


When the Spreadsheet Bends: Identifying Diabetic Macular Edema
If you have diabetes and your central vision feels smudged, wavy, or oddly dim in one eye, the fear isn’t just blur. It’s the not-knowing: Is it a glasses problem, a dry-eye flare that hits in the afternoon, or something happening deeper in the retina?
Delay can cost you the easiest kind of win in eye care: catching swelling early, while treatment options are still straightforward.
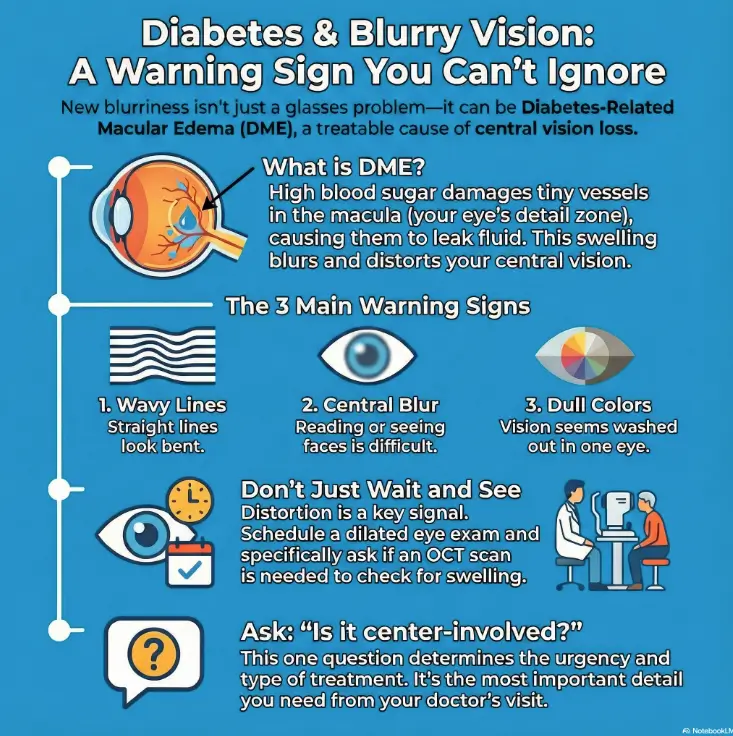
Diabetes-related macular edema (DME) is swelling in the macula—the retina’s detail zone—caused by leaky, stressed blood vessels from long-term high blood sugar. When the blood–retina barrier breaks down, fluid builds up and can blur or distort central vision, especially if it becomes center-involved.
This post helps you move from vague symptoms to a clear next step: what the one-eye test means, why OCT is the “receipt” of swelling, and how treatment decisions (often starting with anti-VEGF injections) are usually guided by trends—not guesswork.
Table of Contents
Safety first: what this can’t do
This article is educational. It can help you recognize patterns, ask better questions, and avoid common delays. It cannot diagnose you, rule out emergencies, or replace a clinician’s exam.
Go urgent today if you have sudden central vision loss, a new dark curtain/blank spot, severe eye pain, a serious headache with neurological symptoms, or vision changes after trauma.
Book soon (days to 1–2 weeks) if you have diabetes and any new distortion, central blur, or “one eye feels off”—even if the other eye seems fine.
- One-eye changes can hide for weeks.
- DME is often treatable, especially early.
- Urgency depends on speed and severity of change.
Apply in 60 seconds: Cover one eye, then the other, and look at straight lines (window blinds count). Notice waviness or a missing patch.
A familiar moment: you hold your phone farther away, bump the brightness, squint—then quietly wonder if you’re being dramatic. With DME, that “maybe it’s just my eyes today” story can be the biggest delay.
Money Block: 60-second eligibility checklist (not a diagnosis)
- Yes/No: Do straight lines look wavy in one eye?
- Yes/No: Is the blur mostly in the center (reading/faces), not the edges?
- Yes/No: Do colors look duller or “washed out” in one eye?
- Yes/No: Do you have diabetes (type 1 or type 2) or a long history of high blood sugar?
Neutral next step: If you answered “yes” to any of the first three, schedule a dilated eye exam and ask whether an OCT is needed.
DME in 30 seconds: the “leak in the macula” model
Macula = reading/faces (why central blur feels personal)
The macula is the retina’s “detail zone.” It’s what makes tiny text readable, faces recognizable, and road signs crisp. When the macula swells, your vision doesn’t always go black—it goes soft, warped, or smudged right where you need precision.
