


Dry Eye and Oral Antihistamines: Claritin vs Zyrtec vs Allegra
Your allergy pill can calm your sinuses and still make your eyes feel like sandpaper by 4 p.m.—even on a “non-drowsy” label day. If you’re comparing dry eye and oral antihistamines—Claritin vs Zyrtec vs Allegra—the frustrating truth is that the box name often matters less than the conditions you’re taking it in.
Dry eye isn’t just “not enough tears.” It’s a tear film that breaks up too fast—because of evaporation (MGD/blepharitis), low humidity, airflow, long screen stretches, contacts, or post-LASIK sensitivity—so friction shows up as burn, grit, blur-that-clears-when-you-blink, or even watery “panic tears.”
Keep guessing and you don’t just stay uncomfortable—you stack meds, rub more, and turn a manageable season into a daily grind.
This post helps you identify your likely pattern (loratadine vs cetirizine vs fexofenadine), stop the common traps, and run a clean 7-day tracker so your eyes give you a usable answer.
No heroics—just one-variable testing and boring competence.
Here’s the part most guides skip: The “least drying” rumor, explained. Then the amplifiers that decide everything.
- Spot your dryness driver fast
- Pick a safer swap (including nasal/local options)
- Track results without muddy data
Table of Contents
Safety / Disclaimer
This is educational information, not medical advice. Don’t stop prescribed medications without clinician guidance. Get urgent care for vision changes, significant eye pain, marked light sensitivity, thick discharge, or sudden one-sided swelling—especially if you wear contact lenses or recently had eye surgery.
- Red flags beat internet advice.
- Contact lens wearers have a lower threshold for evaluation.
- Dry eye can mimic allergy eye symptoms and vice versa.
Apply in 60 seconds: Do a quick self-check: pain? light sensitivity? vision change? If yes—stop tinkering and get evaluated.

Dry-eye verdict: Claritin vs Zyrtec vs Allegra (2026)
If you came here for a simple ranking—“Zyrtec is worst, Allegra is best”—I get it. I also want one neat answer that doesn’t require a spreadsheet. But with dry eye, the more honest truth is this: your baseline eye surface (contacts, LASIK/PRK, MGD/blepharitis, screen hours, low humidity) often matters more than the brand name on the box.
So what’s the verdict? Many dry-eye-prone people start by tolerating Allegra (fexofenadine) or Claritin (loratadine) better than Zyrtec (cetirizine)—but “better” can mean “less dryness,” “less sedation,” or “enough relief without extra dosing.” And those are different goals.
Quick scorecard: what to watch (not a universal ranking)
| Medication | When it “feels drying” | Who notices fastest | Best first move |
|---|---|---|---|
| Claritin (loratadine) | Late afternoon / long screen stretches | Contact lens wearers, “blur that comes and goes” folks | Track timing + add environment fixes first |
| Zyrtec (cetirizine) | After stronger symptom suppression or dose stacking | Dry-eye baseline + heavy allergy days | Avoid “more is more”; consider local options |
| Allegra (fexofenadine) | When dryness is driven by MGD / humidity / airflow | People who “still feel dry on everything” | Treat the amplifiers; don’t expect a magic pill |
The surprising part: “watery eyes” can still mean dry eye
Yes, really. Allergy tears can be reflex tearing—your eye’s panic sprinkler system—while the tear film is still unstable. I learned this the hard way the first spring I tried to “power through” pollen season: my eyes watered in the grocery store aisle… and burned in the car ride home.
Who this is for / not for (fast filter)
- For you if: allergies + gritty/burning sensation, fluctuating vision, contact lens discomfort, “I blink a lot” days.
- Not for you if: severe pain, strong light sensitivity, thick discharge, sudden vision change, or post-op eye recovery.
Money Block: Eligibility checklist (quick yes/no)
- Yes/No: Do your eyes feel worse within 2–6 hours of an oral antihistamine?
- Yes/No: Do you wear contacts, have had LASIK/PRK, or have known MGD/blepharitis?
- Yes/No: Are you in heated/AC indoor air for 6+ hours/day?
