing animal image may be disturbing without creating immediate danger. Other images may affect function: a person hesitates at stairs, avoids the bathroom at night, reaches toward something that is not there, loses sleep, becomes afraid to be alone, or stops cooking because the kitchen feels visually unpredictable.
That distinction matters. The goal is not to catalog every visual event like a museum curator of weirdness. The goal is to identify what changes daily life. If an image affects walking, bathing, cooking, medication use, sleep, driving, or emotional stability, it deserves special attention.
Tiny Rule: Write Less Than You Worry
A two-minute note is enough. The notebook is a lantern, not a second illness. If logging becomes obsessive, shrink it. Use checkboxes. Use one sentence. Ask a caregiver to help once a day instead of after every episode.
Here is a practical structure:
- What: pattern, person, animal, face, object, scene.
- When: date, time, and what you were doing.
- Where: room or situation.
- Safety: sitting, standing, walking, stairs, bathroom, driving, cooking.
- Helped: light, blink, look away, move, music, call, rest.
I like logs that can be completed before the kettle boils. Any longer and the log becomes a hobby nobody asked for.
Home Safety: When Hallucinations Meet Stairs, Bathrooms, and Night Walking
Insight helps. Knowing an image is not real helps. But insight does not remove fall risk. A person can know the pattern is unreal and still pause at the wrong moment, misread a step, reach poorly, or avoid turning on a light because they do not want to “make a fuss.”
Home safety is not an insult to independence. It is how independence gets a sturdier chair to sit in.
Make the Walking Path Boring on Purpose
A predictable home is kinder to low vision and less vulnerable to visual confusion. Keep floors clear. Avoid moving furniture casually. Improve contrast at steps and thresholds. Use night lights along bed-to-bathroom routes. Keep frequently used items in fixed locations. Reduce glossy glare where possible.
The Centers for Disease Control and Prevention has long emphasized that falls are a major risk for older adults. Vision changes, clutter, poor lighting, and night walking can all make that risk feel closer. When hallucinations enter the picture, the best home design is not fancy. It is boring, consistent, and easy to read.
Treat Bathrooms as High-Stakes Spaces
Bathrooms deserve special attention because they combine water, hard surfaces, low light, mirrors, turning, transfers, and sometimes urgency. It is a tiny room with the confidence of a mountain pass.
If images appear near the shower, toilet, mirror, or night bathroom route, prioritize non-slip surfaces, better lighting, contrast tape, grab bars where appropriate, and reachable supports. A simple upgrade such as anti-slip shower strips placed where feet actually move can be more useful than random coverage that looks safe but misses the standing and turning zones. Keep towels, soap, glasses, mobility aids, and medications in predictable locations. Avoid loose rugs. Check that lighting does not create harsh shadows that look like obstacles.
For some people, a mirror can be visually confusing in low light. If hallucinations often happen around a bathroom mirror, consider changing lighting, reducing glare, or covering the mirror temporarily during vulnerable times. A guide to bathroom mirror glare may help you think through angle, bulbs, and surface reflections without turning the room into a glare trap. The goal is not to make the home clinical. The goal is to stop the bathroom from auditioning for a suspense film at 2 a.m.
Don’t Let “I Know It Isn’t Real” Become a Safety Excuse
Many people with Charles Bonnet syndrome maintain insight. They know the images are not physically present. That is reassuring, but it should not become a reason to ignore safety.
Ask function-based questions:
- Do the images ever appear while walking?
- Do they show up on stairs or near thresholds?
- Do they make the bathroom feel unsafe?
- Do they interrupt cooking, medication use, or driving decisions?
- Do they cause sleep loss or fear of being alone?
If the answer is yes, the response should include environmental changes and clinical follow-up, not just reassurance.
Eligibility Checklist: Do You Need a Home Safety Mini-Review?
Answer yes or no:
- Do visual images appear while you are walking, bathing, cooking, or using stairs?
- Have you changed your routine because a room feels visually confusing?
- Do you get up at night to use the bathroom?
- Have you had a recent fall, near-fall, or “furniture grab” moment?
- Do you avoid turning on lights because you do not want to wake someone?
