


Navigating Life Beyond the Blur
A low vision occupational therapy appointment can go strangely vague if you walk in with only one sentence: “I’m having trouble seeing.” The more useful story is hiding in ordinary places: the pill bottle at 8 p.m., the shower shelf in glare, the stove dial that suddenly feels less trustworthy.
When low vision starts changing daily life, the problem is rarely just “small print.” It is medication labels, lighting, contrast, screens, stairs, cooking, fatigue, and the quiet habit of avoiding tasks that used to feel simple. Keep guessing too long, and small workarounds can turn into missed doses, falls, burns, or unpaid bills.
This guide helps you prepare practical questions for your therapist by focusing on the map of your daily life:
- 📍 Start with the hard moment: Describe the specific task and setting.
- 📸 Bring the messy evidence: Use home photos and problem objects.
- 📋 Ask for a plan: Seek functional strategies, not just a device.
Turn ordinary trouble into your roadmap for independence.
Table of Contents
Safety / Disclaimer
This guide is for appointment preparation and everyday function planning. It does not replace advice from an eye doctor, occupational therapist, low vision specialist, pharmacist, primary care clinician, or emergency service.
Low vision can be connected to macular degeneration, glaucoma, diabetic eye disease, stroke, medication effects, neurological changes, or other conditions. Some changes are slow and frustrating. Others are urgent.
Get urgent medical help for sudden vision loss, new eye pain, sudden flashes or floaters, new loss of side vision, new weakness, facial drooping, confusion, severe headache, repeated falls, or a sudden change in speech or balance. If you are unsure whether a change is ordinary aging or something more serious, review these senior vision changes warning signs and contact a clinician promptly.
- Use OT for daily-life adaptation and safety planning.
- Use eye care for diagnosis, disease monitoring, and treatment.
- Use urgent care or emergency services when symptoms are sudden or severe.
Apply in 60 seconds: Write down one symptom that would make you call for urgent help, so the whole household knows the line.
Start Here: Your Best Questions Begin With “Where Does Life Get Hard?”
The Appointment Is Not a Vision Trivia Test
Many people arrive worried they will be quizzed on eye words they barely remember from the last appointment. Acuity. Field loss. Contrast sensitivity. Central vision. Peripheral vision. The terms matter, yes, but they are not the front door.
The front door is simpler: Where does life get hard?
That might sound like, “I miss the stove dial,” “I cannot read pill labels,” “I avoid the shower,” “I keep putting bills in a pile because I cannot sort them,” or “I trip near the bedroom rug when the hallway light is off.” These are not small complaints. They are the breadcrumbs your OT needs.
I once watched someone spend five minutes trying to describe glare. Then they pulled out their phone and showed a photo of the kitchen counter at sunset. The whole problem appeared instantly: white counter, shiny toaster, tiny black knob, sunlight bouncing around like an overexcited mirror.
Bring the Ordinary Trouble
Low vision occupational therapy is practical. It is about reading mail, cooking safely, managing money, using a phone, walking through rooms, getting dressed, finding objects, and finishing self-care without turning the day into an obstacle course.
Your best questions will not be dramatic. They will be plain. Plain is powerful.
- “Why do I spill more when I pour coffee now?”
- “How can I tell shampoo from conditioner?”
- “What lighting helps bills but does not create glare?”
- “Why do stairs feel worse at night?”
- “What should I stop forcing myself to do visually?”
The Tiny Log That Changes Everything
For 3 days before the appointment, keep a tiny vision friction log. It can live on paper, in your phone, or in a voice memo. No calligraphy required. This is not a school assignment. It is a field report from the kitchen table.
| Task | Time | Lighting | What went wrong? | What did I try? |
|---|---|---|---|---|
| Reading pill bottle | 8 p.m. | Dim lamp | Could not tell two bottles apart | Used phone flashlight |
| Shower | Morning | Glare from window | Could not see soap on shelf | Skipped washing hair |
Money Block: Eligibility checklist
You are probably ready to ask about low vision OT if you answer yes to 2 or more:
- Yes / No: Glasses do not fully solve reading, cooking, or home safety.
- Yes / No: You avoid at least one daily task because seeing it feels unreliable.
- Yes / No: Lighting, glare, contrast, or shadows change your confidence.