Next step: If you answered “Yes” to 2+ items, skip the guessing game and use the 7-day A/B test section below (or print a simple tracker like this printable symptom diary format so you don’t lose the data).
Neutral action: Screenshot this checklist and use it as your starting baseline.
Tear-film trade: why antihistamines can dry eyes
Dry eye isn’t just “not enough tears.” It’s often a tear film that doesn’t stay stable long enough to protect the surface of your eye. The National Eye Institute explains dry eye in plain terms: either your eyes don’t make enough tears, or your tears don’t work correctly. That “don’t work correctly” part is the sneaky one.
Tear film in 60 seconds: oil + water + mucin
- Oil layer: slows evaporation (often impacted by MGD).
- Watery layer: provides moisture and clears debris.
- Mucin layer: helps tears spread evenly (think: “paint primer”).
Let’s be honest… you notice tear problems after friction starts
Most of us don’t notice “tear instability.” We notice the fallout: burning, sandy feeling, blurry vision that clears when you blink, or the urge to rub your eyes like you’re trying to erase the day.
The evidence line (context, not fear)
Systemic medications can influence tear production and tear stability. That’s why ophthalmology sources routinely flag allergy medications—especially oral antihistamines—as potential dry-eye aggravators. The key is not panic. It’s matching the strategy to your biggest driver.
Show me the nerdy details
Dry eye is commonly discussed as a homeostasis problem: the tear film loses stability, leading to surface stress and symptoms. Oral antihistamines can add a “drying pressure” system-wide, which may matter more in people with evaporation issues (MGD) or high screen time (reduced blink rate). That’s why two people can take the same medication and have totally different eye outcomes.
- If you’re in dry indoor air, symptoms intensify.
- If you blink less (screens), tears evaporate faster (especially for people dealing with digital eye strain patterns).
- If you have MGD, the “oil seal” is already weak.
Apply in 60 seconds: Take one deep breath, then check your room: fan/vent? heater? low humidity? Fix the air before you blame the pill.
Claritin pattern: loratadine’s “late-day drift”
Claritin is the friend who shows up on time, helps you move a couch, and then quietly leaves before the pizza arrives. For some people, it’s smooth. For others, it’s smooth until late afternoon—when your eyes suddenly feel like they’ve been open since 2009.
When Claritin feels “fine”… until screens pile up
This is a common pattern: morning is okay, lunchtime is okay, and then—around the “one more email” hour—your eyes start to sting. I used to blame the laptop. Then I noticed it tracked with allergy pill days, not workload days.
Contacts as an early-warning sensor
If you wear contacts, your lenses will tell the truth before your mirror does. Dryness often shows up as reduced lens comfort, more frequent rewetting drops, or that “lens is slightly off” feeling even when it isn’t—especially if you’re already juggling meds and lenses (if that’s your life right now, keep this handy: how drops interact with contact lens wear).
Timing tweak: morning vs evening
If your dryness is worst at night, try discussing timing with a clinician or pharmacist. Sometimes the win isn’t “new medicine.” It’s “same medicine, smarter timing.” (No heroics. No double-dosing. Just boring competence.)
Money Block: Quote-prep list (what to gather before you compare)
- Your current med + dose + time taken (e.g., 10mg at 8am).
- Baseline risk: contacts, LASIK/PRK, known MGD/blepharitis.
- Your top 2 symptoms: burning vs blur vs watering vs itch.
- Environment: heater/AC, fan, screen hours, humidity estimate.
Why this matters: it helps your clinician/pharmacist recommend a swap (or a non-pill strategy) faster.
Neutral action: Put this list in your notes app before your next pharmacy run.
Zyrtec tradeoff: cetirizine and “strong relief, drier eyes?”
Zyrtec often feels like it hits harder for allergy symptoms. That can be a blessing on high-pollen days. But if you’re dry-eye prone, “stronger relief” sometimes comes with a trade: your eyes feel more exposed, more reactive, or more “tired” even when you slept.
