
Cataract Surgery for Diabetics: Extra Risks and Questions to Ask Your Surgeon – 10 Must-Know Mistakes I Nearly Made as a First-Time Patient
The week before my first cataract surgery, I found myself obsessing more about parking logistics than about how my diabetes might affect the procedure. If that sounds painfully familiar, you’re in the right place. People with diabetes are more likely to develop cataracts earlier than most, and unfortunately, we also get bonus complications—like swelling in the retina or macula and a higher risk of vision loss if things aren’t handled just right.
In the next few minutes, I’ll walk you through the unique risks cataract surgery poses for people with diabetes, the critical questions I wish I’d asked my surgeon before they came at my eye with a laser, and the 10 near-mistakes I almost made—so you don’t have to. I know you’re probably juggling a million things, possibly worried about cost, and frankly sick of playing amateur medical detective, so I’ve kept this practical. Expect checklists, mini calculators, and even some ready-made conversation starters you can take straight to your eye care team today.
Table of Contents
Why cataract surgery feels different when you have diabetes
For most people, cataract surgery gets pitched as a quick, almost routine tune-up: in and out, tiny incision, shiny new lens, back to life. That story is mostly true—unless you add diabetes.
People with diabetes are more likely to develop cataracts, to develop them younger, and to watch them progress faster than their friends without diabetes. That means many of us hit the operating room while we’re still working, driving, caring for kids—or parents. The stakes feel higher.
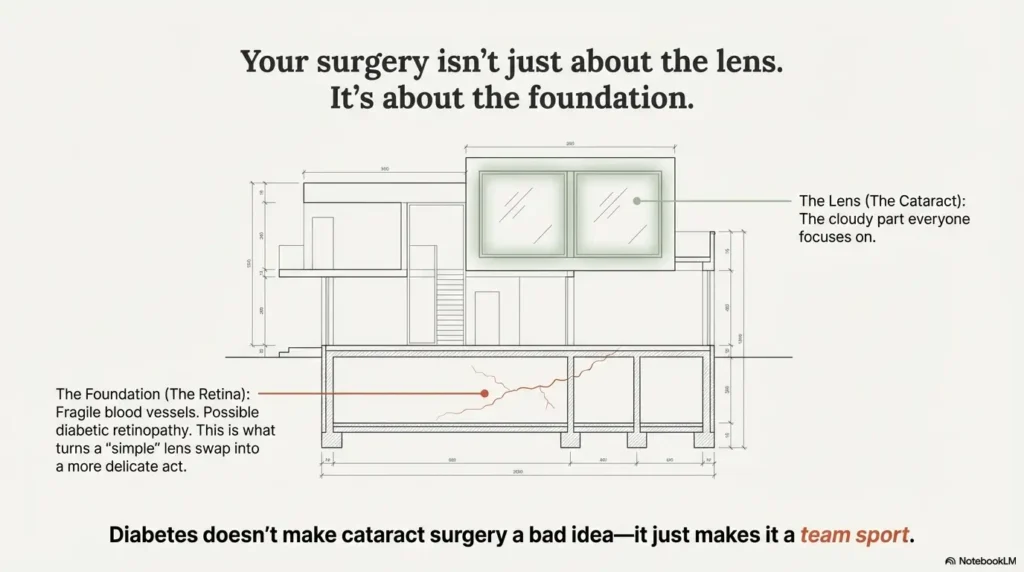
And underneath the cloudy lens, there’s the retina: fragile blood vessels, maybe early diabetic retinopathy, maybe tiny leaks in the macula. That’s the part that turns a “simple” lens swap into a more delicate balancing act. Diabetic eye disease—especially diabetic retinopathy and diabetic macular edema—is one of the leading causes of preventable blindness in adults.
Here’s the good news: with the right prep, a cautious surgeon, and honest diabetes control, cataract surgery can improve vision and protect long-term eye health. This article is the conversation I wish someone had with me before I signed the consent form.
Think of this as your “translator” between surgical optimism and diabetic reality.
60-second diabetic cataract surgery readiness check
Before we dive into the scary (and fixable) details, run this quick self-check. It’s not a medical verdict—just a reality snapshot you can bring to your next visit.
Money Block #1 – Eligibility-style checklist
Answer each with a simple “Yes/No/Not sure”.