Blood–retina barrier = waterproofing (what fails in diabetes)
Your retina has a protective barrier that keeps fluid where it belongs. Long-term high blood sugar can damage small vessels and weaken that barrier. When it fails, fluid leaks into retinal tissue like rain into drywall—swelling the macula and blurring the image your eye is trying to deliver to your brain.
A familiar moment: you can still see the clock across the room, but the text on a receipt looks like it’s been lightly smeared with a finger. That pattern—distance okay, reading not okay—often pushes people to the eye doctor.
Show me the nerdy details
DME is closely tied to microvascular damage and breakdown of the blood–retina barrier. That leak increases retinal thickness (often measured by OCT), and the location of fluid relative to the foveal center helps guide management decisions.
Sugar → swelling chain: how high glucose turns into fluid
Barrier breakdown + leaky capillaries (the first domino)
High glucose over time stresses tiny retinal vessels. Think of it as wear and tear on the plumbing: vessel walls become more fragile, and the retina’s “tight seals” loosen. Once that happens, fluid and proteins slip out into retinal tissue—especially in the macula, where the architecture is tuned for precision, not padding.
VEGF + inflammation: the leak amplifier
When retinal tissue is stressed, it can release signals that increase vessel permeability. One well-known signal is VEGF (vascular endothelial growth factor). In plain English: it’s the body trying to help tissue survive—but it can also make vessels leakier, which feeds swelling.
Why swelling blurs (light can’t land cleanly on the receptors)
Your retina is meant to be thin and orderly. Swelling disrupts that order. Light that used to land precisely now scatters across “puffed up” layers, and your brain receives a fuzzier signal. That’s why DME can cause blur, distortion (straight lines bend), and a feeling that one eye is “lagging.”
Here’s what no one tells you…
Swelling and vision don’t always move in lockstep. Some people have measurable swelling with only mild symptoms; others feel dramatic distortion early. That’s why “I can still read okay” isn’t a reliable safety signal.
High blood sugar stresses small retinal vessels
Blood–retina barrier weakens (“waterproofing” fails)
VEGF/inflammation increases leakage
Macula swells (fluid in the detail zone)
Blurry or distorted central vision (reading/faces)
Accessibility note: This flowchart summarizes a common pathway; an eye exam is required to confirm DME or other causes.
A familiar moment: you read one line fine, then the next line “swims” and you blame the lighting. DME often shows up as inconsistency—good moments and bad moments—because the visual system is constantly compensating.
The symptom fingerprint: what DME vision actually looks like
Blurry center vs wavy lines vs dull color (quick tells)
DME commonly affects the center of vision. People describe it as:
- Central blur that makes letters look slightly smeared
- Distortion where straight lines look bent or wavy
- A “missing patch” or smudge that doesn’t blink away
- Duller color in one eye compared to the other
One-eye cover test (20 seconds) + what a “fail” means
Cover your left eye and look at straight lines (window blinds, a door frame, a spreadsheet grid). Then switch. If one eye shows waviness, blur, or a missing spot that the other eye doesn’t, it’s a strong reason to get evaluated promptly. It doesn’t prove DME—but it’s a useful flag.
Curiosity gap: why your brain hides one-eye blur until it doesn’t
Your brain is a generous editor. If one eye is weaker, it quietly borrows the sharper eye’s signal and “fills in” the gaps. That’s why some people don’t notice anything until reading speed drops, night driving feels risky, or a routine diabetes eye exam finds swelling first.
Money Block: mini urgency “calculator” (3 inputs, educational)
Pick the closest match:
- Speed: sudden (hours–1 day) / gradual (days–weeks)
- Pattern: distortion (wavy lines) / blur only / dark spot
- One-eye test: clearly different between eyes (yes/no)
Output: Sudden + dark spot or severe distortion → treat as urgent. Gradual + one-eye difference → book soon and request dilated exam + OCT discussion.
Neutral next step: Use this to schedule appropriately, not to self-diagnose.
A familiar moment: you pass an eye chart at your primary care visit and think, “Okay, I’m fine.” A chart can miss early macular problems—because it’s not measuring distortion, fluid location, or the “one-eye vs the other” difference. (If you want a practical, bring-it-with-you structure, this annual eye exam checklist for seniors is the kind of simple list that keeps visits from turning vague.)
