
Beyond the Hallway Blur
You know the feeling: one hand on the appointment papers, one hand on the door, and a dozen instructions already beginning to blur.
This note-taking system isn’t about a beautiful notebook—it’s about protecting memory, dignity, and medication safety. We translate fast-paced medical conversations into safe, actionable steps at home, ensuring the patient’s voice is never lost in the rush.
Table of Contents
Fast Answer: A doctor appointment note-taking system for a caregiver and low vision patient should capture four things: the patient’s main concern, medication and symptom changes, the doctor’s instructions, and the next action after the visit. The best system is large-print, repeatable, shared, and easy to review aloud so the patient remains included instead of being quietly managed.

Start Here: The Appointment Is Not the System
The appointment is only the middle of the story. The system is what happens before the visit, during the visit, and after the car door closes.
Most families discover this the awkward way. The doctor explains something clearly. Everyone nods. The visit ends. Then, 40 minutes later, someone asks, “Were we supposed to stop the old eye drop or add the new one?” That sentence can make a kitchen feel suddenly very large.
Why the real risk happens after everyone leaves the clinic
Inside the exam room, there are professionals, screens, labels, and people who can clarify. After the visit, the patient and caregiver are back in real life: dim hallways, pill bottles, transportation stress, portal passwords, dinner cooling on the stove, and one instruction sheet printed in ant-sized type.
For a low vision patient, this after-visit gap matters. The National Eye Institute explains that low vision can make everyday activities such as reading, recognizing faces, driving, and seeing screens difficult even when some vision remains. That means the written note is not a decoration. It is part of the care environment.
The three-note problem: patient memory, caregiver memory, and portal instructions
There are often three versions of the visit floating around:
- The patient’s memory of what mattered emotionally.
- The caregiver’s memory of tasks, dates, and warnings.
- The official after-visit summary or patient portal note.
None of these is automatically wrong. The trouble starts when they are not brought together. A patient may remember, “The doctor seemed worried about dizziness.” A caregiver may remember, “We need to call the pharmacy.” The portal may say, “Follow up in 4 weeks.” The system makes those pieces sit at the same table.
Build one repeatable page, not a heroic notebook
A heroic notebook sounds noble until it disappears under insurance envelopes and old grocery lists. A repeatable one-page visit sheet is more humble. It has the same headings every time. It fits in a folder. It can be read aloud. It does not require an app update, a perfect pen, or a personality transplant.
- Use one page per visit.
- Keep the same four sections each time.
- Review the note aloud before acting on instructions.
Apply in 60 seconds: Write four labels on a blank page: Reason, Changes, Instructions, Next Actions.
Who This Is For, and Who It Is Not For
This system is for real households, not brochure households. It assumes someone may be tired. Someone may be worried. Someone may be pretending they heard everything because asking again feels embarrassing.
I once watched a caregiver unfold three pieces of paper, two appointment cards, and a pharmacy receipt from one coat pocket. It was not disorganization. It was love under pressure. Love deserves a better container.
Best fit: caregivers helping with vision loss, complex visits, or multiple providers
This system works especially well when the patient has low vision plus one or more of these complications:
- Multiple medications, eye drops, or supplements.
- Several doctors or specialists.
- Recent falls, dizziness, pain, confusion, or fatigue.
- New tests, referrals, surgery discussions, or home care changes.
- Adult children helping from another city.
The more moving parts there are, the less you can rely on “we’ll remember.” Memory is not a filing cabinet. On a stressful day, it is more like a shopping bag with a hole in one corner.
Also useful for spouses, adult children, home aides, and distance caregivers
A spouse may use it to keep both people calm. An adult child may use it to send a clear summary to siblings. A home health aide may use it to report practical changes. A distance caregiver may ask for a photo of the completed sheet after each visit.
Not enough for emergencies, confusion, severe symptoms, or unsafe home situations
A note-taking system is not a substitute for urgent medical care. If there is sudden vision loss, severe eye pain, chest pain, trouble breathing, new weakness, severe confusion, signs of stroke, a serious fall, or an unsafe home situation, the next step is not “improve the binder.” The next step is getting appropriate medical help.