- I’ve had a full dilated eye exam (including retina) in the last 6–12 months.
- Someone has told me clearly whether I do or do not have diabetic retinopathy.
- I know my latest HbA1c and fasting/post-meal glucose pattern from the last 3 months.
- My diabetes team has weighed in on whether this is a good time for elective surgery.
- I understand whether my macula is dry, swollen, or at risk for edema.
- I have a written estimate of cataract surgery cost, including lenses and follow-up.
- I know which medications (including insulin, GLP-1, SGLT2, etc.) to adjust on surgery day.
- I have someone to drive me home and stay reachable the first 24 hours.
- I know who to call after hours if my eye suddenly hurts or vision drops.
Rule of thumb: If you have more than three “Not sure” answers, your next appointment shouldn’t just be for surgery—it should be for questions.
Save this checklist and confirm each point with your own eye team before scheduling surgery.
Extra risks of cataract surgery when you have diabetes
Let’s name the elephant in the operating room: yes, cataract surgery is generally safe, but diabetes adds some specific risks your surgeon and retina specialist will be watching for.
1. Higher risk of macular edema (retinal swelling)
When the cloudy lens is removed, inflammation in the eye temporarily increases. In people without diabetes, this usually settles down quietly. In people with diabetes—especially if any retinopathy is present—the fragile capillaries in the retina can leak, causing diabetic macular edema (DME), a swelling in the center of vision that can blur or distort what you see.
Recent studies have confirmed that poorer pre-surgery blood sugar control (higher HbA1c) is linked with a higher risk of post-surgery cystoid or diabetic macular edema.
2. Possible progression of diabetic retinopathy
Cataract surgery can modestly increase the risk that existing diabetic retinopathy moves to a more severe stage, particularly if it was already present or poorly controlled. That doesn’t mean surgery is a mistake; it means your retina may need tighter follow-up and sometimes preventive treatment (such as injections or laser) before or after the lens swap.
3. Slower healing and slightly higher infection risk
Poorly controlled blood sugar can slow wound healing and increase the risk of infection in many surgeries, including eye surgery. The eye incision is tiny, but it still needs a clean, well-fed body to heal. Good perioperative control is less about achieving perfection and more about avoiding big, chaotic swings in glucose during the healing window.
4. Glare, halos, and “vision disappointment”
If the retina isn’t healthy, a perfect new lens can still deliver imperfect vision. Some diabetics feel underwhelmed after surgery because retinopathy, DME, or nerve damage limits the sharpness they can achieve—even when the cataract is gone. Managing expectations is part of protecting your mental health around surgery.
- Ask directly about your risk of macular edema and retinopathy progression.
- Expect extra retina imaging (OCT, photos) before and after surgery.
- Plan tighter glucose control around the surgery window, not perfection forever.
Apply in 60 seconds: Write down one question about macular edema and one about retinopathy to ask at your very next visit.
Questions to ask your cataract surgeon when you live with diabetes
This is the part where we turn vague dread into concrete, answerable questions. Print these, screenshot them, or copy them into your notes app. You won’t remember them all in the waiting room.
1. “How healthy is my retina right now?”
- Do I have diabetic retinopathy? If yes, what stage?
- Is there any sign of macular edema or previous bleeding?
- Should I see a retina specialist before surgery?
2. “What is my personal risk of macular edema after surgery?”
- Do we need extra anti-inflammatory eye drops or injections to protect the macula?
- Will you use OCT (retinal scan) before and after surgery to monitor swelling?
3. “Is this the right time, given my diabetes control?”
- Given my HbA1c and glucose pattern, would you recommend we stabilize control first?
- Are there diabetes-related reasons to delay or not delay surgery?
4. “How will you coordinate with my diabetes team?”
- Which medications should I take the morning of surgery—insulin, GLP-1, SGLT2, metformin?
- Who decides adjustments—your team or my endocrinologist/primary care doctor?
5. “What lens options are actually worth paying for in my situation?”
- Given my retina health, would a premium multifocal or toric lens actually help, or could it worsen glare?
- What are the coverage tiers and premium lens upgrades—what’s standard, and what counts as an upgrade, with extra premium and out-of-pocket costs?
6. “What will I realistically see—and when?”