Why “stronger” can change the eye story
When your nose finally calms down, it’s tempting to assume the whole allergy picture is solved. But your eyes run a different operation. Allergies can irritate the eye surface, and an oral antihistamine can also reduce moisture signals—so you can end up with less itch and more friction. Fun combo. Zero stars. Would not recommend.
Here’s what people skip… dose stacking is the fastest way to lose
It’s not uncommon to stack: pill + “sinus” combo product + another “just in case.” This is where dry eye can jump from annoying to relentless.
Don’t do this: doubling doses to chase a “clean nose”
If you’re not getting relief, the answer usually isn’t “more.” The safer path is switching strategies: nasal-first options, local eye options, or clinician guidance—especially if you have eye-surface disease or wear contacts.
If you already took it: same-day comfort triage
- Stop rubbing (I know. I know.)
- Use preservative-free lubricating drops if you tolerate them (this quick guide to preservative-free eye drops can help you avoid the “random bottle roulette” problem).
- Take a 20-second blink break every 20 minutes for 2 hours.
- Reduce airflow directly at your face (fan/vent).
Mid-article check-in: If you’re feeling, “Okay, but I still want official guidance,” here’s a clinician-led explainer that connects allergy meds and dry eye in plain language. Read the official dry eye and oral antihistamines (Claritin vs Zyrtec vs Allegra) guidance
Allegra nuance: fexofenadine and the “least-drying” rumor
Allegra gets a reputation—especially online—as “the least drying.” Sometimes that’s true for an individual. But it’s not magic. If your dryness is driven by evaporation (MGD, airflow, low humidity) rather than just tear volume, switching brands can feel like rearranging deck chairs on a windy boat.
The myth: “non-drowsy” = “non-drying”
“Non-drowsy” describes sedation, not tear film behavior. It’s a different target. Different problem. Different scoreboard.
Here’s what no one tells you… nose-first strategies can spare your eyes
When you reduce the need for systemic meds, your eyes often get happier. That’s why many eye doctors encourage a “nasal-first” approach for some patients: get inflammation under control locally, then use the lowest systemic dose that actually helps.
When Allegra still dries you out: 3 common scenarios
- Indoor air: heat/AC + low humidity for 6–10 hours.
- Screen stretches: blink rate drops; evaporation climbs.
- MGD/blepharitis: oil layer is compromised, so tears evaporate quickly.
Personal note: I once switched brands and felt triumphant for exactly one day—then the office heater turned on and my eyes went back to “crunchy audiobook narrator.” Lesson learned: environment can overpower medication choice.
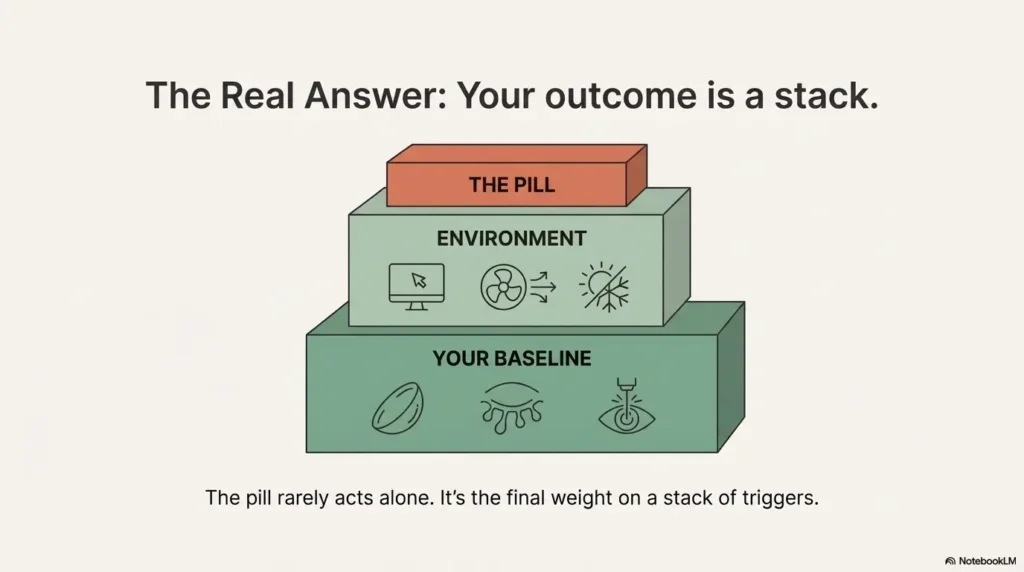
Dry-eye amplifiers: the real culprits that decide your outcome
Dry eye is rarely one villain with a neat confession. It’s more like a group chat. Antihistamines are in there… but so are your vents, your blink rate, your eyelid oil glands, your contact lenses, and sometimes your sleep setup.
