


Stop the Two-Week Detour:
Mastering Wet AMD Prior Authorizations
One missing field can turn a routine wet AMD injection into a two-week detour—while everyone insists it’s “still processing.”
If you’re on Medicare Advantage, prior authorization delays for anti-VEGF injections rarely happen because the plan “won’t cover it.” They happen because the request lands as incomplete: the wrong site of care, a mismatch between medical vs pharmacy benefit routing, or identifiers that don’t line up with how your retina clinic bills. And if your plan also uses Medicare Advantage step therapy for wet AMD, the paperwork path can get even more finicky unless everyone is describing the same request in the same language.
Keep guessing and you risk the worst kind of loss: a treatment calendar that collapses into last-minute reschedules and endless phone-tag.
This post gives you a simple, repeatable workflow to prevent that: a one-page PA Proof Pack a reviewer can approve at a glance, a buffer that survives a “needs more info” reset, and scripts that get you a case ID, received date, and completeness status—fast.
It’s built from the same patterns that show up in real patient/caregiver call logs: not drama, just precision that stops the clock from restarting.
- • Here’s the bottleneck.
- • Here’s the fix.
- • Here’s how to keep your request in the right queue.
- • And here’s how to escalate cleanly—only when it’s actually needed.
- Build a one-page Proof Pack the reviewer can approve in one glance.
- Confirm the plan’s exact UM/PA requirements (drug + frequency + site-of-care).
- Use expedited language only when it matches the plan’s standard.
Apply in 60 seconds: Text or message your retina office: “Can you generate a one-page prior-auth Proof Pack for my next anti-VEGF injection?”
Table of Contents
Prior-auth bottleneck: where anti-VEGF requests actually get stuck
The “missing puzzle piece” problem (it’s rarely the whole puzzle)
Here’s the frustrating truth: your plan can be perfectly willing to cover the injection… and still stall the request because one field doesn’t match their internal checklist. I see it most often when a member is told, “It’s pending,” but the plan has quietly marked it as incomplete. Nobody calls it a denial, so nobody treats it like a fire—until your injection date is suddenly next week.
A common pattern from reader notes: the retina office submits clinical documentation, but the plan reviewer is actually looking first for a clean administrative match—right provider identifiers, right location, right requested frequency, right drug descriptor, right billing detail. If even one element is missing or inconsistent, the request can bounce back into “needs more info,” and that clock you thought was ticking… starts over when the missing piece arrives.

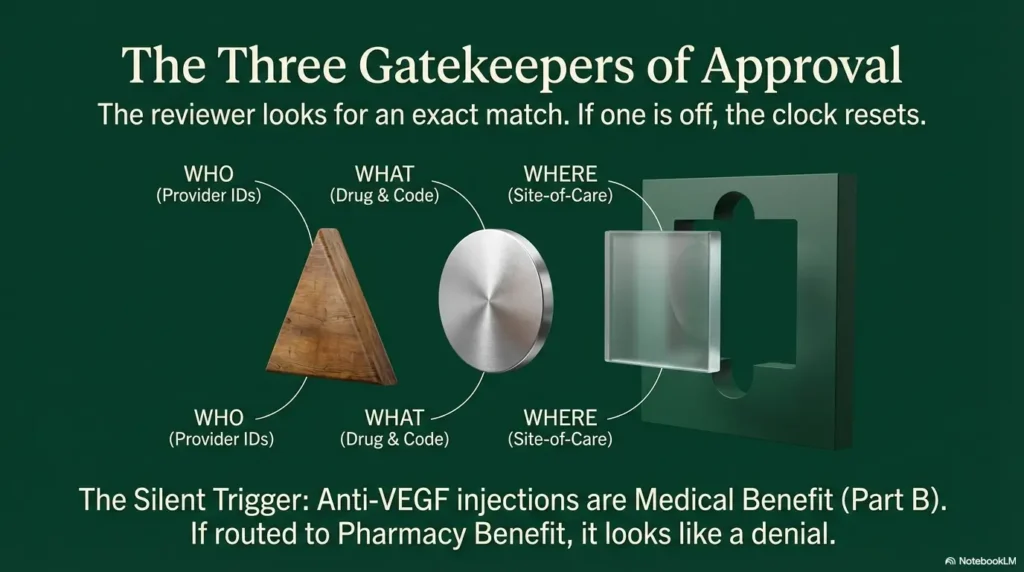
The 3 data points plans check first (and why one mismatch stalls everything)
- Who: ordering clinician and billing entity (NPI and sometimes tax ID), plus whether they’re in-network.