If 1 or more are yes: Start with one high-risk path: bed to bathroom, favorite chair to kitchen, or entryway to stairs.
Neutral action line: Fix one repeated route before buying new equipment.
- Prioritize night routes, bathrooms, stairs, and kitchens.
- Use consistent lighting and contrast.
- Keep furniture and essential items predictable.
Apply in 60 seconds: Walk the bed-to-bathroom route in daylight and remove one obstacle today.
Family Response: How to Help Without Taking Over
Caregiving around visual hallucinations requires a difficult balance: believe the person, protect safety, and avoid taking over the whole room with your anxiety. Families often swing between two unhelpful poles. One side dismisses: “You’re imagining things.” The other side panics: “We can’t leave you alone for a second.” Neither response feels good to the person living inside the experience.
Start With Belief, Then Move to Safety
Use a practical script:
“I believe you are seeing it. I do not see it, but I want to make sure you feel safe. Is it blocking your path? Do you want more light or a different seat?”
This approach respects the person without confirming that the image is physically real. It also avoids turning the conversation into a debate. Debates are for book clubs and city council meetings, not for a frightened person near a staircase.
If the person is calm and seated, you can ask what the image looks like, when it started, and whether it has happened before. If the person is moving, cooking, bathing, or near stairs, ask safety questions first. “Can you sit down?” may matter more than “What color was it?”
Ask Better Check-In Questions
Replace loaded questions with functional ones. Instead of “Are you hallucinating again?” try:
- “Have the images been more frequent this week?”
- “Are they showing up during walking, bathing, cooking, or bedtime?”
- “Do they make any part of the house feel unsafe?”
- “Are you sleeping less because of them?”
- “Did anything change with your vision, medication, or health recently?”
These questions are less shaming and more useful. They gather information about frequency, triggers, safety, and function.
Let’s Be Honest: Independence Is the Hidden Fear
Many older adults worry that admitting visual hallucinations will cost them trust, keys, privacy, or home independence. That fear is not irrational. Families sometimes overreact because they are scared. Clinicians sometimes have limited time. Systems sometimes treat risk like a switch: safe or unsafe, independent or not. Real life is more nuanced.
The goal is not to punish honesty. The goal is to reward honesty with better support. If a person says, “I saw a child near the hallway,” the family response should not immediately become, “You can never be alone.” A better response is, “Thank you for telling me. Let’s figure out when it happens and make that hallway safer.”
That sentence keeps dignity in the room. Dignity is not decorative. It is part of adherence, trust, and safety.
Coverage Tier Map: Family Support From Light Touch to Higher Concern
Tier 1: Occasional and not distressing — Encourage logging and routine eye care follow-up.
Tier 2: Repeating pattern — Add lighting changes, activity cues, and weekly check-ins.
Tier 3: Affects sleep or mood — Discuss with eye doctor or primary care clinician soon.
Tier 4: Affects walking, bathing, cooking, or driving — Prioritize home safety and prompt clinical review.
Tier 5: Sudden, confused, non-visual, or neurologic symptoms — Seek urgent medical help.
Neutral action line: Match support to function and safety, not to family fear alone.
When to Seek Help: The Red-Flag Section Readers Actually Need
This is the section to bookmark, print, or quietly tape inside the family brain. Charles Bonnet syndrome can be approached calmly, but calm does not mean casual. Some symptoms need prompt care because they may point to something beyond visual release hallucinations.
Call Promptly for New, Sudden, or Changing Symptoms
New visual hallucinations should be discussed with a clinician, especially if vision has recently worsened or the hallucination pattern changes sharply. If someone has had occasional patterns for months and suddenly begins seeing frightening scenes for long periods, that change deserves attention. If hallucinations begin after a medication change, infection, surgery, fall, or major sleep disruption, mention that clearly.
A prompt call may go to an eye doctor, primary care clinician, nurse advice line, pharmacist, or urgent care service depending on the situation. The exact path depends on symptoms, timing, severity, and local access. When in doubt, describe the change and ask where the person should be evaluated.