When the patient should lead and the caregiver should simply support
Low vision does not erase adulthood. The patient should lead whenever possible. The caregiver’s role is to support access, accuracy, and follow-through, not to become the main character by accident. For spouses and partners, that same balance shows up in helping a spouse with vision loss without turning support into control.
Eligibility Checklist: Is this system a good fit?
| Question | Yes or No | Next step |
|---|---|---|
| Does the patient struggle to read small print? | Yes | Use large print and read notes aloud. |
| Are medications, eye drops, or supplements discussed? | Yes | Write exact name, dose, timing, and reason. |
| Will another caregiver need the update? | Yes | Create a same-day summary before details fade. |
Neutral action: If two or more answers are yes, use a one-page visit sheet at the next appointment.
Before the Visit: Capture the Story While It Is Still Warm
The best appointment notes often start at the kitchen table, not in the exam room. That is where the story is still warm: the near-fall on Tuesday, the blurry label on the new bottle, the morning dizziness that vanished by lunch but left everyone uneasy.
Write the “why we’re here” sentence in plain language
Before the visit, write one sentence that sounds like a person, not a form:
“We are here because reading medication labels has become harder, dizziness is worse in the morning, and there was one near-fall in the bathroom last week.”
That sentence does not diagnose. It orients the visit. It gives the clinician a front door instead of asking them to climb through a window of scattered details.
List recent changes by date, not vague worry
“Worse lately” is understandable, but it is slippery. Try dates and patterns:
- March 4: missed evening eye drop because label looked similar.
- March 8: felt dizzy after lunch and sat down for 20 minutes.
- March 10: bumped into bathroom doorframe at night.
- March 12: stopped reading mail without help.
Clinicians can use patterns. Vague worry is smoke. Dates are little lanterns. A simple printable symptom diary for seniors can make those lanterns easier to carry into the visit.
Bring the medication list, eye drops, supplements, and pharmacy name
Medication notes need precision. Bring the medication list, eye drops, over-the-counter medicines, vitamins, herbal products, and the pharmacy name. If the patient uses more than one pharmacy, write that down too. It is not fussy. It is how you prevent the classic household mystery: “Which white bottle did the doctor mean?”
Ask the patient what they want said first
Before the visit, ask, “What do you want the doctor to know first?” Then write that sentence in the patient’s own words. The first concern is often not the caregiver’s first concern. The caregiver may worry about falls. The patient may worry about losing independence. Both matter.
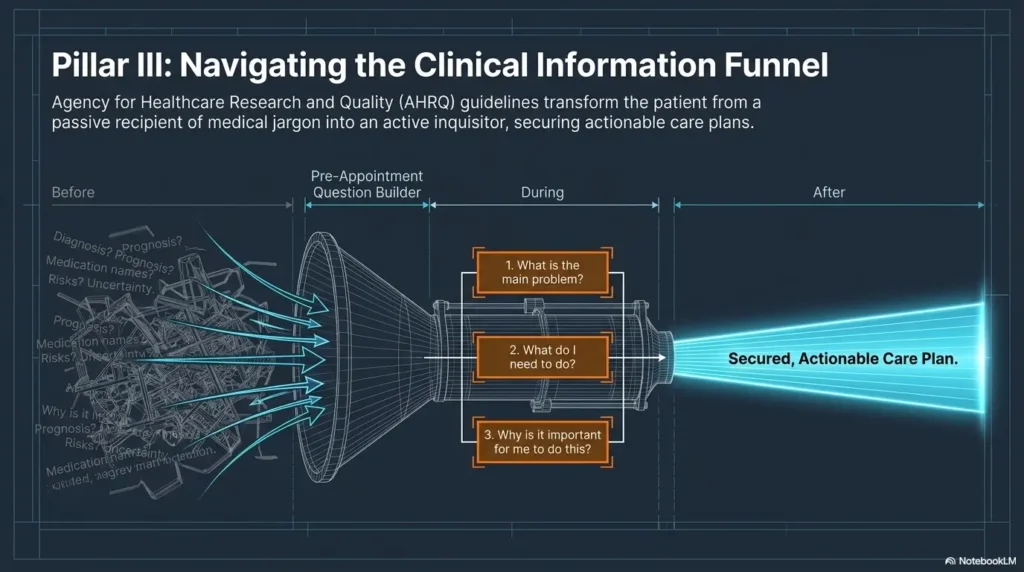
AHRQ has long encouraged patients to prepare questions and share information with clinicians because clear questions can improve the usefulness of a visit. For low vision patients, preparation also reduces the pressure to read, recall, and respond all at once.