- How quickly should I expect usable vision for driving, reading, and screens?
- What symptoms are normal in the first weeks, and which are a red flag?
7. “Who do I call at 10 p.m. if something feels wrong?”
- Is there a 24-hour number for sudden pain, flashes, or dark shadows?
- What’s the emergency plan if my blood sugar crashes or spikes around surgery?
Take these questions, add your own money questions, and reframe the visit: you are interviewing the surgery team, not the other way around.
10 must-know mistakes I nearly made as a first-time diabetic cataract patient
Here are the exact landmines I almost stepped on. Think of them as signposts: you might not hit every one, but even dodging two or three can protect your eyes and your wallet.
1. Treating cataract surgery like a quick errand
I almost treated the procedure like a dental cleaning—pick a date, show up, done. The reality? For diabetics, it’s more like planning a small project: pre-op labs, retina imaging, medication adjustments, rides, time off work, and a follow-up schedule.
Better move: Put surgery and follow-up dates on a calendar and block out your first 48–72 hours after each eye. Protect the time the way you’d protect an important work deadline.
2. Going in with “mystery” blood sugar
At one point, my plan was, “I’ll just do my best that week.” That’s not a plan; that’s vibes. Studies show that poorer pre-op glycemic control is associated with higher risk of post-cataract macular edema.
Better move: Aim for a calm, boring glucose pattern in the weeks before surgery, not a crash diet of strict control. Bring your last 2–4 weeks of readings (or CGM download) to pre-op so the team can see your usual pattern, not your best day.
3. Ignoring the retina because “the cataract is the main problem”
At first I was so focused on fixing the cloudy lens that I barely asked about the retina underneath. That’s like renovating a house without checking if the foundation is cracked.
Better move: Ask specifically: “Is my retina healthy enough that a new lens will actually deliver good vision? Do we need to treat retinopathy or edema before surgery?” In some cases, retina treatment first can dramatically improve your odds of a clear result.
4. Assuming all lenses are created equal—for all eyes
The brochure made every intraocular lens sound magical. But in diabetics, especially with retinopathy or macular changes, some “premium” lenses don’t play nicely with contrast or night vision.
Better move: Ask, “If this were your eye, with this retina and this level of diabetes, which lens would you choose and why?” Expensive is not the same as appropriate.
5. Not asking for a real cost breakdown
I almost signed the consent form without a written estimate that separated standard coverage vs. upgrades, deductibles, and out-of-pocket costs. In many places, standard monofocal cataract surgery is covered by insurance or public systems, but laser-assisted surgery and premium lenses can add thousands per eye.
Better move: Ask for a line-item estimate: surgeon fee, facility fee, anesthesia, lens type, post-op visits, and any separate retina imaging. Treat it like any other major purchase.
6. Forgetting that anesthesia and fasting rules interact with diabetes
The instructions said, “Nothing to eat after midnight.” My insulin pen said, “Absolutely not.” That mismatch can lead to dangerous lows or highs on surgery day.
Better move: Ask early: “What’s the plan for my insulin and other meds on surgery day?” and “Who is responsible for that plan?” Insist on a written set of instructions, and share them with whoever is driving you.
7. Underestimating recovery time—and screen time
I pictured myself back on a laptop in 24 hours. Instead, my eye felt gritty, my focus changed from hour to hour, and bright screens were exhausting.
Better move: Expect a few days of fuzzy, “soft-focus” vision and plan lighter duties if you work on screens all day. Give yourself permission to be slightly slower and more cautious, especially with stairs and night driving.
8. Not planning for “what if something goes wrong?”
Everyone reassured me that complications were rare (true), but no one pushed me to plan for them (less ideal). For diabetics, retinal swelling, pressure spikes, or infections—even if rare—can be more serious.
Better move: Before surgery, ask: “If I develop macular edema or a pressure spike, what’s our plan? Do you treat it here or refer me?” Knowing the next step makes it less terrifying if you need it.
9. Assuming one surgery fixes all vision problems forever
Cataract surgery can dramatically improve clarity, but it doesn’t “cure” diabetic eye disease. Retinopathy, glaucoma risk, and macular changes still need lifelong monitoring.
Better move: Treat the surgery as a chapter, not the whole book. Ask your team how often you should have dilated exams and retinal imaging after surgery, given your diabetes duration and control.