- Yes / No: Medication labels, bills, phone screens, or appliances cause mistakes.
- Yes / No: A caregiver has noticed skipped tasks, near-falls, or new hesitation.
Neutral action: Bring this checklist to your eye doctor, OT, or rehab intake call and ask what referral path fits your situation.
Who This Is For, and Who It Is Not For
This Is For People Who Can Still Do Some Tasks, But Not Reliably
This guide is for people who are not fully blind but are finding daily life less predictable. Maybe print fades into gray soup. Maybe glare turns the kitchen into a snowfield. Maybe side vision loss makes doorframes feel newly rude.
Low vision can involve contrast, glare, print size, depth perception, side vision, visual fatigue, or trouble finding objects against busy backgrounds. A person may still read some words, cook some meals, and walk through familiar rooms, but the reliability has changed.
That “not reliably” part matters. It is where safety lives.
This Is For Caregivers Who Hear “I’m Fine” But See Avoidance
Caregivers often notice the plot twist before the person names it. The mail pile grows. The refrigerator has expired food. The phone goes unanswered because the screen is hard to use. The shower becomes “later.” Errands shrink. The person says, “I’m fine,” while quietly building a smaller life.
That does not mean the caregiver should storm in with a clipboard and become the household sheriff. Please do not become the sheriff. The badge is imaginary and nobody likes it.
Instead, bring observations gently:
- “I noticed the mail has been harder lately.”
- “You seem less comfortable with the stove at night.”
- “Would it help if we asked about labels and lighting?”
- “I want you to have more control, not less.”
If the appointment involves a spouse or partner, it may help to read about helping a spouse with vision loss before the visit, especially if support has started to feel tense, protective, or uneven.
This Is Not For Replacing an Eye Exam
Occupational therapy does not replace eye disease diagnosis or treatment. Eye doctors evaluate what is happening medically. Occupational therapists help translate vision changes into safer routines, home setup, tools, and practice.
The two roles should work together. Think of it this way: the eye doctor studies the instrument; the OT helps you play the music of daily life with the instrument you have now.
- Bring eye diagnosis details if you have them.
- Bring daily-life problems even if you do not know the diagnosis terms.
- Ask how OT, eye care, pharmacy, and primary care should coordinate.
Apply in 60 seconds: Write one sentence that starts, “Glasses help, but I still struggle with…”
Ask About Tasks, Not Just Eyes
“Which Daily Activities Should We Prioritize First?”
A good low vision OT visit should not become a foggy tour of every inconvenience in your week. Start with priority. Ask the OT how to rank tasks by danger, frequency, and emotional importance.
Danger comes first. If bathing, stairs, medication, cooking, or night walking feels unsafe, say so early. Frequency comes next. A task that happens 3 times a day can quietly drain more energy than a dramatic task that happens once a month. Emotional importance also counts. Reading a grandchild’s note may not be “essential” on paper, but it may be essential to the person’s heart.
I learned this from a family who thought the biggest issue was bills. The patient cared more about making tea without spilling boiling water. Once the OT helped with the tea station, the whole appointment softened. Safety first, dignity right beside it.
“What Should I Stop Doing the Old Way?”
This is one of the most underrated questions. People often ask, “What can I buy?” Ask this first instead: What should I stop doing the old way?
That might apply to cutting food, reading labels, crossing rooms, pouring liquids, finding clothes, organizing medication, or using the stove. Sometimes the safer change is not a device. It is a new sequence.
- Move the task to better lighting.
- Use contrast before magnification.
- Make frequently used items live in fixed places.
- Reduce visual clutter before adding tools.
- Practice one routine until it becomes automatic.
“What Can I Practice Between Visits?”
Therapy works better when practice is specific. “Use your magnifier more” is vague. “Practice reading 3 medication labels at the kitchen table with the task lamp at 10 a.m.” is useful.
Ask for practice that includes the task, setup, time, and success sign. For example: “Practice sorting mail for 10 minutes using the lamp, black tray, and large-print labels. Stop when the pile is separated into bills, medical, and discard.” If medication routines are part of the plan, a low vision medication tracker printable can give the OT a concrete format to review instead of relying on memory alone.