“Center-involved” is the fork in the road
Center-involved vs non-center-involved: what changes clinically
“Center-involved” means the swelling affects the very center of the macula (the fovea), where detail vision is highest. This matters because it often changes:
- Urgency (how quickly treatment is considered)
- Monitoring (how often OCT is repeated)
- Treatment strategy (which options are favored first)
Let’s be honest…
If you leave an eye visit without knowing whether your DME is center-involved, you’re missing the detail that turns a scary word into a clear plan. Ask it directly. It’s a fair question, not a “difficult patient” moment.
- It links symptoms to OCT findings.
- It helps explain why treatment may start sooner.
- It gives you a measurable goal: reduce central swelling.
Apply in 60 seconds: Write the question now: “Is it center-involved, and what’s the follow-up interval?” Bring it to the visit.
A familiar moment: you nod through the visit, then realize in the car you didn’t actually understand the plan. “Center-involved?” is an anchor question that makes the rest make sense.
Why now? The flare triggers most pages bury
The control triangle: glucose, blood pressure, lipids (eyes care about all three)
DME risk isn’t only about blood sugar. Eyes respond to the whole metabolic “weather system.” Many clinicians emphasize a triangle: glucose control, blood pressure control, and lipid management. You don’t need perfection—just fewer spikes and fewer long stretches of uncontrolled stress on vessels.
Kidney/fluid balance signals (why systemic swelling can echo in the retina)
When the body’s fluid balance is off—sometimes due to kidney issues that can accompany diabetes—swelling can show up in places you didn’t expect. This doesn’t mean “kidney problem = DME,” but it’s a reason eye doctors sometimes ask about broader health changes.
Medication curveballs (steroids; some diabetes meds) — “ask, don’t guess”
Some medications can push blood sugar higher (steroids are the classic example). Other diabetes medications have complex effects on fluid and weight. Don’t stop anything on your own—just mention recent changes to your eye clinician so the timeline makes sense. (If you’re trying to make sense of a scary timeline, including newer diabetes medications, you may also want to read semaglutide and sudden vision loss in seniors as a “questions to ask” companion—not a self-diagnosis tool.)
Open loop: why DME can show up at any retinopathy stage
People expect a neat sequence: “first retinopathy, then DME.” Reality can be messier. DME can appear with mild, moderate, or advanced diabetic eye disease. That’s one reason routine screening exists: it catches the messy timeline before symptoms get loud. If you’re rebuilding the bigger picture, start with a clear explainer on diabetic retinopathy, because DME often lives in that neighborhood—even when the symptom story is mainly blur.
Show me the nerdy details
Systemic factors influence microvascular permeability and retinal stress. Clinicians often look at overall cardiometabolic control when assessing risk and recurrence, even when local ocular treatment is planned.
A familiar moment: you’ve been “pretty good” lately, but life got loud—holidays, travel, missed meds, stress eating—and then vision feels different. Bodies keep score in delayed ways; the eye is one of those scoreboards.
The test that settles it: what happens at a real DME workup
Dilated exam vs retinal photos (screening vs decision)
Retinal photos can screen and document changes. A dilated exam lets the clinician assess the retina directly. For DME decisions, photos alone may not be enough—because the key question is often fluid and thickness at the macula. (If you’re wondering how often to do this even when you feel “fine,” see how often seniors should get dilated eye exams.)
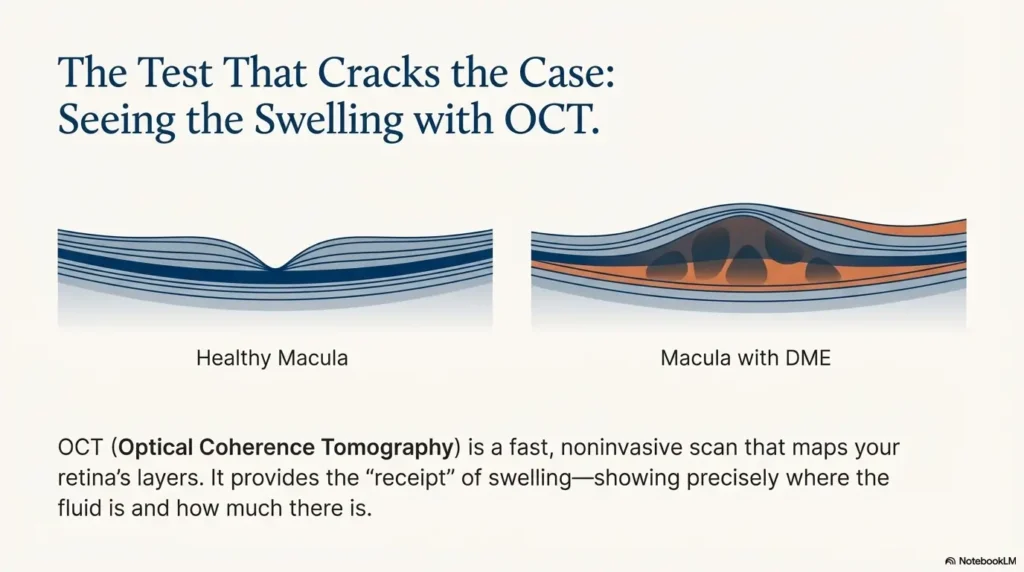
OCT: thickness + fluid location (the “receipt” of swelling)
OCT (optical coherence tomography) is a fast scan that maps the retina’s layers and thickness. It’s the test that turns vague words like “swelling” into something measurable: where the fluid is, how much thickening exists, and whether the center is involved.