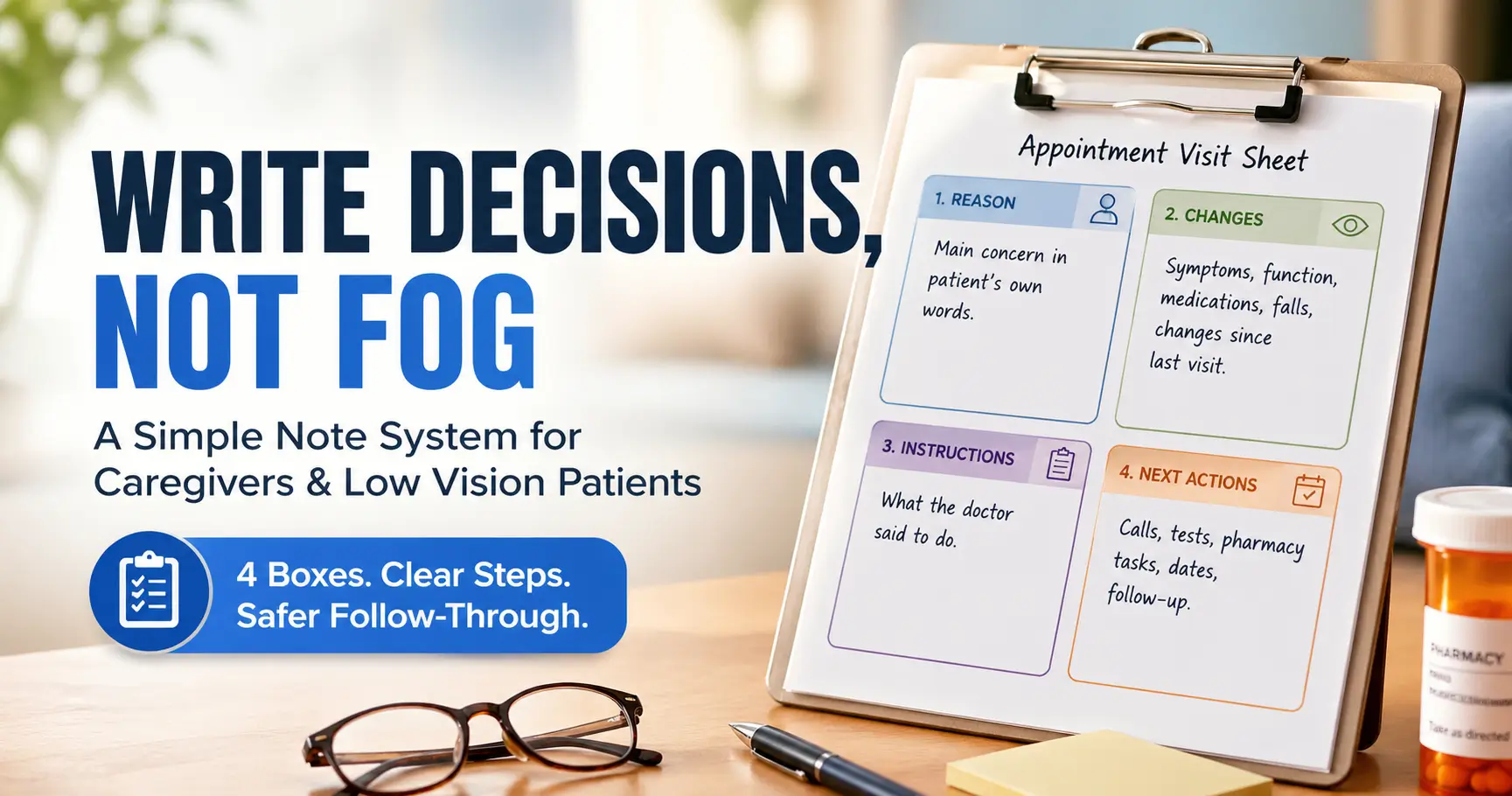
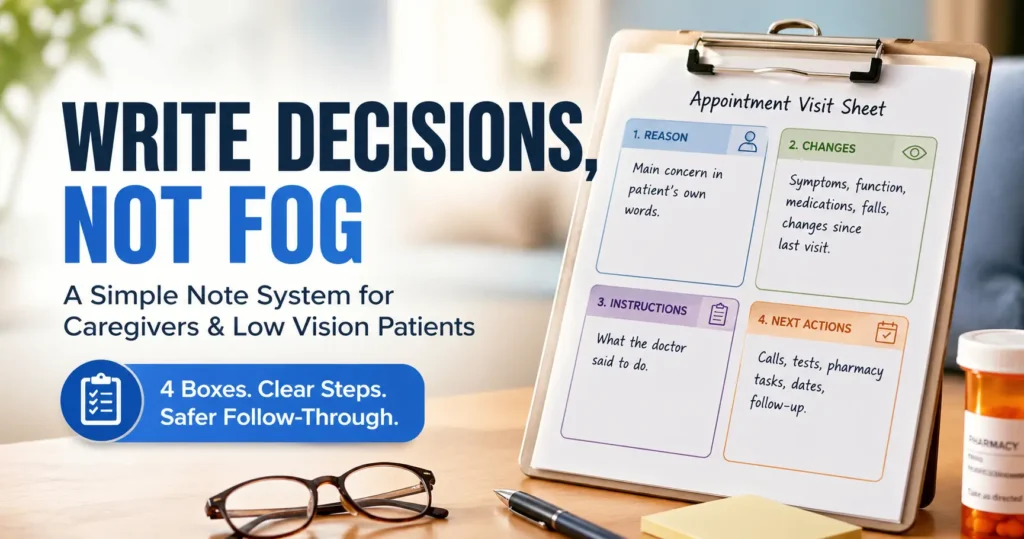
The One-Page Visit Sheet: Four Boxes That Prevent Fog
The four-box sheet is intentionally plain. It does not need flowers, tabs, color coding, or a stationery personality. It needs to be usable by a tired person in a parking lot.
Infographic: The Four-Box Visit Sheet
1
Reason
Main concern in the patient’s own words.
2
Changes
Symptoms, function, falls, pain, vision, medication issues.
3
Instructions
What the clinician said to do, written as actions.
4
Next Actions
Calls, tests, pharmacy tasks, dates, transportation, follow-up.
Box 1: Main concern in the patient’s own words
This box protects the patient’s voice. Use quotation marks if helpful. “I’m afraid I’ll take the wrong drop” is more useful than “patient has medication anxiety.” One sounds human. The other sounds like it wandered out of a filing cabinet.
Box 2: Symptoms, function, and “what changed since last time”
Function often reveals what symptoms hide. Instead of only writing “vision worse,” add daily-life clues:
- Stopped reading prescription labels without help.
- Needs brighter light for meals.
- Trips more often near the bathroom threshold.
- Avoids stairs or showering when alone.
These details help the clinician understand risk, not just complaint.
Box 3: Doctor instructions, written as actions
Write instructions as verbs. “Schedule eye exam.” “Use new drop twice daily.” “Call if dizziness worsens.” “Bring bottles next visit.” Action language is harder to misread than paragraph fog.
Box 4: Follow-up tasks, names, dates, and phone numbers
This box is where good intentions become actual care. Include who does what and by when. If the task belongs to “someone,” it belongs to the household ghost. Give it a name.
Let’s be honest: if it needs three apps, it may fail in the parking lot
Digital tools can help, especially for distance caregivers. But the core system should work even when the phone battery is low, the portal password is sulking, and the clinic hallway sounds like a blender full of shoes.
- Keep the page predictable.
- Write tasks as verbs.
- Assign names and dates before leaving.
Apply in 60 seconds: Draw one page divided into four boxes and label them before the next visit.
Low Vision Format Rules: Make the Notes Readable Before They Matter
Readable notes are safety equipment. They are not an aesthetic preference. A note that cannot be read under stress is basically a decorative napkin with medical ambitions.