Show me the nerdy details
Strong OT questions describe performance, context, and outcome. Instead of saying “reading is bad,” describe the object, font size, lighting, glare, body position, time of day, fatigue level, and what mistake happens. This helps the therapist separate visual acuity problems from contrast, glare, scanning, cognition, reach, endurance, or environmental setup.
Bring Proof: Photos, Objects, and Real-Life Clues
A Photo Beats a Vague Memory
Memory gets slippery in appointments. You may remember the bathroom is “kind of dark,” but forget that the bathmat is pale gray on a pale floor, the towel hangs over the grab area, and the shampoo bottles all look like cousins wearing the same outfit.
Bring photos. Not glamorous photos. Functional photos. The kind your phone takes while you mutter, “Why is this hallway so gloomy?” Perfect.
Photograph the bathroom, kitchen counter, stove, medication area, stairs, entryway, favorite chair, reading spot, bedroom path to the bathroom, laundry area, and any place where glare, clutter, or shadows cause trouble.
Appointment Prep Map: Bring the Problem, Not Just the Memory
Bathroom, stairs, stove, medication area, bedside path.
Pill bottles, mail, phone, remote, labels, magnifier.
Morning glare, evening fatigue, shower fear, night walking.
One safety task, one independence task, one meaningful task.
Bring the Actual Problem Items
If the problem item fits in a bag, bring it. Pill bottles, mail, insurance cards, phone, remote control, food labels, sunglasses, current magnifier, favorite book, checkbook, eye-drop bottles, flashlight, or the small object you keep losing on the nightstand.
The OT can learn from how you hold it, where you look first, how much light you need, and whether the issue is print size, contrast, glare, hand steadiness, memory load, or setup.
Let’s Be Honest: The Clinic Room Lies a Little
Clinic rooms are often brighter, cleaner, and less chaotic than real homes. They do not always contain steam, pets, patterned rugs, glossy counters, bad lamps, ringing phones, or the emotional drama of finding the correct pill at 9:47 p.m.
So bring the home into the clinic through photos and objects. Otherwise, everyone is solving a tidy version of the problem. Tidy problems are adorable. Real problems pay the rent.
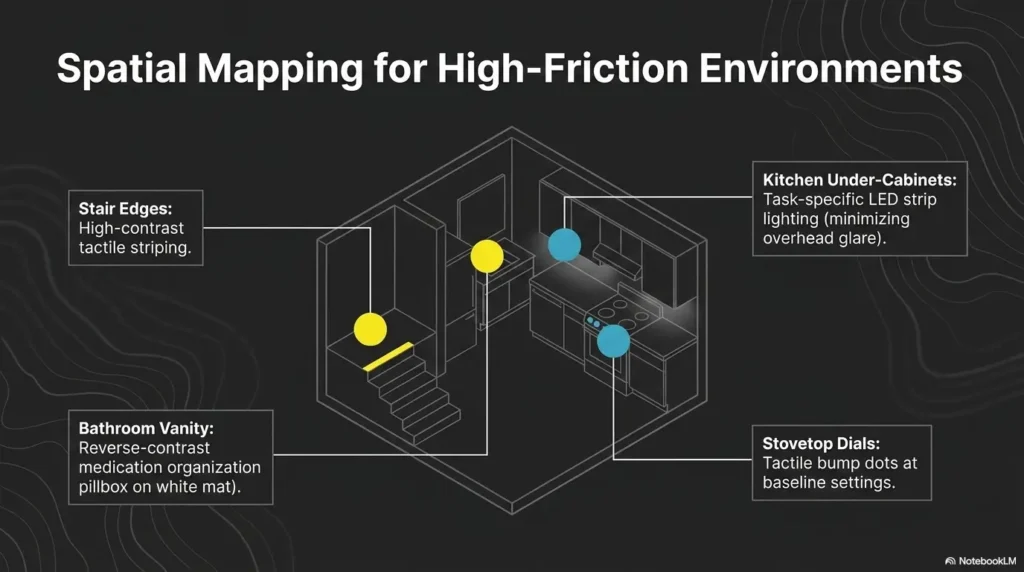
The Home Questions That Prevent Risky Guesswork
“Where Should Lighting Change First?”
Lighting is not just “brighter.” Brighter can help, but it can also create glare, shadows, and visual confusion. Ask the OT where lighting should change first and what kind of lighting fits the task.