Fluorescein angiography: when leak-mapping matters
Sometimes clinicians use fluorescein angiography to see patterns of leakage and blood flow. It’s not required for everyone, but it can help in certain scenarios—especially when the plan is unclear or the disease behaves unpredictably.
Quick table: what each test answers
💡 Read the Cleveland Clinic DME guidance
A familiar moment: you hear “OCT” and imagine something dramatic. In most clinics it’s quick, noninvasive, and oddly anticlimactic—like a photo booth for your retina. But it’s also the kind of anticlimax that gives you clarity.
Treatment, but with decision logic (not a menu dump)
Anti-VEGF injections: first-line for many center-involved cases (what “loading” means)
If DME is affecting the center, many retina specialists consider anti-VEGF injections because they can reduce leakage and swelling. The early phase often involves a series of injections close together (sometimes called a “loading” period), followed by adjustments based on response. The most important framing: it’s usually a plan, not a one-time event. (If you want a patient-friendly sense of what “a plan” can look like over time, see this injection schedule overview—the disease is different, but the rhythm of “monitor → treat → adjust” will feel familiar.)
Steroids: when they show up (tradeoffs: pressure/cataract risk)
Steroids can help reduce inflammation and swelling in certain cases. They’re not “better” or “worse”—they’re a different tool with different risks, including potential increases in eye pressure and cataract progression in susceptible people. Your clinician balances those tradeoffs with your specific situation.
Laser today: targeted tool, not the default hammer
Laser therapy still exists in the DME toolbox, often in more targeted ways than in the past. The right question isn’t “laser or no laser,” but “what problem are we solving with laser in my case?”
Surgery: the “different problem” category (traction/interface issues)
Sometimes swelling persists because of mechanical factors—pulling or traction at the macula. In those cases, the conversation shifts from “leak control” to “structure,” and a surgical option may enter the room. This is not common for everyone, but it’s useful to know why a plan might pivot.
Curiosity gap: what it means when swelling “persists” after injections (and the next pivot)
“Persistent fluid” doesn’t automatically mean failure. It can mean the retina needs more time, a different dosing schedule, a different medication class, or evaluation for other contributing factors. Ask what “success” looks like in your plan: vision improvement, OCT improvement, or both.
- Anti-VEGF often targets leakage signals like VEGF.
- Steroids can be helpful in selected cases, with specific risks.
- Ask for a goal you can track: symptom change and/or OCT change.
Apply in 60 seconds: Write down your “success metric” question: “What change on OCT tells us this is working?”
Show me the nerdy details
Management often blends anatomy (where the fluid is), physiology (signals increasing permeability), and patient context (ability to follow up, ocular pressure history, lens status). OCT findings can guide adjustments over time.
Money Block: Decision card (When A vs B)
- Center-involved swelling
- OCT shows fluid close to the fovea
- Goal is to reduce leakage and thickness
- Incomplete response over time
- Inflammation-heavy pattern suspected
- Clinician-specific risk balancing (pressure, cataract)
Neutral next step: Ask your clinician which “bucket” your case fits and what factor drives that choice.
A familiar moment: you hear “injection” and your body tenses like it’s bracing for a needle the size of a bicycle pump. The actual experience is usually more “weird pressure and blinking” than “pain horror story,” but anxiety is normal. Bring it up—clinics have ways to make it tolerable. (If it helps to read someone’s fear in plain language, this injection-anxiety guide for older adults can make the room feel less lonely.)