Use large print, strong contrast, wide spacing, and thick pens
For paper notes, use large print, dark ink, plain fonts, and generous spacing. A thick black pen is often better than a pale fine-point pen. Avoid glossy paper when glare is a problem. If typed, consider 18-point or larger text for the patient copy, then adjust based on what the patient can comfortably read.
The National Eye Institute notes that low vision cannot be fixed with regular glasses, contacts, medicine, or surgery in the usual way. Because the barrier is not laziness or carelessness, the format must do more of the work.
Keep headings in the same order every time
Predictable order lowers cognitive load. If “Next Actions” is always the last box, the patient and caregiver know where to look. This is especially useful when stress, fatigue, pain, or hearing difficulty also enters the room carrying its little suitcase.
Avoid tiny checkboxes that become invisible under stress
Checkboxes can be useful, but tiny boxes are easy to miss. Use large circles, bold labels, or simple yes-no lines. If a task is critical, write it as a sentence, not a microscopic tick mark.
Add tactile cues: binder tabs, raised dots, clips, or page corners
Low vision systems often work better when they are not only visual. Add a raised dot to the top of the visit sheet, use a binder clip for active tasks, or fold the corner of the latest medication list. Texture can become a quiet handrail for information. A broader low vision filing system can also keep appointment notes, insurance papers, and medication updates from disappearing into the paper weather.
Show me the nerdy details
For many low vision readers, consistency beats complexity. The practical goal is not simply larger text. It is reducing search time, visual clutter, glare, and decision load. Use predictable headings, left alignment, strong contrast, short lines, and enough blank space so the reader can locate the next section without scanning a dense page.
During the Visit: Write Decisions, Not Every Sentence
Trying to write every sentence during a medical visit is a trap. You will miss the tone, lose the thread, and possibly write “take blue thing morning maybe” with the confidence of a pirate map.
Record the diagnosis or working explanation exactly as stated
If the clinician gives a diagnosis, working diagnosis, or explanation, write the wording as clearly as possible. If you are unsure, ask: “Can you say the name of that again so I can write it correctly?” This is not annoying. It is useful.
Capture medication changes with dose, timing, reason, and start date
Medication notes deserve their own small spotlight. For each medication or eye drop change, capture:
- Name of medication or drop.
- Dose or strength.
- Timing and frequency.
- Reason for the change.
- Start date, stop date, or review date.
If a medication is staying the same, write the name. “Continue same” is too vague when several bottles are living in the same cabinet like a tiny pharmacy choir. A one-page medication list template can keep those names, doses, and schedules in one dependable place.
Write down what to watch for at home
Ask what symptoms, side effects, or functional changes matter. For a low vision patient, “watch for” may need to become more concrete: new stumbling, missed doses, dizziness after medication, difficulty reading labels, worsening night navigation, or trouble using eye drops safely.
Ask: “What should we do if this gets worse before the next visit?”
This is one of the most useful questions in the room. It turns uncertainty into a plan. Write the answer in plain language, including whether to call the office, use the patient portal, go to urgent care, or seek emergency help.
Here’s what no one tells you: the best note is often a question repeated back
Before moving on, repeat the key instruction: “So we start the new drop tonight, keep the old one in the morning only, and call if dizziness gets worse. Is that right?” That tiny moment can prevent a week of household debate.
Decision Card: Paper Sheet vs. Digital Note
Use paper when…
- The patient reads large print better than screens.
- The clinic visit is fast or stressful.
- You need a visible sheet on the kitchen table.
Use digital when…
- A distance caregiver needs the summary.
- You need reminders or calendar tasks.
- The patient uses screen magnification or voice tools.
Neutral action: Most families should use both: paper for the visit, digital for sharing and reminders.
Don’t Do This: The Common Note-Taking Mistakes That Create Trouble Later
Some appointment mistakes are not dramatic. They are quiet, ordinary, and wearing sensible shoes. That is why they sneak through.
Don’t write “continue same” without naming what stays the same
“Continue same” is only safe if everyone knows exactly what “same” means. Write the medication name, dose, and schedule. For eye drops, also write which eye, if that matters. The left-right question has started many bathroom-counter negotiations.
Don’t rely on memory for medication changes
Medication changes should never live only in someone’s head. The CDC warns that medicines, including prescription drugs, over-the-counter medicines, supplements, and herbal products, can affect alertness and increase safety risks for older adults. Exact notes are not fussy. They are a guardrail. When multiple medicines and vision problems overlap, polypharmacy and vision problems deserve extra attention before the visit ends.