For many people, the first lighting wins happen at the medication station, reading chair, kitchen prep area, bathroom path, closet, and bedside table. Small changes in lamp placement can save more frustration than another oversized magnifier tossed into the drawer of noble intentions. For reading areas, ask whether your setup resembles a reading lamp position for central vision loss problem rather than a “not enough magnification” problem.
Ask about:
- Task lighting for reading, cooking, and medication.
- Glare control near windows, counters, mirrors, and screens.
- Contrast between objects and surfaces.
- Nighttime pathway lighting to the bathroom.
- Shadows that hide steps, thresholds, or low furniture.
If nighttime walking is part of the concern, bring up whether a red vs. amber night light would be easier on your eyes than a harsh white light in the hallway or bathroom.
“What Should Be Moved, Labeled, or Simplified?”
Low vision safety often improves when objects stop migrating. Keys, glasses, phone, drops, medication, wallet, water, emergency contacts, remote controls, and magnifiers need fixed homes.
A fixed home is not a decorative basket called “miscellaneous.” That basket is where confidence goes to become compost.
Ask the OT which items should be moved, labeled, simplified, or separated. For example, eye drops may need tactile labels and a stable tray. Cooking tools may need contrast. Bathroom supplies may need fewer bottles and clearer placement. A simple tactile label system for shampoo and conditioner can turn a slippery shower guessing game into a routine the hands recognize first.
“Which Rooms Are Most Dangerous for Me?”
Ask for a safety-first room ranking. The usual suspects are bathroom, bedroom, kitchen, stairs, laundry area, and entryway. The order depends on the person.
One person may be safest in the kitchen but nervous on stairs. Another may walk well but struggle with medication. A third may do fine until evening fatigue pulls a curtain over the room.
Money Block: Coverage tier map
Home support can be discussed in tiers, not all-or-nothing panic:
| Tier | Typical focus | What to ask |
|---|---|---|
| 1 | Lighting and contrast | What is the first low-cost change? |
| 2 | Labels and fixed zones | Which items need tactile or large-print labels? |
| 3 | Task tools | Which tool matches which task? |
| 4 | Safety routines | What should I practice daily? |
| 5 | Caregiver backup | What should be checked without taking over? |
Neutral action: Choose the lowest tier that solves the problem before buying more equipment.
Don’t Do This: Asking Only About Devices
A Magnifier Is Not a Plan
Magnifiers matter. So do lamps, contrast tools, talking devices, large-print labels, phone accessibility settings, and organization systems. But a device by itself is not a plan.
A magnifier sitting in the wrong room, under the wrong light, beside the wrong paper pile, used at the wrong time of day, can become another little object of disappointment. It did not fail because the person failed. It failed because the setup was incomplete.
Ask the OT: “Where would I use this? For how long? Under what lighting? What should success look like?” If hand tremor or fatigue makes handheld tools frustrating, ask whether a stand magnifier for tremor fits the task better than another handheld option.
“Which Device Should I Buy?” Is Too Small a Question
A better question is: Which task am I trying to solve, and what tool or setup fits that task?
Reading a prescription label is different from reading a novel. Identifying a stove dial is different from reading mail. Using a phone is different from signing a check. Each task has its own distance, lighting, contrast, hand position, error risk, and patience budget.
That patience budget matters. A tool that requires 7 tiny steps may be technically clever and emotionally exhausting. The best device is the one a person can actually use on a tired Tuesday.
The Drawer of Abandoned Gadgets
Most families have one drawer where hopeful purchases go to nap forever. It contains magnifiers, odd lamps, talking gadgets, label makers, remote controls, and at least one cable that looks vaguely medical but is probably from a printer.
Before buying, ask the OT to consider vision needs, hand strength, cognition, lighting, daily routine, and caregiver support. A tool should earn its place by solving a specific problem.
- Match tools to real tasks, not vague hope.
- Test lighting and contrast before adding devices.
- Ask how long to practice before judging whether it works.
Apply in 60 seconds: Pick one device you already own and write the task it is supposed to solve.
Ask About Reading, Screens, and Paperwork Separately
“What Is the Best Setup for Mail and Bills?”
Mail is not one task. It is a tiny bureaucracy parade. There are envelopes, due dates, insurance notices, medical forms, small print, glossy inserts, low contrast, and the occasional letter that looks important but is mostly trying to sell you something.