MGD/blepharitis: the evaporation engine
If you have MGD, tears evaporate faster because the oil layer isn’t doing its job. That means even a small “drying pressure” from medication can feel huge. Many people think they have “watery tears” when they actually have evaporation plus reflex tearing.
Contacts + LASIK/PRK: why your baseline is different
Contacts are a stress test for the tear film. LASIK/PRK can change ocular surface sensation. If you’re in either group, you may need a more conservative plan and a lower threshold for targeted dry-eye treatment.
Indoor heat + low humidity: the invisible dehydration tax
My least glamorous dry-eye fix has also been my most effective: turning the vent away from my face. Not sexy. Very effective. Dry indoor air can turn “mild dryness” into “why do my eyeballs feel like toast?”
CPAP airflow + antihistamines: the double-hit combo
If you use CPAP and get air leaking toward your eyes, that airflow can amplify dryness dramatically. Add an oral antihistamine on top and you can feel punished for trying to breathe and exist in springtime. If this sounds familiar, start with the boring fix: how to handle CPAP mask leaks that blow air into your eyes (because fixing airflow at the source beats improvising near the eyelids).
How to use this: If your “bars” are high, your best ROI is often fixing the stack—not hunting for a mythical perfect pill.
Common mistakes: 7 dry-eye traps during allergy season
Dry eye loves good intentions. It thrives on “I’ll just do a little more.” Here are the mistakes I see constantly—plus the simple swaps that actually work.
Mistake #1: treating the nose with a pill when a spray would do better
Oral antihistamines are convenient. But if your biggest symptoms are nasal congestion and sneezing, a nasal-first plan (discussed below) can reduce how much systemic medication you need.
Mistake #2: combo products (antihistamine + decongestant) without noticing the dryness jump
“All-in-one” cold/sinus products can dry secretions by design. That may help your nose—while making your eyes feel worse. Read labels. Keep it boring.
Mistake #3: redness relievers as “dry eye drops”
Redness-relief drops can backfire for some people and don’t treat tear film instability. If you need drops frequently, it’s a sign to reassess strategy.
Don’t do this: blocking vents or taping near the eye without clinician guidance
If airflow is blasting your eyes (fan, vent, CPAP leak), fix the source. Don’t improvise solutions that could irritate skin or the eye area.
Mistake #5: “tightening” your way out of contact lens discomfort
When contacts feel dry, people often push longer wear time, add random drops, and hope. A smarter move: shorten wear time temporarily and fix the tear film stack.
Mistake #6: forgetting the eyelids exist
MGD/blepharitis management is unglamorous. It’s also one of the highest-ROI moves if evaporation is your driver.
Mistake #7: ignoring the room
The fastest win is often environmental: redirect vents, reduce direct airflow, and consider humidity support. I’ve watched a $0 vent adjustment beat a $25 “miracle” purchase.
- Label awareness beats guesswork.
- Airflow management is a cheat code.
- Eye redness isn’t the same as lubrication.
Apply in 60 seconds: Find the vent/fan aimed at your face and redirect it—right now.
Better swaps: allergy control that’s kinder to dry eyes
If you’re time-poor and symptom-rich, you want the simplest plan that works. Here are the alternatives that often help people reduce systemic “drying pressure” while still controlling allergies.