Don’t let the caregiver answer everything by default
A caregiver may know dates and logistics, but the patient knows the lived experience. Let the patient answer first when possible. Then the caregiver can add specifics: “That started last Thursday,” or “It happened twice this week.” This keeps the visit both respectful and useful.
Don’t bury urgent warning signs in a paragraph
Warning signs should be easy to find. Use a bold label: Call the doctor if… or Seek urgent help if…. Dense paragraphs are where important instructions go to wear camouflage.
Don’t leave without knowing who to call, and when
Before leaving, ask for the best contact method. Phone? Portal? Pharmacy? Specialist office? Primary care? Write the name or department, not just “call them.” Future-you deserves better than detective work. For pharmacy conversations, a low vision pharmacy help script can make refill, label, and medication questions less awkward and more precise.
- Name every medication that changes or stays the same.
- Separate routine instructions from urgent warning signs.
- Write the correct contact person before leaving.
Apply in 60 seconds: Add a bold line to your template: “Who do we call if this gets worse?”
Patient Voice First: Keep the Low Vision Patient in the Conversation
The best note-taking system does more than capture facts. It protects the patient from being quietly edited out of their own care.
This matters in small moments. A caregiver says, “She can’t understand the labels.” The patient goes silent. A better version is, “We want to confirm the label system because small print has made it harder to manage drops safely.” Same concern. Very different dignity.
Ask permission before taking over the explanation
Try: “Would you like me to explain what happened with the medications, or do you want to start?” This gives the patient control. It also prevents the caregiver from accidentally becoming a public-address system with a tote bag.
Read the notes aloud before leaving the room
Reading the notes aloud helps everyone catch errors. It also gives the patient a chance to say, “That is not what I meant,” or “Please add that I’m scared to shower alone.” Those details matter. They are not emotional garnish.
Use “we want to confirm” instead of “she doesn’t understand”
Language can either include or corner a person. “We want to confirm” keeps the question neutral. “He doesn’t understand” may feel like a door closing. When in doubt, choose language that preserves adulthood.
Make space for pain, fear, embarrassment, and fatigue
Low vision can make practical tasks harder, but it can also make people feel watched, rushed, or reduced. A patient may be embarrassed about needing help with labels or forms. Slow down enough to let that truth enter the room without turning it into a spectacle.
The dignity test: would you speak this way if vision were not the issue?
Before explaining something about the patient, pause and ask: Would I use this tone if vision were not involved? Would I say this in front of any adult managing a health condition? If the answer pinches, revise the sentence.
The Caregiver Question Ladder: What to Ask When Time Is Short
Medical visits can move quickly. A question ladder helps you climb from broad confusion to practical clarity before the door handle starts calling everyone’s name.
What is the most important thing to do before the next visit?
This question forces priority. If the clinician gives five tasks, ask which one matters most. A household can often handle several tasks, but it needs to know which one is the load-bearing beam.
What changed today: diagnosis, medication, test, referral, or routine?
Use this as a closing question. It helps separate “we talked about it” from “we changed it.” That difference matters, especially when several specialists are involved.
What symptoms mean we should call the office?
Write the answer in patient-friendly language. If the clinician says “worsening symptoms,” ask what that might look like at home. More dizziness? More falls? New eye pain? Increased confusion? Trouble using medication correctly?
What symptoms mean urgent care or emergency care?
This question should be asked plainly. It does not create panic. It creates a map. Families often feel calmer when they know what counts as urgent.
Can we get instructions in large print or through the patient portal?
Ask for accessible instructions. Some clinics can print larger text, send portal messages, provide after-visit summaries, or help clarify medication lists. The AHRQ QuestionBuilder approach encourages patients and caregivers to prepare visit details and questions ahead of time, which pairs well with large-print notes.
Quote-Prep List: What to Gather Before Comparing Care Options
If a visit may lead to home care, low vision rehabilitation, transportation help, medical equipment, or medication changes, gather these details before making calls.
- Current diagnosis or working explanation.
- Medication and eye drop list.
- Insurance card and pharmacy information.