- What: the specific drug request (name + billing code information the plan expects) and that it aligns with the diagnosis submitted.
- Where: site-of-care (retina clinic office vs hospital outpatient) and whether the plan restricts location for that service.
One small story: a reader once copied a prior year approval letter into a new request “to make it easy.” Unfortunately, the new plan year required a different site-of-care field, so the request just sat. The plan wasn’t rejecting treatment—it was rejecting the format.
Open loop: the one code/detail that silently triggers “incomplete” status
It’s usually not the OCT image quality. It’s not even the diagnosis. The silent trigger is often a billing/administration detail—a code, place-of-service indicator, or “buy-and-bill” vs pharmacy channel mismatch.
Many anti-VEGF injections are handled as a Part B drug in a medical setting (not a retail pharmacy pickup), and when the request gets routed to the wrong internal queue, it can look “stuck” even if everyone is acting in good faith. (If you’re new to this world, it helps to read a plain-English primer on what to expect at your first anti-VEGF injection for wet AMD—because the administrative pathway is part of the experience.)
Show me the nerdy details
Plans typically run prior-auth requests through utilization management workflows that rely on structured fields. If the request enters the wrong pathway (medical benefit vs pharmacy benefit), the reviewer may not have authority to approve it, so they mark it “need info” rather than “deny.” This is why a “readable in 30 seconds” one-page pack helps: it makes misrouting obvious and easier to correct.
- Confirm the plan is reviewing it under the correct benefit pathway.
- Make the site-of-care explicit.
- Match the requested frequency to what’s in the chart summary.
Apply in 60 seconds: Ask: “Is this being handled under medical benefit (Part B) or pharmacy benefit?”
Who this is for / not for
For: ongoing injections, new MA enrollment, plan change, or first-time PA
This is for you if you’re a Medicare Advantage member who:
- Gets ongoing anti-VEGF injections and wants fewer last-minute surprises (start with a realistic wet AMD injection schedule so you can protect your buffer).
- Switched plans (or is about to) and worries about a January paperwork jam
- Is newly diagnosed and wants a calm workflow before your schedule fills up
- Has been told “pending,” “in review,” or “needs more information” more than once
Also: if you’re the adult child doing the phone calls between meetings, this guide is for you too. I’ve read enough “I’m at work, my mom’s appointment is Friday, the plan won’t answer” messages to know how fast this spirals. And if home logistics are part of your stress load, bookmark a simple wet AMD home safety checklist—because the goal isn’t just approvals; it’s a life that doesn’t feel like it’s constantly rearranging itself around phone calls.
Not for: medical advice, self-diagnosis, or choosing a drug without your clinician
I won’t tell you which medication you “should” get, how often you “must” be treated, or how to interpret imaging. This is strictly the insurance logistics side: how to reduce avoidable administrative delays while your clinician handles the clinical decisions. For costs and coverage specifics (which vary), you may also want a separate reference on AMD treatment cost and how plans typically structure patient responsibility.
Paperwork that moves: build a one-page “PA Proof Pack”
What to include on one page (so a reviewer can approve fast)
Think of the Proof Pack as a one-page cover sheet that sits on top of whatever your clinic submits. The clinic still sends the full notes; you’re just making sure the reviewer sees the essentials immediately.