Nasal steroid sprays: why they’re often the dry-eye-friendly backbone
Many ophthalmology and allergy clinicians recommend considering nasal corticosteroid sprays for nasal symptoms, because they target inflammation locally. That can mean fewer “stacked” systemic medications. This is not a DIY directive—just a strong discussion point if you’re struggling.
Local wins: antihistamine eye drops vs oral pills
If your main symptoms are eye itch and redness, local eye drops may control symptoms with less systemic impact. (Still: use as directed, and ask a professional if you’re unsure—especially with contacts.)
Low-tech, high-ROI: saline + barrier methods
- Saline rinse (if appropriate for you) to reduce nasal allergen load.
- Shower after outdoor exposure on heavy pollen days.
- Change pillowcases more often during peak season.
Money Block: Decision card (When A vs B)
- You have full-body allergy symptoms (sneezing/itching/runny nose).
- Eye symptoms are mild and manageable.
- You can keep dosing consistent for 7 days.
- Your eyes dry out noticeably on pills.
- Your main symptoms are nasal or eye-specific.
- You have contacts/LASIK/MGD and a fragile baseline.
Time/cost trade-off: oral is convenient; local strategies can reduce systemic side effects but may take a few days to dial in.
Neutral action: Pick one lane for 7 days so you can evaluate it cleanly.

Switch logic: change meds without confusing the data
Switching meds can help. Switching chaotically can make you feel like nothing helps. The goal is to change one variable at a time so you can answer the real question: Is my dryness medication-driven, environment-driven, or baseline-driven?
The “one variable” rule
- Keep sleep schedule roughly consistent.
- Keep screen schedule as similar as possible.
- Keep drops the same (or none the same).
- Change only the antihistamine (or only the timing).
What improvement should look like
- Less fluctuation in vision (less “blink to clear”).
- Longer comfortable contact lens time.
- Lower “grit score” by evening.
When switching won’t help
If your dryness is dominated by MGD + airflow + heavy screen time, switching brands may feel like tiny gains. That’s not failure. That’s information. It means you’ll get more ROI from treating the stack.
Quick anecdote: I once tried to “fix” dryness by switching brands three times in eight days. The only thing I proved was that I can create chaos faster than pollen can.
7-day A/B test tracker: find your least-drying option
This is the part most competitor articles don’t give you: a practical, low-drama method to find your least-drying option without accidentally changing five things at once.
Setup: keep everything steady, change one thing
- Pick one antihistamine (Claritin or Zyrtec or Allegra) for days 1–7.
- Keep timing consistent (same hour each day).
- Don’t add new drops, masks, supplements, or “miracle hacks” this week.
What to measure (2 minutes/day)
Daily tracker (copy/paste):
- Comfort (0–10): ____
- Blur episodes (count): ____
- Drop use (times/day): ____
- Contacts worn? (Y/N): ____
- Airflow exposure high? (Y/N): ____
If you prefer paper on the fridge (or you want something caregiver-friendly), use a printable symptom diary template and keep the timing consistent.
Decision rule: stay / switch / go local
- Stay: comfort improves by 2+ points and blur episodes drop.
- Switch: comfort worsens by 2+ points for 3 consecutive days.
- Go local: allergy control is okay but dryness persists—ask about nasal sprays or eye drops instead of escalating pills.
Show me the nerdy details
This is essentially an n-of-1 experiment: you’re reducing confounders (environment, sleep, screen load) so the signal (medication effect) is easier to detect. Even a simple 0–10 comfort score can be surprisingly useful when you standardize the timing and the conditions.
Money Block: Mini calculator (2 inputs, 1 output)
Use this to estimate whether your dryness is more likely “environment-driven” than “pill-driven.”
Output: Enter your hours, then press Calculate.
Neutral action: Use this output to decide whether to fix airflow/blinking first or run a tighter medication test.
When to seek help: red flags + what to ask
Dry eye can be miserable, but it shouldn’t be frightening. The moment it becomes scary—pain, vision change, light sensitivity—you stop optimizing and start getting evaluated.