Seek Urgent Help for Neurological or Whole-Body Symptoms
Seek urgent help if visual experiences come with confusion, one-sided weakness, facial drooping, slurred speech, severe headache, fainting, seizure-like activity, fever, chest pain, sudden severe dizziness, recent head injury, or sudden major vision loss.
Those symptoms should not be tucked under the CBS umbrella. They may reflect urgent medical conditions such as stroke, infection, delirium, seizure, medication toxicity, or other serious problems. Nobody wins a prize for waiting bravely in the living room while the body is ringing alarm bells.
Review Medication and Sleep Changes
Medication side effects, interactions, sleep deprivation, dehydration, infection, and delirium can complicate the picture, especially in older adults. Bring a current medication list to appointments. Include prescription drugs, over-the-counter sleep aids, allergy medicines, pain medicines, supplements, eye drops, recent antibiotics, and anything newly started or stopped.
A pharmacist can be a useful ally here. Medication lists often become archaeological sites: old bottles, duplicate doses, “as needed” pills that quietly became daily, and sleep aids that arrived in the cart next to toothpaste. A one-page medication list template can help turn that archaeological site into something a clinician can actually review. A review can identify risks that are easy to miss at home.
Fee/Rate Table: Common Care Pathways and What They Usually Involve
| Care pathway | When it may fit | What to bring |
|---|---|---|
| Eye doctor visit | Known vision loss, new visual-only images, low vision questions | Symptom log, glasses, eye medication list, vision changes |
| Primary care visit | Medication changes, sleep issues, infection concerns, whole-body symptoms | Full medication list, timeline, recent illnesses or falls |
| Urgent or emergency care | Confusion, weakness, speech changes, severe headache, fall, fever, fainting | Symptom start time, emergency contacts, medication list |
| Low vision or occupational therapy support | Home safety, lighting, contrast, reading, daily task struggles | Hardest tasks, home layout concerns, current devices |
Neutral action line: Choose the care pathway based on symptom severity and safety, not embarrassment.
- Sudden neurological symptoms need urgent help.
- Medication and sleep changes matter.
- New or changing hallucinations should be reported.
Apply in 60 seconds: Keep an updated medication list with the symptom log.
Treatment Expectations: Relief May Mean Less Fear, Not Instant Disappearance
It is natural to want a switch. A pill. A lamp setting. A sentence from the doctor that makes the images disappear and sends everyone back to breakfast. Sometimes symptoms improve. Sometimes they fade. Sometimes they continue but become less frightening. Treatment expectations need to be honest, because overpromising is just fear wearing a nicer coat.
There May Not Be a Simple Cure
Many medical resources explain that there is no simple universal cure for Charles Bonnet syndrome. Management often focuses on education, reassurance, vision optimization, coping strategies, environmental changes, and ruling out other causes when symptoms do not fit the usual pattern.
That may sound disappointing, but it is not empty. Fear often shrinks when the person understands what may be happening. Distress may decrease when family responses improve. Safety may improve when lighting, contrast, and walking routes are changed. Daily life can get better even if the occasional image still appears.
Vision Care Still Matters
Vision care is not only about curing the underlying eye condition. It is also about preserving usable vision, improving function, and reducing confusion where possible. Updating glasses, addressing cataracts when appropriate, treating eye disease when possible, managing dry eye or glare, and using low vision tools may all help the person feel more oriented.
Ask the clinician whether anything can improve visual input or daily function. Sometimes the answer is medical treatment. Sometimes it is a magnifier, better task lighting, contrast labels, mobility support, or training. Sometimes it is accepting that the eye disease cannot be fully reversed while still improving the way the home works.
Measure Progress by Daily Life
Progress does not always look like “no more hallucinations.” It may look like better sleep. Fewer panic calls. Safer bathroom trips. More honest conversations. A caregiver who responds calmly. A person who can say, “That is the visual thing again,” and return to folding laundry.
Measure what matters:
- Are episodes less frightening?
- Is the person sleeping better?
- Are high-risk routes safer?
- Is the person telling someone when symptoms change?
- Is shame decreasing?
Those are not small wins. They are the scaffolding of independence.