Short Story: A Tuesday appointment that changed the plan (120–180 words) …
Short Story: Jordan had been blaming the blur on screen time. The first clue was small: the spreadsheet grid looked slightly bowed in the right eye. At the diabetes eye exam, the clinician did a dilated exam, then an OCT. The result wasn’t dramatic in the mirror—no redness, no obvious “injury”—but the scan showed fluid near the center of the macula. Jordan expected a lecture about “better control” and a vague follow-up.
Instead, the plan was concrete: define whether it was center-involved, set a follow-up interval, and discuss treatment options with a retina specialist. The biggest surprise was how much calmer it felt once the problem had a name and a measurement. The blur didn’t vanish overnight, but the guessing stopped. And that—oddly—was the first real improvement.
Common mistakes that quietly cost vision
Mistake #1: “I’ll wait for it to clear” when lines look wavy
Distortion is a strong signal that the macula may be involved. Waiting weeks to “see if it passes” is one of the most common delays—especially if the blur comes and goes.
Mistake #2: Treating DME like a glasses problem (skipping dilation/OCT)
New glasses can help many things. But if the issue is swelling in the macula, the solution won’t be stronger lenses. A refraction-only visit can miss what an OCT would reveal.
Mistake #3: Stopping injections early because vision feels better
Feeling better is good news—but it doesn’t always mean the underlying swelling is fully stable. Follow-up matters because DME is often managed over time. If visits feel like a burden, talk about scheduling realities and what “minimum safe follow-up” looks like.
Mistake #4: Fixating on A1C only (ignoring BP/lipids)
A1C matters. But so does blood pressure and other vascular risk factors. Eye outcomes often reflect the whole system’s stability, not just one number.
Fast table: mistake → better move
- Wait-and-see → schedule evaluation when distortion appears
- Glasses-only thinking → ask about dilation and OCT when central blur is new
- Stop early → confirm the plan’s end point (symptoms, OCT, or both)
- One-number focus → treat glucose + blood pressure stability as a team sport
A familiar moment: you feel guilty, like DME is a moral judgment. It isn’t. It’s biology plus time plus risk factors. Shame doesn’t improve outcomes; a plan does.
When to seek help: urgent vs soon vs routine
Urgent today: sudden central blur/distortion, dark spot, severe pain, neuro signs
Sudden changes deserve same-day attention. The goal is not to panic—it’s to avoid missing conditions that need fast care.
Soon (days–1–2 weeks): progressive blur, new distortion, known retinopathy with any change
Many DME cases are not “ambulance emergencies,” but they are time-sensitive. Booking soon can be the difference between treating early and treating late.
Routine (but don’t skip): no symptoms ≠ no risk (screening still matters)
Diabetic eye disease can progress quietly. Regular eye exams exist because symptoms often arrive late to the party. If you’re sorting out the practical side—what to book, what it’s called, and how billing can differ—start with Medicare diabetic eye exam cost and booking guidance.
- One eye can compensate for the other.
- Distortion is more concerning than mild blur.
- Routine screening catches silent changes.
Apply in 60 seconds: Put a reminder on your phone: “One-eye check weekly until my appointment.”
FAQ
Is diabetic macular edema the same as diabetic retinopathy?
They’re related but not identical. Diabetic retinopathy describes diabetes-related damage to retinal blood vessels broadly. DME is swelling in the macula that can occur alongside retinopathy and can drive central vision symptoms.
Can DME go away if I lower my blood sugar?
Improving glucose stability supports overall vessel health and can reduce ongoing stress, but DME doesn’t always disappear quickly just from better numbers. Many people need eye-directed treatment plus systemic control. Think “team approach,” not “one lever.”
What does “center-involved DME” mean—and why does it matter?
It means swelling affects the foveal center of the macula. It matters because it often changes urgency, monitoring frequency, and which treatments are discussed first.
Do anti-VEGF injections hurt, and how often will I need them?
Most clinics use numbing drops and antiseptic prep. People often describe pressure or weirdness more than pain. Frequency varies by plan and response—ask what the initial phase looks like and how adjustments are made over time.
What does an OCT actually show in DME?
OCT shows cross-sections of retinal layers, thickness, and fluid pockets. It helps answer “where is the fluid?” and “is the center involved?” and it provides a baseline to track change.
If one eye is blurry, is that still DME?
Yes—DME can affect one eye more than the other. The brain often compensates, which is why one-eye testing is useful for noticing differences early.
Can I drive if I have DME?