- Recent falls, near-falls, or safety concerns.
- Tasks the patient can no longer do safely alone.
Neutral action: Keep this list in the same folder as the visit sheet so calls are faster and less guessy.
After the Visit: The 20-Minute Parking Lot Review
The parking lot review sounds almost too simple. That is why it works. Before the visit dissolves into traffic, lunch, pharmacy lines, and someone asking where the sunglasses went, take 20 minutes to translate the appointment into life.
Read the instructions aloud before driving away
Read the main instructions aloud while the clinic is still reachable. This is the moment to catch missing details, not three days later while holding two nearly identical bottles under a kitchen light that hums like a tiny refrigerator.
Circle anything unclear while the clinic is still reachable
If something is unclear, circle it. Then call, walk back in, or send a portal message as appropriate. Do not rely on “I think they meant…” for medications, warning signs, test prep, or follow-up timing.
Turn instructions into calendar tasks, pharmacy tasks, and home tasks
Every instruction should become a task category:
- Calendar: follow-up visit, test date, transportation.
- Pharmacy: refill, new prescription, side-effect question.
- Home: label bottles, improve lighting, remove tripping hazard.
- Communication: update distance caregiver, message clinic, call specialist.
A practical low vision calendar system for appointments can turn those follow-up dates into something visible, repeatable, and harder to miss.
Send a summary to the distance caregiver, if appropriate
A simple same-day summary can prevent family confusion. Use plain language: “The main change today was…” Then list the next 3 tasks. No one needs a novel. They need a compass.
Tiny ritual, big payoff
I like the parking lot review because it respects human limits. It admits that everyone is tired. It says, “Let’s not ask tomorrow’s memory to carry today’s details.” That is not overplanning. That is mercy with a pen.
Mini Calculator: How many follow-up tasks are you carrying?
Use this quick count after the visit.
Neutral action: If the number is 3 or higher, assign names and dates before bedtime.
When to Seek Help: Notes Are Not Enough for Red Flags
A good note-taking system supports care. It does not replace care. The difference matters most when symptoms change quickly or safety starts to slip.
Seek urgent help for sudden vision loss, severe eye pain, new weakness, chest pain, trouble breathing, or confusion
Do not use appointment notes as a waiting room for serious symptoms. Sudden vision loss, severe eye pain, new weakness, chest pain, trouble breathing, severe confusion, or signs of stroke require urgent medical attention. If symptoms feel dangerous or rapidly worsening, seek emergency help. It also helps families know the senior vision changes warning signs that should not be filed away for “next time.”
Call the clinician promptly for medication side effects, falls, worsening dizziness, or unclear instructions
Call the clinician when there are possible medication side effects, a fall, worsening dizziness, unusual sleepiness, repeated missed doses, or confusion about instructions. The CDC’s STEADI resources focus on fall prevention for older adults and include patient and caregiver materials, which is a useful reminder that falls often connect to medication, balance, vision, and home setup.
Ask for low vision rehabilitation support when reading, cooking, medication use, or mobility is getting harder
Low vision rehabilitation can help people build skills and use tools that support daily life and independence. Ask the eye care provider, primary care clinician, or specialist whether low vision services may be appropriate, especially if reading, cooking, medication use, mobility, or home safety is becoming harder.
Treat repeated “I’m fine” answers as incomplete if function is clearly slipping
“I’m fine” can mean many things: I am tired, I am embarrassed, I do not want to worry you, I do not want another appointment, or I have not found the words yet. If function is changing, ask specific questions: “Did the stairs feel harder this week?” “Any missed drops?” “Any close calls in the bathroom?” Specific beats polite fog. For bathroom-related close calls, low vision nighttime bathroom safety is often one of the first home areas worth reviewing.
- Do not wait on sudden or severe symptoms.
- Call promptly when medication or fall risk changes.
- Ask about low vision rehabilitation when daily tasks become unsafe.
Apply in 60 seconds: Add a red box to your visit sheet labeled “When to call or seek urgent help.”
Next Step: Make One Reusable Visit Sheet Today
The hallway feeling from the beginning does not disappear because families become perfect. It fades because the system catches what tired people drop.