Common Mistakes: What Readers Should Stop Blaming Themselves For
One of the quiet cruelties of strange symptoms is how quickly people blame themselves. They replay the episode. They wonder whether they caused it by worrying too much, reading too long, sleeping badly, aging badly, praying badly, or somehow failing to be sensible enough. Let’s remove that burden from the table.
Mistake: Assuming “I’m the Only One”
Charles Bonnet syndrome is recognized in people with visual impairment. Many people do not talk about it, so it can feel rarer and more shameful than it is. Silence creates a distorted mirror: everyone else seems fine because nobody is narrating their private symptoms at the pharmacy counter.
You are not required to announce it to the world. But telling a trusted person and a clinician can break the isolation. A symptom that can be spoken becomes easier to manage.
Mistake: Waiting for the Perfect Words
The doctor does not need a literary description. You do not need to explain the exact emotional tone of the face by the curtains or whether the pattern looked more like lace, tile, or an overly ambitious snowflake.
Start with this:
“I see things that are not there, and I know they are not real.”
Then add: when it began, how often it happens, whether it is visual only, whether anything else changed, and whether it affects safety. That is enough to begin.
Mistake: Designing the Home for Eyes That No Longer Exist
After vision loss, many homes remain set up for the old eyes. Same dim hallway. Same low-contrast step. Same dark bathroom route. Same glass coffee table quietly plotting against shins. Same medication bottles with tiny print designed by someone who has apparently never met a human retina.
Low vision asks the home to become more legible. Stronger contrast. Better lighting. Clearer routes. Fewer loose objects. Fixed locations. Larger labels. Safer nighttime paths. These changes are not admissions of defeat. They are design updates for the body you actually have now.
Charles Bonnet Syndrome Calm Plan Infographic
The 5-Step CBS Calm Plan
1
Name it
“This may be a visual symptom.”
2
Check safety
Sit down, pause walking, avoid stairs or cooking until steady.
3
Change the scene
Adjust light, blink, look away, move rooms, or re-anchor.
4
Log lightly
Write time, place, trigger, and what helped. Two minutes is enough.
5
Escalate wisely
Seek help for sudden change, confusion, weakness, fever, fall, or non-visual symptoms.
Short Story: The Pattern on the Curtains
Maria first noticed the pattern after dinner. Her vision had been changing for years, but that evening the curtains looked covered in tiny blue birds. She knew the fabric was plain beige. She also knew, with a cold little pinch in her stomach, that telling her son might make him worry about her living alone. For three nights she said nothing.
Then she wrote one sentence on a grocery receipt: “I see birds on the curtains at night, but I know they are not real.” At her eye appointment, she handed over the note before she could lose courage. The doctor did not laugh. Her son did not take over. They changed the lamp, cleared the path to the bathroom, reviewed medications, and made a plan. The birds did not become welcome guests. But they stopped being a secret jury.
FAQ
Can Charles Bonnet syndrome make you see patterns?
Yes. Some people see simple shapes or patterns, including lines, grids, dots, tiles, colors, or repeated designs. Others see more complex images such as people, animals, objects, landscapes, buildings, or full scenes. The images can be vivid even when the person knows they are not physically real.
Does Charles Bonnet syndrome mean dementia?
Not by itself. Charles Bonnet syndrome is commonly described as visual hallucinations in people with vision loss, often with preserved insight that the images are not real. However, new confusion, memory changes, personality changes, disorientation, unsafe behavior, or loss of insight should be discussed with a clinician. Do not assume every symptom is CBS just because vision loss is present.
Why do hallucinations happen after vision loss?
A common explanation is that reduced visual input can lead the visual brain to generate images on its own. When the eyes send less information, the brain may fill in the quiet places. This does not mean the person is choosing the images or inventing them for attention.
Should I tell my family?
Yes, if it is safe to do so. A trusted person can help you track patterns, reduce fear, improve lighting, clear walking paths, and support medical follow-up. For spouses and partners, a practical guide to helping a spouse with vision loss can make the conversation feel less like crisis management and more like shared problem-solving. You do not need to tell everyone. Start with one calm person who can listen without turning the room into a committee hearing.