- Patient: name, DOB, member ID (as your plan lists it)
- Diagnosis: wet AMD (and laterality if applicable), plus a brief one-line status
- Requested therapy: anti-VEGF intravitreal injection (drug name clearly written)
- Dose & frequency: what is being requested and how often (in plain language)
- Site-of-care: retina clinic office vs hospital outpatient (explicit)
- Provider identifiers: ordering clinician NPI + facility/billing NPI as submitted
- Billing identifiers: the billing code details the office uses (for example, HCPCS/J-code where applicable) and any plan-specific fields
- Clinical snapshot: 2–4 sentences summarizing OCT/visual status and why continued therapy is needed
- Urgency line (if appropriate): short statement about time sensitivity if delay could risk function
Small lived-experience note from the trenches: the “two-NPI problem” is real. Readers often assume the ordering doctor’s NPI is enough, but plans also track the billing entity. If the wrong entity is listed, you can get an “approved” that isn’t usable—or a request that never matches your clinic’s submission.
What to screenshot/save (so you can prove timelines later)
Keep a tiny “evidence folder” on your phone. Nothing fancy. Just:
- The date the office submitted the PA (portal screenshot or message)
- The plan’s reference number / case ID
- Any “incomplete” notice and what they say is missing
- The name/department of the person you spoke with and the time
This isn’t about picking a fight. It’s about preventing the maddening reset: “We don’t see it” / “Can you ask them to resubmit?” If you can calmly say, “It was submitted on Tuesday; the reference number is X,” the conversation changes.
Let’s be honest… the fastest PA is the one that’s readable in 30 seconds
Reviewers are human beings working a queue. A readable one-page Proof Pack reduces friction. And friction is the silent killer of timelines. (If your plan keeps stalling on specific branded products, it can help to separately understand how Medicare coverage for Eylea injections is typically processed—because “coverable” and “properly routed” aren’t the same thing.)
- Yes/No: Does the pack show drug + frequency + site-of-care on one page?
- Yes/No: Does it list both ordering and billing identifiers?
- Yes/No: Does it include the plan’s case ID once you have it?
Apply in 60 seconds: Ask your clinic: “Can you put the requested site-of-care and frequency on the first page?”
Plan rules that surprise people: MA vs Original Medicare logistics
Prior authorization vs formulary vs “medical necessity” (don’t mix them up)
These three get mashed together in phone calls, and that’s how you lose weeks.
- Prior authorization: “We need approval before we cover it.” (Process gate.)
- Formulary/preferred drug: “We cover these products more easily than those.” (Coverage preference.)
- Medical necessity decision: “We approve/deny based on the submitted documentation.” (Clinical review outcome.)
One quick story: a reader heard “It’s on the formulary” and assumed the appointment was safe. But the plan still required prior authorization for that exact administration setting. Formulary answered “is it coverable,” not “is it approved yet.”
If you’ve ever felt whiplash between “covered” and “approved,” you’re not alone—many people only realize the difference after they’ve already started tracking bills (and yes, sometimes it shows up as an eye-exam style “double charge” moment—see why Medicare may charge separately for refraction fees for a familiar example of how categories can split).
Network + site-of-care rules (retina clinic vs hospital outpatient vs ASC)
Medicare Advantage plans can have narrower networks and more explicit site-of-care preferences than Original Medicare. For injections, the friction point is often where the drug is administered and billed. If your retina specialist is in-network but your facility billing is out-of-network (or categorized differently), your request can stall or get partially approved.
Practical tip: when you call the plan, don’t ask, “Is my doctor covered?” Ask, “Is this location covered for this service under my plan?” Then confirm the location is listed the same way your clinic bills it.
Open loop: why two plans can treat the same injection as two different categories
Because “the same injection” can travel two different administrative roads: one plan routes it as a medical-benefit Part B drug request, another routes parts of it through a different utilization management workflow. That’s not you being unlucky—that’s how plan designs differ.
Federal Medicare rules set timeframes and standards for organization determinations and expedited decisions, including circumstances where plans can extend timeframes.
Medicare’s public guidance for Medicare Advantage appeals also outlines common resolution windows (including fast decisions in urgent situations). You don’t have to memorize the law—you just need to know the plan has to play by time rules, and you’re allowed to ask what clock is running.
The clinic-plan handshake: how to align your retina office and your MA plan
Ask these 7 questions before your next injection date is scheduled
Yes, it feels awkward. Do it anyway. These questions prevent “surprise reschedules.”
- Do you (the clinic) need prior authorization for my plan for this injection?