Create four headings: Reason, Changes, Instructions, Next Actions
Start with one page. Four headings. Nothing fancy. If the page looks too simple, good. A medical visit is already complicated enough. The paper does not need to audition for a design award.
Print it in large type or save it as a phone note template
Make one version the patient can use. Make one version the caregiver can share. If using a phone, enlarge the text and test it before the appointment. The clinic waiting room is not the ideal place to discover that your template requires seven taps and the patience of a monk.
Put copies with the medication list, insurance card, and glasses
Store the sheet where appointment items already live. A folder, tote pocket, binder, or envelope can work. The best location is boring, obvious, and repeatable.
Use it at the next appointment, then improve only what caused friction
Do not redesign the whole system after one visit. Improve the part that caused friction. If the medication box was too small, enlarge it. If the patient could not read the headings, increase contrast. If the distance caregiver needed details faster, add a summary line.
Your 15-minute pilot: Create the four-box sheet, print or save it, add the medication list, and choose one person who will review it after the next visit. That is enough for today. Small systems are how households become safer without becoming colder.
FAQ
What should a caregiver write down during a doctor appointment?
A caregiver should write the main concern, the diagnosis or working explanation, medication changes, test orders, warning signs, follow-up date, and the exact next action. The note should be action-based, not a transcript. A transcript may feel thorough, but a clear task list is what helps at home.
Should the caregiver record the doctor visit?
Only if clinic policy allows it and everyone agrees. Many offices have privacy rules, and some clinicians may not permit recordings. A written or typed visit summary is usually easier to review, enlarge, print, and share with approved family members or caregivers.
How can notes be made easier for a low vision patient to read?
Use large print, high contrast, short sections, bold labels, wide spacing, and predictable headings. Avoid pale ink, glossy paper, and tiny checkboxes. Reading the notes aloud also helps preserve the patient’s control and gives them a chance to correct or add details.
What should be on a medication note?
A medication note should include the medication name, dose, timing, reason, start or stop date, side effects to watch for, pharmacy, and who to call with questions. For eye drops, also include which eye and timing if the instructions are different for each eye.
How can a caregiver avoid speaking over the patient?
Ask the patient what they want covered before the visit, let them answer first when possible, and step in only to clarify dates, medication names, safety concerns, or details the patient wants help explaining. Use language such as “we want to confirm” instead of speaking about the patient as if they are not present.
What if the caregiver and patient remember different instructions?
Contact the clinic, review the after-visit summary, check the patient portal, and ask for clarification in writing. Do not guess about medication, treatment, testing, or safety instructions. Different memories are common after a stressful visit; clarification is safer than confidence theater.
Should appointment notes be digital or paper?
Use whichever format the patient and caregiver will actually review. Many families do best with both: a large-print paper sheet for the visit and a digital copy for sharing, reminders, and distance caregiver updates.
What is the most important follow-up step after the visit?
Turn the doctor’s instructions into one concrete next action. That may be calling the pharmacy, scheduling a test, updating the medication list, arranging transportation, improving lighting near medications, or messaging the clinic for clarification.
Can a home health aide use this system?
Yes, if their role allows it and the patient agrees. A home health aide can help capture practical details such as missed doses, mobility changes, trouble reading labels, or safety concerns. Medical decisions should still be handled by the patient, authorized caregiver, and clinician.
What if the patient does not want help taking notes?
Respect the patient’s choice unless there is an immediate safety concern. Offer a lighter option: “Would you like me to write only the medication changes?” or “Would you like me to read the after-visit summary aloud?” Support should feel like a handrail, not a takeover.
Conclusion: A doctor appointment note-taking system for a caregiver and low vision patient is not a paperwork hobby. It is a small safety practice that keeps the patient’s voice present, makes instructions readable, and turns medical advice into doable next steps.
The appointment may still feel rushed. The hallway may still be noisy. The portal may still ask for a password nobody remembers. But with one repeatable page, four clear boxes, and a 20-minute review, the family no longer has to carry the whole visit in fragile memory.
Do this within 15 minutes: Make one large-print visit sheet with Reason, Changes, Instructions, and Next Actions. Put it with the medication list and insurance card. Use it once. Then improve the one part that felt clumsy. That is how safer systems begin: not with perfection, but with one page that remembers when people are tired.
Last reviewed: 2026-04.