Ask the OT how to create a mail station. This may include a task lamp, dark writing surface, document stand, large-print labels, sorting trays, bold pens, a discard container, and a rule for when to ask for help.
The goal is not to read every word visually. The goal is to know what needs action, what needs storage, and what can leave the house before it forms a paper mountain. If glossy envelopes or shiny inserts are especially hard, bring one and ask about ways to read glossy mail without glare.
“How Should I Adjust My Phone or Tablet?”
Phones can be lifelines or tiny glowing tyrants. Ask about accessibility settings before buying a new device. Larger text, magnification, voice features, high contrast, screen brightness, shortcut setup, voice assistant tools, and simplified home screens can make a real difference.
Bring the actual phone or tablet. Bring the charger too. Appointments have an uncanny way of draining batteries at the exact moment you need to show the problem.
Ask the OT to watch you perform 2 or 3 tasks:
- Call a family member.
- Read a text message.
- Use the camera as a magnifier.
- Set a medication reminder.
- Find emergency contacts.
For phone-based magnification, you can ask whether an iPhone Back Tap Magnifier shortcut would make it easier to open the tool quickly when labels, receipts, or appointment papers suddenly become tiny.
“What Should I Stop Trying to Read Visually?”
This question can feel emotional. Reading is identity for many people. But adaptation is not surrender. Sometimes the safer, smarter option is audio, voice assistant tools, large-print labels, electronic magnification, caregiver backup, or a redesigned routine.
Ask which tasks should move away from visual strain. Medication instructions, financial forms, transportation details, and medical appointment instructions may deserve backup systems, especially when mistakes have real consequences. For long inserts and pharmacy paperwork, ask whether the plan should include ways to read medicine leaflets with low vision without turning every refill into an exhausting decoding session.
Money Block: Mini calculator
Paperwork burden check
Use this simple estimate before your visit:
- How many times per week do you avoid mail, bills, forms, or labels?
- How many minutes does each attempt usually take?
- How many times per week do you need someone else to re-check it?
Output: If the total is more than 60 minutes per week or causes one missed bill, medication concern, or appointment confusion, make paperwork a top-3 therapy goal.
Neutral action: Bring 3 real paper items to the appointment instead of describing the whole pile.
Ask About Movement Before a Fall Forces the Conversation
“Where Am I Most Likely to Trip or Misjudge Distance?”
Low vision is not only about reading. It can change how safe a person feels moving through space. Thresholds, rugs, stairs, low furniture, pets, shiny floors, uneven lighting, and bathroom transitions can all become harder to judge.
The CDC states that more than 1 in 4 older adults report falling each year, and falling once doubles the chance of falling again. That does not mean fear should run the house. It means fall risk deserves a calm, specific conversation before a crisis writes the agenda.
Ask the OT where you are most likely to trip, hesitate, bump, overreach, or misjudge distance. You can also ask whether your home needs a broader aging vision fall prevention at home review, especially if glare, stairs, rugs, or nighttime bathroom trips are becoming part of the same risk pattern.
“Should I Be Evaluated for Mobility Support?”
Keep the wording careful and open. The OT may recommend strategies, home changes, contrast improvements, lighting adjustments, practice routines, or referral to another professional depending on scope and need.
Do not assume the answer is automatically a cane, walker, or dramatic equipment parade. Sometimes the first answer is better lighting on the stair edge. Sometimes it is removing a rug. Sometimes it is changing how the person turns in the bathroom. Sometimes it is a referral.