- Which entity submits it—your office or a specialty pharmacy hub?
- Is it processed under medical benefit (Part B) or pharmacy benefit?
- What exact drug and frequency are you submitting? (Make sure it matches your treatment plan.)
- Which site-of-care and billing location are you using?
- When will you submit it relative to my next due date? (Get an actual date.)
- How will I get the reference number/case ID?
I’ve watched readers lose two weeks because they assumed “the office handles it.” Many offices do—beautifully. But plans change, portals glitch, and humans rotate shifts. A single planned check-in prevents a lot of chaos.
(And if you’re piecing this together while also juggling other medical appointments, it can help to keep your admin notes as structured as possible—some readers even pair this with a printable symptom diary for seniors so the timeline and “what changed” details are easy to retrieve when a plan asks.)
The “reference number” habit that prevents lost requests
Make this your default phrase: “Can I get the reference number or case ID?” Say it to the plan. Say it to the clinic. Write it down once. Keep it in your phone notes.
Why it matters: if the plan can’t locate your request quickly, you fall into “Please ask your provider to resubmit.” That’s how time gets erased. A reference number anchors reality.
Here’s what no one tells you… “urgent” only works if you use the plan’s exact wording
Plans typically require a specific standard to treat a request as expedited. In many cases, the expedited path is tied to whether delaying a decision could seriously jeopardize life, health, or the ability to regain maximum function. Your clinician’s support can matter. Your emotions (valid as they are) usually don’t trigger the expedited pathway by themselves.
So don’t say, “This is urgent because I’m scared.” Say, “We’re requesting expedited review because a delay could risk function; my clinician supports the expedited request.” Calm, clear, procedural.
- Gather: plan name + member ID + the clinic’s billing NPI (ask the office).
- Gather: requested drug name + frequency + site-of-care.
- Gather: the plan’s fax/portal route used for UM/PA submissions.
Apply in 60 seconds: Ask the clinic front desk: “What billing NPI are you using for my injection?”
Expedited pathways: when and how to request a faster decision
What “expedited” typically means in Medicare Advantage (in plain English)
“Expedited” is not a magic customer-service override. It’s a formal pathway with a standard. If your clinician indicates that waiting for a standard timeframe could seriously jeopardize health or the ability to regain maximum function, plans generally must treat the request as expedited.
In Medicare Advantage regulations and public guidance, expedited decisions are often described in terms of a short clock (commonly hours to a few days), and plans can only extend deadlines under defined circumstances.
Translation: if you qualify, expedited review is a real tool. If you don’t, pushing “urgent” can backfire by creating confusion instead of speed.
How to document time sensitivity without sounding adversarial
Use a three-part sentence. It’s polite, specific, and hard to ignore:
- Situation: “I’m due for an ongoing course of intravitreal anti-VEGF injections.”
- Risk: “A delay could affect my ability to maintain/regain maximum function.”
- Request: “We’re requesting expedited review; my clinician supports this request.”
A small personal-style note from the inbox: readers who get traction tend to sound boringly procedural. The goal is not to win an argument. It’s to get the request into the correct queue.
Open loop: the timing window that matters more than the submission date
The window that matters is your buffer before the next due date. Submitting “sometime this month” is not a plan. The practical buffer is usually measured in weeks, not days, because “incomplete” fixes can restart the clock. That’s why mapping your next due date against a realistic anti-VEGF injection schedule is more than “planning”—it’s protection.
- Mini calculator: Buffer Days = (Next injection date) − (PA submission date)
- Target: Aim for a buffer that can absorb “incomplete” + resubmission.
- Reality check: If your buffer is under 10 days, treat it as a risk state.
Apply in 60 seconds: Count the days on your phone calendar—if it’s tight, ask the clinic to submit earlier for the next cycle.
Appeals ladder without the headache: a calm, step-by-step escalation map
First response: fix “incomplete” vs fight a “denial” (choose the right move)
Before you go full “appeal,” identify what you’re actually dealing with:
- Incomplete/pending: Usually a missing field, document, or mismatch. Fixable fast.
- Adverse decision/denial: The plan says no (or limits scope/duration). This is where appeal steps apply.