Costs, coverage tiers, and out-of-pocket estimates (2025, US)
Now for the uncomfortable part: money. Cataract surgery is one of the most commonly performed operations in the world—and in the United States, it’s also a significant business.
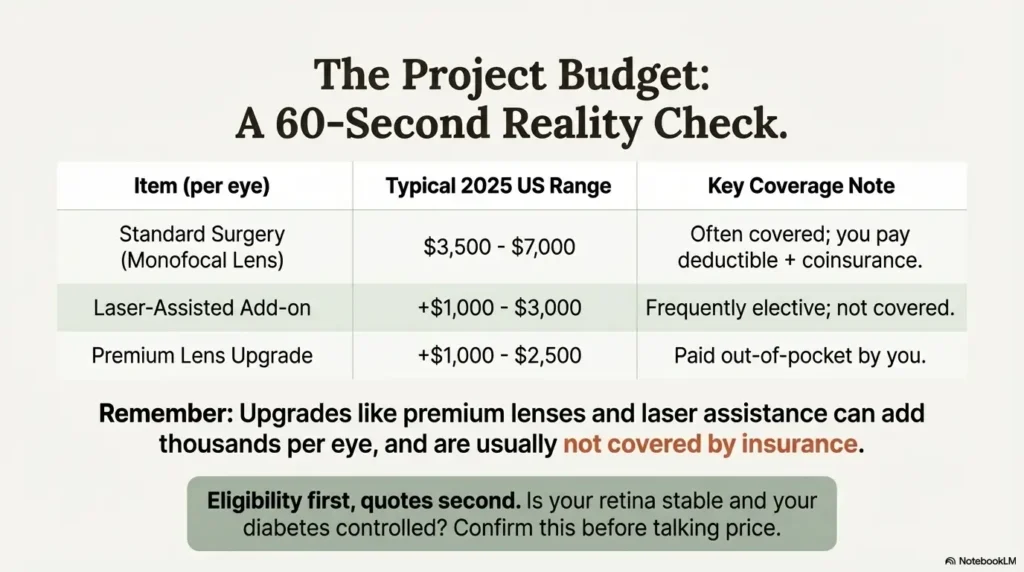
In many US clinics, standard cataract surgery without insurance often ranges from around $3,500 to $7,000 per eye, depending on where you live, the technology used, and the lens you choose. With Medicare or good private insurance, your out-of-pocket can shrink to a few hundred dollars in coinsurance and deductibles for standard surgery, but extras such as laser assistance or premium multifocal lenses are usually paid fully by you.
And remember: you may also face costs for pre-op retina imaging, extra follow-up visits, and additional treatments if diabetic macular edema appears later.
Money Block #2 – Sample fee/coverage table (US, 2025)
| Item (per eye) | Typical 2025 range (US) | Coverage notes |
|---|---|---|
| Standard cataract surgery with monofocal lens | $3,500–$7,000 cash price | Often covered by Medicare/private insurance; patient pays deductible + ~20% coinsurance for approved charges. |
| Laser-assisted surgery / advanced technology add-on | +$1,000–$3,000 | Frequently considered elective; many plans do not cover the extra premium. |
| Premium multifocal or toric lens upgrade | +$1,000–$2,500 | Paid out-of-pocket in many plans; check if medically necessary astigmatism correction changes coverage. |
| Medicare facility coinsurance (standard surgery) | About $384–$598 on average | Actual number varies by region and facility; Medigap or secondary coverage can reduce this. |
These are broad, illustrative ranges, not quotes. Your local costs, coverage tiers, and deductible structure may look very different.
Save this table and confirm the current fee on your provider’s official fee schedule or written estimate.
Money Block #3 – 60-second out-of-pocket estimator
Quick estimator (not financial advice):
USD%
Take a screenshot or write down this number, then compare it to your clinic’s written estimate and insurance explanation of benefits.
Eligibility first, quotes second. Before chasing “cheapest surgery,” confirm the basics: is your retina stable, is your diabetes reasonably controlled, and is your surgeon comfortable managing higher-risk eyes?
Money Block #4 – Quote-prep list before you compare carriers or clinics
Have these in front of you before you request insurance quotes or clinic estimates:
- Your diabetes type, duration, and latest HbA1c.