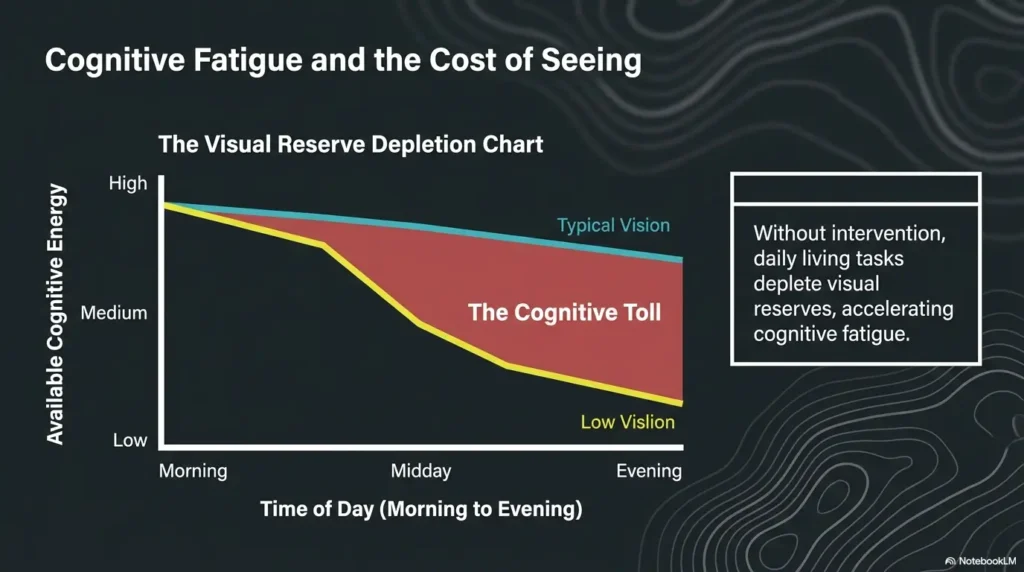
Here’s What No One Tells You: Fatigue Has Footsteps
Low vision fatigue can change movement. A person may walk more slowly, lean forward, avoid stairs, misjudge a shadow, or stop scanning carefully when tired. The body begins negotiating with the eyes, and not all negotiations are safe.
Ask whether your walking confidence changes by time of day. Morning glare, afternoon fatigue, cloudy weather, and nighttime darkness may each create a different version of the same home. If the riskiest route is the bedroom-to-bathroom path, bring up low vision nighttime bathroom safety as its own therapy topic rather than hiding it inside a general “walking is harder” complaint.
Quiet truth: A near-fall is not “nothing happened.” It is useful data arriving before the bill comes due.
Medication, Eye Drops, and Labels Need Their Own Question List
“How Can I Tell Bottles Apart Safely?”
Medication is a high-stakes visual task. Tiny print, similar bottles, white labels, glare, refill changes, and new prescriptions can create confusion even for careful people.
Ask about tactile labels, color contrast, large-print systems, talking labels, storage zones, pill organizers, and separating look-alike containers. Ask the pharmacist what label options are available too. Many pharmacy teams can discuss larger print, medication synchronization, or packaging options, depending on location and service. If you freeze when trying to explain the problem at the counter, bring a low vision pharmacy help script so the request comes out clearly.
Eye drops deserve special attention because bottle shapes, cap colors, timing, and storage instructions can be easy to mix up. Bring the bottles. Do not just bring the names. Names are useful. Bottles are evidence.
“What Is My Backup Check?”
Ask for a double-check system for high-risk moments: morning doses, evening doses, new prescriptions, refill changes, and eye-drop timing. The system should be simple enough to work when tired.
Examples include a marked tray, a large-print schedule, a tactile dot on one bottle, a phone reminder, a caregiver check-in, or a pharmacist-prepared medication list. The best system is boring. Boring is underrated. Boring keeps Tuesday from becoming a medical detective story.
If bottle confusion is already happening, ask whether pill bottle tactile label placement would help you separate “recognize by touch” from “guess by color,” especially in dim light or during evening fatigue.
“What Should My Caregiver Check Without Taking Over?”
Caregiver support should preserve dignity. Ask what a caregiver should check without swallowing the whole room. Helpful checks may include refill dates, label clarity, drop schedule, lighting, and whether the person can identify each item consistently.
Try this wording: “I want to stay in charge, but I want a backup for the parts where mistakes matter.” That sentence has both backbone and grace.
- Bring real bottles to the appointment.
- Ask about tactile, large-print, and storage systems.
- Create a backup check for new or changed prescriptions.
Apply in 60 seconds: Put all current eye drops and medication bottles in one bag or tray for review.
Common Mistakes That Make the Visit Less Useful
Mistake 1: Saying “Everything Is Hard”
“Everything is hard” is emotionally true, but clinically blurry. Replace it with 3 concrete examples. The OT can work with “I cannot read the microwave buttons,” “I confuse two eye drops,” and “I avoid the shower when I am tired.”