One small moment of humor because we need it: appealing an “incomplete” is like arguing with a printer that’s out of paper. The printer does not need a persuasive essay. It needs… paper.
What to ask for in writing (so you know the real reason)
When you hear “denied,” ask for the precise basis:
- The exact reason (not a category—an actual sentence)
- The policy or coverage criterion they used
- Whether it’s drug-related, documentation-related, or site-of-care related
- Your appeal rights and the deadline
Medicare’s own consumer guidance describes Medicare Advantage coverage decisions as “organization determinations” and outlines timeframes for different types of appeals, including faster decisions in urgent situations. Knowing the vocabulary helps you stay calm—and sound like someone who expects process competence.
When to loop in your prescriber statement (and what it should focus on)
If you’re appealing, the most effective clinician statement is usually not dramatic. It’s targeted:
- Confirms diagnosis and that the therapy is part of an ongoing course
- Explains why the requested frequency matters
- Addresses the plan’s stated reason for denial (not everything under the sun)
- When needed, supports expedited handling using the plan’s standard language
Reader-pattern note: the best statements respond to the plan’s reason code. The worst statements are generic letters that don’t mention what the plan complained about. (If the plan’s issue is really “preferred product first,” the most productive next read is often a clear explanation of how step therapy works for wet AMD on Medicare Advantage, because it changes what “a good appeal” looks like.)
Common mistakes that cause avoidable delays
Mistake 1: waiting until the week of the injection to start prior-auth
This is the most common—and the most forgivable—mistake. You’re busy. You assume the system works. Then you get a call that feels like a trap door opening under your week.
Fix: treat prior authorization as a rolling process. The best time to start the next cycle is right after you finish the current one, when the clinic already has fresh notes.
Mistake 2: assuming “same drug as last year” means “same rules this year”
Plan years reset. Formularies update. UM requirements shift. Provider contracts change. Even if your therapy is unchanged, the paperwork expectations can drift.
A small anecdote from reader emails: someone had approvals all year, switched nothing, and still got stuck in January because the plan required a new form version. Nobody did anything “wrong.” The system just turned over.
Mistake 3: mixing up drug names, strengths, frequency, or administration setting
To a plan, small wording differences can look like two different requests. If your notes say one frequency and the PA says another, that’s a stall risk.
Mistake 4: losing track of who submitted what (patient vs clinic vs plan)
Patients call the plan. Plans tell them to call the clinic. Clinics say they submitted it. Everyone is sincere. Nobody can prove it. That’s why the reference number habit is so powerful—it creates a shared anchor.
Mistake 5: accepting vague answers like “it’s processing” without a reference ID
“Processing” is not a status. It’s a mood. Ask for:
- The case ID
- The date received
- Whether it’s complete
- The deadline for decision under standard vs expedited
Don’t do this: plan switching mid-treatment without a bridge plan
The continuity gap: why the first injection after a switch is the riskiest
If you switch Medicare Advantage plans while you’re in an ongoing injection schedule, your biggest risk isn’t “coverage forever.” It’s the first appointment after the switch. That’s when:
- New plan requires new authorization
- New plan’s network rules get tested for the first time
- New plan’s site-of-care preference shows up uninvited
One reader described it as “my eyes didn’t change, but the bureaucracy did.” Accurate.
How to time enrollment changes around ongoing treatment
If you have flexibility, aim to avoid a plan change that forces your first post-switch injection into the earliest weeks of the new plan year without preparation. The tactical move is to start your Proof Pack and new-plan UM confirmation before the switch becomes active.
What to confirm during open enrollment (so January doesn’t become a paperwork month)
- Is your retina specialist in-network under the new plan?
- Is the clinic’s billing entity in-network?
- Does the plan require prior authorization for your anti-VEGF injection?
- Any site-of-care restrictions?
- Is step therapy used for this category?
- When A wins: Stay put if your current plan is consistently on-time and your clinic is stable in-network.
- When B wins: Switch if your current plan repeatedly delays or restricts site-of-care—even after you fix completeness issues.
- Trade-off: Lower premiums can come with tighter UM/PA friction; factor in time cost.