Same-day care
- Significant eye pain
- Marked light sensitivity
- Sudden vision changes
- Thick discharge or a “stuck shut” morning
Within a week (don’t just tough it out)
- Persistent burning + blurred vision despite basic steps
- Contact lens intolerance that appears suddenly
- Symptoms that worsen every day for 5–7 days
What to ask (simple scripts)
- “Do my symptoms look more like allergy eye, dry eye, or both?”
- “Should we try a nasal-first plan so I can reduce oral antihistamines?”
- “Do you suspect MGD/blepharitis, and what’s the simplest routine?”
Personal note: the first time I finally asked, “Is this actually dry eye?” I felt silly—and then relieved. Because once you name the problem, you stop doing random things and start doing the right things.
FAQ
Which antihistamine dries eyes the most: Zyrtec, Claritin, or Allegra?
There isn’t a single “most drying” choice for everyone. Many dry-eye-prone people tolerate Allegra or Claritin better than Zyrtec, but your baseline risk (MGD, contacts, screen time, low humidity) can outweigh the brand. A 7-day A/B test is the cleanest way to find your personal answer.
Does Zyrtec cause dry eyes more than Claritin?
For some people, yes—especially if they end up stacking doses or using multiple products. For others, the difference is minimal. If your eyes worsen reliably after taking it, treat that pattern as data and consider a switch or a more local strategy.
Is Allegra really the least drying antihistamine?
Allegra is often perceived as easier to tolerate by some dry-eye-prone users, but it’s not universally “least drying.” If your dryness is driven by evaporation (MGD, airflow, screens), Allegra may not feel dramatically different until you fix the amplifiers.
Why do my eyes feel dry even when my allergies improve?
Allergy itch can improve while the tear film remains unstable. You can also have reflex tearing (watery eyes) while still having dry eye. That’s why symptom relief in the nose doesn’t always translate to comfort on the eye surface.
Are antihistamine eye drops better than oral pills for dry eye sufferers?
They can be—especially if your main symptoms are eye itch and redness. Local drops target the eyes without as much systemic effect. The safest choice depends on your history (contacts, eye surgery, chronic dry eye), so follow label directions and get guidance if you’re unsure.
Do nasal steroid sprays help allergies without drying out eyes?
For many people with primarily nasal symptoms, a nasal-first plan can reduce the need for oral antihistamines—potentially lowering dryness pressure. Discuss this option with a clinician or pharmacist, especially if you have persistent dry eye.
How long does antihistamine-related dry eye last after stopping?
It varies. Some people feel better within days; others have ongoing symptoms because the main driver is environment, MGD, or screen-related evaporation. If symptoms persist for a week or two after changing strategies, it’s a sign to address dry eye directly.
Can contact lenses make antihistamine-related dry eye worse?
Yes. Contacts can magnify tear film instability and make dryness more noticeable. Shortening wear time temporarily and fixing airflow/blink habits can help while you evaluate medication options.
Close the loop: your 15-minute plan (and why the “most drying” question is tricky)
Here’s the loop we opened at the start: Which one dries eyes most? The honest answer is: the one that hits your tear film at the exact moment your environment and blink habits are already pushing it over the edge. That’s why two people can argue about the same pill online and both be right.
So instead of chasing a universal ranking, you run a short, clean test. You remove the easy amplifiers. You stop dose stacking. You pick a lane for 7 days. You let your eyes vote.
- Fix airflow and blinking first.
- Keep dosing consistent for 7 days.
- Pivot to nasal/local options if dryness persists.
Apply in 60 seconds: Choose your Day-1 plan: (A) keep your current med and fix airflow + blink breaks, or (B) switch once and track for a week.
Your next step (doable in 15 minutes): open your notes app and set up the daily tracker. Then pick one medication plan for the next 7 days. If your eyes flare hard, don’t escalate blindly—consider a nasal-first discussion and targeted dry-eye care. If your trouble clusters at night, consider pairing your allergy plan with a simple 15-minute night routine for dry eyes so your mornings aren’t starting at a deficit.
If you want a trusted baseline explanation of dry eye from major eye-health authorities, these two pages are a solid starting point: Read the official dry eye basics guidance and read the official NIH dry eye overview.
Last reviewed: 2025-12.