Concrete examples turn frustration into a work order.
Mistake 2: Hiding the Embarrassing Problems
People hide bathroom fear, spills, missed medication, unpaid bills, food prep anxiety, and avoiding visitors because they feel embarrassed. But hidden problems cannot be redesigned.
I have seen families spend 20 minutes discussing magnifiers while the real problem was fear of stepping out of the tub. Once someone finally said it, the appointment became useful. Awkward honesty opened the correct door.
Mistake 3: Forgetting Time of Day
Low vision problems change with the clock. Morning glare, afternoon fatigue, cloudy weather, sunset shadows, and nighttime darkness may create different risks. Mention time of day every time you describe a problem.
“I struggle with stairs” is useful. “I struggle with the basement stairs after dinner when the overhead light creates shadows” is much better.
Mistake 4: Letting the Caregiver Answer Everything
Caregivers can add crucial observations, but the person with low vision should describe what matters most. A good caregiver adds context without taking the microphone and turning the visit into a one-person podcast.
Try a simple rhythm: the person with low vision answers first, then the caregiver adds one observation. That keeps the appointment respectful and accurate.
Money Block: Quote-prep list for comparing services or support options
If you are comparing low vision rehab programs, home safety evaluations, transportation support, or private-pay add-ons, gather:
- Eye diagnosis and most recent eye care summary, if available.
- Insurance information and referral requirements.
- Top 3 daily tasks you want improved.
- Photos of risky rooms or work areas.
- Current devices, magnifiers, labels, and lighting tools.
Neutral action: Ask each provider what evaluation includes, what follow-up looks like, and whether home-based recommendations are part of the process.
Build Your Appointment Question Card
The 5-Question Core
This is the printable-style heart of the plan. Put these 5 questions on one page, in large print if needed. Bring two copies if a caregiver is attending.
- Which daily task should we fix first?
- What part of my home setup is making this harder?
- What tool, lighting change, or routine should I try?
- How will I know if it is working?
- What should I practice before the next visit?
Notice what these questions do. They move the visit away from vague worry and toward action. They also prevent the common trap of leaving with a product name but no practice plan.
The “Hard Moment” Add-On
Complete this sentence before the appointment:
The hardest moment of my day is __________________ because __________________.
Examples:
- The hardest moment of my day is taking evening medication because two bottles look alike.
- The hardest moment of my day is getting out of the shower because the floor and mat blend together.
- The hardest moment of my day is opening mail because I cannot tell what is urgent.
The “Safety First” Add-On
Complete this one too:
I feel least safe when __________________.
This sentence often reveals the most important therapy goal. It might be stairs, night walking, cooking, bathing, eye drops, or finding the phone during an emergency.
Short Story: The Question That Finally Worked
Short Story: A daughter once came to an appointment with a neat list of devices her father might need. Magnifier, brighter lamp, talking watch, bigger remote. Her father sat quietly, polite but distant. Then the OT asked, “What part of the day do you dread?” He paused and said, “When the kettle whistles.” Everyone expected bills or reading. But the kettle meant heat, steam, a pale mug on a pale counter, and fear of spilling boiling water.
The visit changed direction. They moved the tea setup, added contrast, simplified the counter, and practiced pouring with a safer routine. The daughter still bought a few tools later, but the first win was not a gadget. It was asking the question that made ordinary fear visible. If hot drinks are part of your own hard moment, bring up low vision kettle safety as a specific therapy goal instead of treating it like a minor kitchen annoyance.
- Use 5 core questions.
- Add one hard moment sentence.
- Add one safety sentence.
Apply in 60 seconds: Copy the 5 questions into your phone notes or print them in large text.
When to Seek Help Sooner
Sudden Vision Changes Are Not an OT Scheduling Problem
Do not wait for an OT appointment if symptoms are sudden or severe. Sudden vision loss, new eye pain, sudden flashes or floaters, sudden loss of side vision, new weakness, confusion, facial drooping, speech trouble, or severe headache should be treated as urgent.
Occupational therapy is valuable, but it is not the emergency door. Use the right door.
Falls, Burns, and Medication Errors Raise the Stakes
Contact a clinician promptly if low vision contributes to falls, near-falls, cooking injuries, burns, missed medication, double dosing, inability to bathe safely, or inability to complete essential self-care.