- Whether you have diabetic retinopathy or macular edema documented.
- Whether you need surgery in one eye or both in the next 12–18 months.
- Your current deductible used this year, and your out-of-pocket maximum.
- Whether you’re considering any premium lenses or laser add-ons.
- For Medicare: which Part (A/B/C/D) you have and any Medigap plan.
Save this list and confirm each number against your insurer’s official plan documents or a benefits specialist.
Recovery, retina care, and long-term diabetes control
Once the surgery is over, the real test begins: how well your eye heals, how your retina behaves, and how your diabetes behaves around all of that.
Short Story: The day my “perfect” surgery suddenly felt risky
(120–180 words)
Two weeks after my first cataract surgery, I walked into the kitchen and noticed a weird bend in the edge of the countertop. Straight lines bowed. White tiles looked patchy. The surgeon had said everything went “beautifully,” so my first thought was, “I’m imagining this.” My second thought was, “Or my retina is quietly freaking out.”
I called the clinic, half expecting to be told to relax. Instead, they brought me in the same day, ran an OCT scan, and found a small area of swelling near the macula—nothing dramatic, but enough to explain the distortion. We added more anti-inflammatory drops and closer follow-up. It resolved over the next few weeks, but the real lesson was this: the end of surgery is not the end of risk, especially with diabetes in the background. Your job after surgery is simple but serious—notice changes, speak up early, and keep your glucose steady enough that your eye can do the quiet work of healing.
How often should I be checked after cataract surgery with diabetes?
Follow-up schedules vary, but many diabetics benefit from:
- Standard cataract checks in the first 24 hours, 1 week, and 1 month.
- Additional retina-focused visits (and OCT scans) in the first 3–6 months, especially if you had retinopathy or macular edema before surgery.
- Ongoing annual or more frequent dilated exams based on your diabetes duration and control.
Guidelines for diabetic retinopathy emphasize more frequent ophthalmology visits when retinopathy is progressing or when major events—like surgery—could change the disease course.
Infographic – The three phases of diabetic cataract surgery care
Phase 1 – Before surgery
- Confirm retina status (retinopathy, macular edema).
- Stabilize glucose pattern over several weeks.
- Clarify lens choice, coverage tiers, and fee schedule.
- Coordinate with diabetes team on medication plan.
Phase 2 – Day of surgery
- Follow fasting + medication instructions exactly.
- Bring glucose meter or CGM, rescue carbs if allowed.
- Confirm ride home and 24-hour support person.
- Ask what symptoms should trigger a same-day call.
Phase 3 – After surgery
- Use drops exactly as prescribed; don’t “taper freestyle.”
- Watch for distortion, new floaters, or dark curtains.
- Keep glucose steady; avoid extreme highs/lows.
- Attend all retina follow-ups, even if you feel fine.
- Plan for at least 3–6 months of more attentive eye follow-up.
- Use new vision as motivation to keep long-term glucose in range.
- Report subtle vision changes early; don’t wait for dramatic loss.
Apply in 60 seconds: Add your next 3 eye appointments (or reminders to schedule them) to your calendar now.
If you’re having cataract surgery with diabetes in Korea
If you live in Korea, there’s an extra layer to all of this: how cataract surgery fits into the National Health Insurance Service (NHIS) and private health insurance (PHI).
NHIS does cover essential cataract surgery, and over recent years cataract procedures in Korea have increased significantly, with substantial growth in both NHIS and private insurance spending. That means you may face relatively modest copayments for standard surgery—but strong incentives from some clinics to recommend more frequent or more advanced procedures, especially if you hold generous private coverage.
For diabetics, that dynamic cuts both ways. On one hand, coverage can make timely surgery more accessible. On the other, it can nudge borderline cases toward “now” instead of “later,” even when retinopathy or macular edema might benefit from stabilization first.
Practical questions to ask in Korea (or similar NHIS-style systems):
- “Is this surgery being billed primarily through NHIS, my private policy, or both?”
- “What’s my expected NHIS copayment in won, and what are my private insurance deductibles?”
- “Would you make the same recommendation if I had NHIS only and no private coverage?”
- “Given my diabetes and retina status, what is the risk of waiting 6–12 months vs. operating now?”