Apply in 60 seconds: If you’re switching, schedule one call: “Confirm PA requirements for my next injection under the new plan.”
Drug changes and formularies: what happens when the plan pushes a switch
Step therapy, preferred products, and “equivalent” language (what it can mean)
Some Medicare Advantage plans use “preferred” status or step therapy rules that can influence which anti-VEGF products are easiest to approve. If the plan suggests an “equivalent” alternative, your clinician may agree—or may have reasons to stick with the current regimen. Either way, your role is to keep the process clean:
- Ask whether the issue is coverage (formulary/preferred) or authorization (UM requirement).
- Ask what documentation the plan needs for an exception, if applicable.
- Ask whether the plan is restricting by site-of-care rather than drug choice.
Commercial reality check (neutral, not promotional): big MA carriers like UnitedHealthcare, Humana, Aetna, Blue Cross Blue Shield-affiliated plans, and Kaiser Permanente can differ in UM workflows even when the therapy category is similar. Your best defense is not guessing—it’s confirming the plan’s written requirement for your plan ID.
Biosimilars and brand changes: what to ask your clinician and plan
If a plan pushes a switch, you don’t need to debate pharmacology on a call. You need to ask two clean questions:
- Plan: “Is the current drug non-preferred, or is this a prior-auth requirement issue?”
- Clinic: “If the plan requires a preferred product first, what documentation supports staying on the current regimen?”
A small anecdote from a caregiver: they kept arguing “but it works!” while the plan kept repeating “preferred.” Once they asked “what exception documentation do you require,” the call turned into a checklist. That’s the pivot.
Open loop: the hidden tradeoff between “preferred” and “available on time”
Even when a preferred option is theoretically easier, availability and coordination can still cause timing problems. Your mission is continuity: keep the schedule intact and keep approvals aligned with that schedule.
- Tier 1: In-network clinic + plan’s preferred workflow + complete PA pack
- Tier 3: Drug or location mismatch triggers manual review
- Tier 5: Denial/limitation requires appeal or exception process
Apply in 60 seconds: Ask the plan: “Is this request delayed because of drug preference or site-of-care?”
FAQ
Does Medicare Advantage require prior authorization for anti-VEGF injections?
It depends on the plan. Many Medicare Advantage plans use prior authorization for certain Part B drugs and administration settings, while others may not require it in the same way. The practical move is to confirm your plan’s UM/PA requirement for your specific drug, frequency, and site-of-care—and to ask how the request should be submitted (medical vs pharmacy pathway).
How long does prior authorization take for wet AMD injections?
Timeframes vary by plan and by whether the request is standard or expedited. Medicare’s public guidance and regulations describe defined decision windows and limited circumstances for extensions, but the day-to-day reality is that “incomplete” submissions can reset timelines. That’s why building a one-page Proof Pack and securing a reference number matters: it reduces the chance of a silent reset.
Can I get an expedited prior authorization if delaying treatment risks my vision?
Plans typically treat a request as expedited when waiting for the standard timeframe could seriously jeopardize health or the ability to regain maximum function—often with clinician support. If your retina specialist supports expedited review, ask the clinic to state that clearly using the plan’s standard language, and confirm with the plan that the request is in the expedited queue.
What documents does my retina specialist need to submit for a PA?
Plans commonly want a concise clinical rationale (often including a brief summary of imaging/visual status), the requested drug and dosing/frequency, site-of-care, and provider identifiers—plus any plan-specific fields. Your “PA Proof Pack” is a one-page cover sheet that makes these elements easy to see, even when the full notes are longer.
What if my MA plan says the request is “incomplete”?
Ask what exact element is missing and whether the plan can list it as a checklist item (for example: missing site-of-care, mismatch in frequency, missing provider identifier, or missing supporting documentation). Then have the clinic resubmit the missing piece and ask the plan to confirm the request is now “complete” with the same reference number (or a new one, if they require it).
What if the plan approves the drug but not the injection location (site of care)?
This can happen. Ask whether the plan requires a different site-of-care (for example, office-based vs hospital outpatient) and what criteria they used. Then coordinate with the clinic to align the billing location and authorization. If the site restriction is not workable, ask what appeal or exception pathway applies and what documentation would support it.