Can lighting changes help?
Sometimes. Some people find that turning on a light, reducing glare, changing rooms, blinking, looking away, or changing activity helps interrupt the images. Lighting is not a guaranteed cure, but it is a low-cost coping experiment and often improves low vision safety anyway. If reading or close tasks are part of the problem, adjusting reading lamp position for central vision loss may also reduce visual strain and confusion.
Should I stop driving if I have Charles Bonnet syndrome?
Do not drive if visual images, low vision, medication effects, anxiety, or uncertainty make driving unsafe. Discuss driving safety with an eye doctor or clinician, especially if hallucinations occur in the car, at intersections, at night, or during visually demanding tasks. Driving decisions should be based on safety, vision status, local rules, and professional guidance. People with macular degeneration may also need a more specific look at night driving safety with macular degeneration.
Is there medicine for Charles Bonnet syndrome?
There is no simple universal medicine for Charles Bonnet syndrome. Management often focuses on reassurance, treating vision problems where possible, low vision support, environmental changes, coping techniques, and checking for other medical causes when symptoms do not fit the usual pattern. Medication decisions should be made with a clinician, especially for older adults or anyone taking multiple medicines.
What should I do during an episode?
Pause. Remind yourself, “This may be a visual symptom.” Check whether you are physically safe. Sit down if you are walking or feel unsteady. Adjust lighting, blink, look away, change activity, or move rooms if safe. Write a short note afterward if the episode was new, upsetting, or connected with a safety concern.
Can stress or boredom make it worse?
Some people notice images more during quiet, passive, lonely, or tired moments. Stress and poor sleep may also make symptoms feel harder to manage. A low vision activity menu, such as radio, audio books, safe tactile tasks, phone calls, music, or structured evening routines, may help reduce fear and attention on the images. For readers who use reflection as part of coping, journaling prompts for macular degeneration can offer a gentle way to name fear without letting it take the whole room.
What should caregivers avoid saying?
Avoid ridicule, panic, harsh correction, or repeated statements like “Nothing is there” in a scolding tone. Try: “I believe you are seeing it. I do not see it, but I want to help you feel safe.” Then ask whether the image is blocking a path, affecting a task, or causing distress.
Next Step: Make a One-Page “CBS Calm Plan”
The opening scene of this article was simple: a familiar room suddenly shows you something unfamiliar. That is what makes Charles Bonnet syndrome so unsettling. It does not arrive in a laboratory. It arrives near your mug, your curtains, your hallway, your bathroom mirror, your ordinary Tuesday.
The answer is not to turn every image into an emergency. It is also not to hide symptoms in the name of bravery. The wiser path is quieter: name it, track it, make the room safer, and get the right clinician in the loop.
One Concrete Action Today
Write down three things:
- What you usually see.
- When or where it tends to happen.
- Who you will tell if it becomes scary, frequent, changing, or unsafe.
Bring that page to your next eye care or primary care appointment. If the symptoms are sudden, changing, paired with confusion or weakness, or affecting safety, do not wait for a routine visit. Call promptly or seek urgent care as appropriate.
Add a Home Safety Mini-Check
Choose one high-risk zone: bed-to-bathroom route, shower, kitchen, stairs, or favorite chair. Improve one thing there today. Add a night light. Move a loose rug. Increase contrast. Clear a path. Put glasses and phone in the same place every night. A low vision bedside organization system can make the phone, glasses, water, drops, and light easier to find when the room is dark or visually confusing. Small changes are not small when they prevent a fall, a panic episode, or a silent week of fear.
End With the Sentence Readers Need
Seeing something after vision loss can be frightening, but you do not have to solve it alone, hide it, or turn every image into a verdict on your mind. Charles Bonnet syndrome is a real, recognized experience associated with vision loss, and the best response is both compassionate and practical: protect safety, tell the truth, track the pattern, and ask for help early.
Your 15-minute next step: create a one-page calm plan with your symptom sentence, red flags, trusted contact, clinician contact, and one home safety fix. That single page can turn a frightening private mystery into a manageable shared plan.
Last reviewed: 2026-04.