These events are not personal failures. They are system warnings. A smoke alarm is annoying, but we do not criticize it for being dramatic. We check the kitchen.
Caregiver Concern Counts
If family notices rapid decline, unsafe driving, unopened bills, spoiled food, repeated confusion, or new avoidance of daily tasks, that concern deserves timely professional attention.
The American Occupational Therapy Association has published resources and professional guidance on low vision rehabilitation, and many vision rehabilitation teams include OTs, eye care professionals, orientation and mobility specialists, and other support roles. Ask your clinician what team model is available in your area.
FAQ
What should I bring to a low vision occupational therapy appointment?
Bring your glasses, current magnifiers, medication list, eye-drop bottles, phone, examples of hard-to-read items, photos of problem areas at home, and a short list of daily tasks you want to improve. If possible, bring 3 specific examples instead of saying “everything is hard.” A one-page medication list template can also help you organize prescriptions, eye drops, timing, and refill questions before the visit.
What questions should I ask an occupational therapist for low vision?
Ask which daily tasks to prioritize, what home changes would help, whether lighting or contrast is the bigger issue, what tools are worth trying, and what you should practice before the next visit. The most useful questions connect directly to daily routines.
Can occupational therapy help if glasses do not fix my vision?
Yes. Low vision rehabilitation often focuses on function, safety, task adaptation, lighting, contrast, assistive tools, and independence when regular glasses or medical treatment do not fully restore vision. The National Eye Institute notes that vision rehabilitation can help people with daily activities and doing things they love.
Should my caregiver come to the appointment?
A caregiver can be helpful, especially if they notice home safety issues, medication confusion, falls, or avoided tasks. The person with low vision should still have space to describe their own goals first. A useful rhythm is patient first, caregiver second.
What home photos should I show the OT?
Useful photos include the bathroom, stairs, kitchen counter, stove, medication area, bedside table, hallway, entryway, favorite reading chair, laundry area, and any place where glare, clutter, or shadows cause problems.
What if I feel embarrassed about needing help?
Embarrassment is common, but hiding problems makes the appointment less useful. The OT needs real examples, not a polished performance. The goal is safer independence, not judgment. The awkward detail may be the key that unlocks the best solution.
How do I know if a low vision tool is worth buying?
Ask the OT to connect any tool to a specific task, setting, and practice plan. A device is only useful if it fits your vision, hands, lighting, routine, and actual home environment. Buy the solution to a named problem, not the prettiest gadget on the shelf.
What should I do after the first appointment?
Test the recommended changes in one or two daily routines, track what improves or still feels unsafe, and bring those notes to the next visit. Do not try to overhaul the whole house in one weekend. That path leads to clutter, fatigue, and one mysterious bag of labels nobody can find.
Next Step: Make a One-Page Question Sheet Today
Write 3 Hard Tasks
Choose one safety task, one independence task, and one emotionally important task. This keeps the appointment balanced. Safety matters, but so does the thing that makes a person feel like themselves.
- Safety task: Showering, stairs, cooking, medication, night walking.
- Independence task: Mail, phone use, dressing, food labels, transportation planning.
- Meaningful task: Reading, hobbies, calling family, attending worship, cooking a favorite meal.
Add 3 Home Clues
For each hard task, add where it happens, what time it happens, and what lighting is present. These three details turn a vague concern into a solvable pattern.
Example: “Medication is hardest at the kitchen counter after dinner under the overhead light because the labels reflect glare.” That sentence is a tiny lantern. It shows the OT where to start.
Bring It, Even If It Feels Messy
The best question sheet is not elegant. It is honest. It turns the appointment from a guessing game into a map.
And that closes the loop from the beginning: you do not need perfect terminology. You need ordinary trouble, written plainly enough that someone can help you redesign it.
- Write 3 hard tasks.
- Add time, place, and lighting clues.
- Bring photos or objects that prove the problem.
Apply in 60 seconds: Start with this sentence: “The task I avoid most is ___ because ___.”
Last reviewed: 2026-04.
Your next step is small enough to do before the kettle boils: write one safety task, one independence task, and one meaningful task on a single page. Bring that page to the appointment. It may look ordinary, but for the right therapist, it is a treasure map with coffee stains.