Driving safety depends on your visual acuity, contrast sensitivity, and distortion level. If signs look smeared, lines are wavy, or you’re unsure, avoid risky conditions (night, rain) and ask your clinician directly about driving safety. (If you’re trying to separate “retina blur” from “screen blur,” digital eye strain in seniors can help you name what’s what before you assume it’s just screens.)
What happens if I miss injections or follow-ups?
DME management often depends on monitoring and timing. Missing visits can allow swelling to return or persist without being noticed. If scheduling is hard, ask for a plan that matches your reality—clinicians would rather adjust than lose you to follow-up.
Does Medicare/insurance usually cover OCT and injections?
Coverage varies by plan and medical necessity documentation. In the US, OCT and medically indicated treatments are commonly covered, but out-of-pocket costs can differ. Your clinic’s billing team can help you verify benefits before treatment starts. If injections are on the table and you’re trying to understand coverage language ahead of time, this can pair well with Medicare coverage for Eylea injections.
Next step: one concrete action
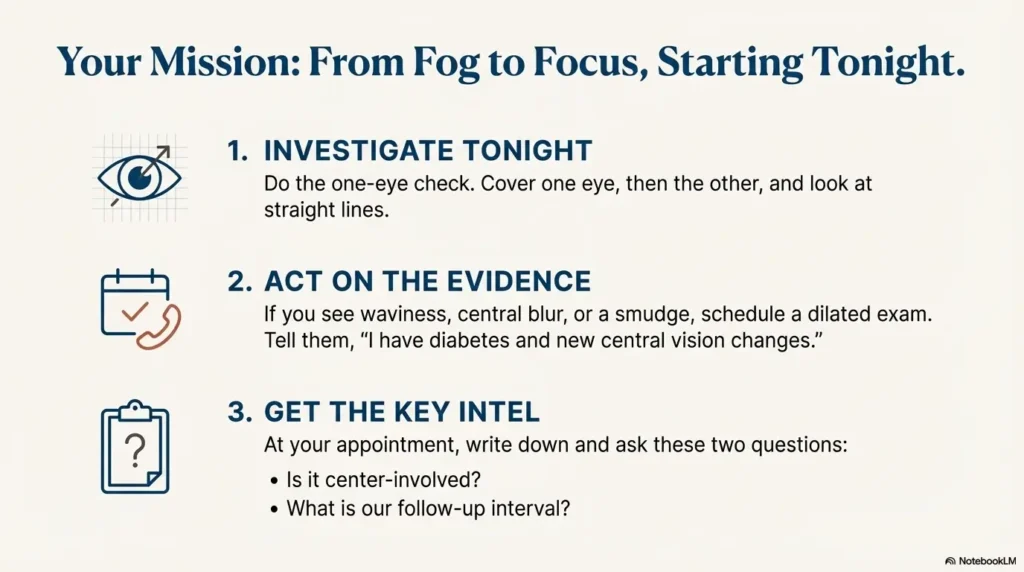
Do the one-eye check tonight (reading small text or a grid-like pattern)
Cover one eye and look at straight lines. Then switch. If one eye shows waviness, blur, dull color, or a missing patch compared to the other, treat that as a reason to schedule a dilated exam.
If one eye shows waviness/dull color/blur → schedule a dilated eye exam + OCT discussion
When booking, you can say: “I have diabetes and new central blur/distortion. I’d like a dilated exam, and I’m concerned about macular edema.” If you’re already seeing an optometrist, ask whether a retina specialist evaluation is appropriate.
Ask this exact question: “Is it center-involved, and what’s the treatment plan + follow-up interval?”
That single question transforms “I’m scared” into “I have a plan.” It also closes the loop from the very first worry: central blur is frightening because it feels vague—until you measure it.
Money Block: appointment prep list (bring these, save time)
- Current medication list (including recent changes and any steroid use)
- Recent A1C and blood pressure readings (if you have them)
- Any previous eye records (OCT reports, retinal photos, injection history)
- Your symptom timeline: “started X days/weeks ago,” one eye or both
- Two questions written down: “center-involved?” and “follow-up interval?”
Neutral next step: Put this list in your phone notes so you don’t rely on memory in the waiting room.
💡 Read the National Eye Institute macular edema page
💡 Read the NCBI Bookshelf clinical overview of DME
Closing the hook’s open loop: central blur feels terrifying because it threatens the parts of life that feel most human—reading, faces, and trust in your own eyes. The good news is that DME is often a treatable problem when it’s recognized and followed. The fastest win you can get in the next 15 minutes is simple: do the one-eye check, write the two questions, and book the right exam.
Last reviewed: 2025-12.