If I switch Medicare Advantage plans, do I need a new prior authorization?
Often, yes. A new plan may require a new authorization even if treatment is ongoing. The highest-risk moment is the first injection after the switch. Reduce risk by confirming UM/PA requirements before the switch takes effect and having the clinic submit early with a fresh Proof Pack.
Is Avastin covered under Medicare Advantage for wet AMD?
Coverage varies by plan, and policies may differ around preferred products, step therapy, and how the medication is billed and administered. If your clinician recommends a specific therapy, focus your calls on whether the plan treats it under medical benefit vs pharmacy benefit and what documentation is required for approval or an exception.
What’s the difference between a formulary denial and a medical-necessity denial?
A formulary issue is about whether the plan prefers or covers a product under its coverage rules. A medical-necessity issue is about whether the plan believes the submitted documentation supports the request. They require different fixes: formulary issues often involve exceptions/step therapy documentation, while medical-necessity issues often require targeted clinical support addressing the plan’s stated reason.

Next step: a 15-minute “no-delay” checklist you can do today
This is the part you can do between coffee and your next obligation. No spreadsheets. No heroics.
- Call your plan’s UM/PA line and ask: “For my next anti-VEGF intravitreal injection, do you require prior authorization? Is it handled under medical benefit (Part B) or pharmacy benefit?”
- Confirm site-of-care rules: “Is the retina clinic office location covered for this service under my plan?”
- Ask for the plan’s submission requirements: “What fields must be included for a complete request (drug, frequency, billing details, provider identifiers)?”
- Message your retina office: “Please generate a one-page PA Proof Pack (diagnosis summary, drug, dose/frequency, site-of-care, billing identifiers) and submit it early.”
- Get the reference number once submitted. Put it in your phone notes with the date and who you spoke with.
One page: drug + frequency + site-of-care + identifiers
Buffer enough to survive one “incomplete” reset
Medical vs pharmacy pathway; site-of-care confirmed
Reference number + received date + completeness status
Fix incomplete fast; appeal denials with targeted clinician support
Short Story: A reader once told me their plan “kept losing” the prior auth. They weren’t exaggerating—it just looked that way. The clinic submitted through the portal, but the plan’s phone reps searched by the ordering physician’s name while the submission was tied to the billing entity. Every call ended with “we don’t see it,” and each resubmission restarted the waiting game.
When they finally asked for two specifics—(1) “What name is the request filed under?” and (2) “What’s the case ID?”—the entire situation snapped into focus. The plan found it in minutes. The request wasn’t lost; it was filed under a different identifier. Their injection wasn’t delayed because the system hated them. It was delayed because the system needed one unglamorous piece of precision. They fixed it once, and the next cycle went smoothly.
Near the end of 2025 and into 2026, Medicare Advantage oversight has continued to emphasize transparency around prior authorization. Federal rules also require plans to publicly post certain prior authorization information and report metrics starting in 2026—use that cultural pressure to your advantage: you’re not asking for special treatment, you’re asking for a clear process.
Conclusion
Remember the open loop from the beginning—the “one missing piece” that stalls everything? It’s usually not a mystery clinical detail. It’s the unglamorous trio: drug + frequency + site-of-care presented in the plan’s required format, tied to the right identifiers. Once you treat prior auth like a small operations problem—not a personal failure—you get your power back.
Your next best move is simple: build the one-page Proof Pack, confirm the plan’s UM requirements for your specific setup, and protect your schedule with a buffer that can survive one reset. If you do nothing else, do this in the next 15 minutes: message your retina office for the Proof Pack and call your plan to confirm whether the request is handled under medical benefit (Part B) or pharmacy benefit.
That one clarification prevents an astonishing number of delays. And if you’re also trying to plan for the “what else is going to show up on my statement” side of eye care, it can be grounding to understand how Medicare treats adjacent categories like surgery billing and eyewear rules—start with cataract surgery and Medicare Part B coverage basics as a familiar parallel where “covered” still has process gates.
Last reviewed: 2026-01-15