Remember: coverage doesn’t automatically mean medical necessity. You’re allowed to ask whether the timing and technique are truly in your best interest, not just covered by your plan.
Nerdy risk–benefit deep dive (optional)
Show me the nerdy details
For the curious (or anxious), here’s a simplified version of what’s going on under the hood.
Why diabetics get more cataracts: Chronic high glucose can alter lens proteins and increase oxidative stress, making the lens cloudier, earlier. Longer diabetes duration is linked to higher rates of cataract and cataract surgery.
Why retinopathy can worsen after surgery: Cataract surgery increases intraocular inflammation and can temporarily disrupt the blood–retina barrier. In eyes with diabetic retinopathy, those vessels are already fragile, so postoperative leakage and progression risk rises—especially if baseline control is poor.
Why macular edema is such a big deal: The macula is the part of the retina that handles fine detail and reading. When fluid leaks into it—whether as classic cystoid macular edema or diabetic macular edema—vision can look blurry, wavy, or washed out. Anti-inflammatory drops, steroid injections, or anti-VEGF injections may be used to treat it, depending on the pattern and severity.
Why your surgeon might add “extra” drops: Some guidelines recommend combining steroid and NSAID eye drops in diabetics, even without visible retinopathy, to reduce the risk of cystoid macular edema after surgery.
None of this means cataract surgery is unsafe for diabetics. It means you and your team are piloting a more complex flight plan—and need clearer instruments and better communication.
FAQ
Is cataract surgery safe if I have diabetes?
For most people with diabetes, yes—cataract surgery is still considered safe and can significantly improve vision. The key differences are extra attention to your retina status, tighter monitoring for macular edema, and more deliberate glucose management before and after surgery. Your 60-second action: ask your ophthalmologist directly, “Given my diabetes and retina status, do you see any special risks or extra steps we should take?”
Will cataract surgery fix my blurry vision from diabetic retinopathy?
Not necessarily. Cataract surgery replaces the cloudy lens at the front of the eye, but it doesn’t repair retina damage. If diabetic retinopathy or macular edema is causing blurriness, you may need separate retina treatments (like anti-VEGF injections or laser) before or after surgery. Your 60-second action: ask, “What percentage of my blur is from the cataract versus retina problems?”
How much does cataract surgery usually cost if I’m on Medicare in the US?
Standard cataract surgery with a basic monofocal lens is generally covered under Medicare Part B, but you’re usually responsible for about 20% of the allowed charges after your deductible. In 2025, that commonly translates to a few hundred dollars in facility coinsurance per eye, plus any physician fees and non-covered upgrades. Your 60-second action: call your insurer and ask, “What would my total coinsurance be for CPT 66984 (standard cataract surgery) at my chosen facility?”
How long should I plan to be off work after cataract surgery with diabetes?
Many people return to light work within a few days, but diabetics may want a bit more margin—especially if your job involves screens, driving, or heavy lifting. Expect a few days of visual fluctuation and fatigue. Your 60-second action: look at your work calendar and block 2–5 lighter days after each eye, with no critical deadlines or night driving.
What symptoms after surgery are an emergency?
Call your surgeon or emergency line immediately if you notice severe eye pain, sudden vision loss, a dark curtain, many new floaters, or flashes of light. These can signal infection, retinal detachment, or serious pressure spikes—conditions where hours matter. Your 60-second action: save your clinic’s 24-hour number in your phone under “Eye Emergency” and share it with your support person.
Can I ever avoid cataract surgery if I have diabetes?
Sometimes mild cataracts can be managed for a while with updated glasses, glare control, and good diabetic eye care. But once cataracts interfere with daily tasks—driving, reading, safe walking—surgery is usually the only way to restore clear vision. Your 60-second action: ask your doctor, “If I delay surgery 6–12 months, what do you realistically expect to happen to my vision and retina?”
Conclusion: your next 15 minutes
Cataract surgery for diabetics is not a simple “yes/no” question; it’s a series of small, navigable decisions. The surgery itself is measured in minutes. The impact on your vision—and your life—is measured in years.
If you do nothing else today, use the clarity you have right now to make life easier for your future self:
- Book (or confirm) a dilated eye exam that includes a retina check.
- Write down your latest HbA1c and a week of glucose readings.
- Turn one of the 10 mistakes into a direct question for your surgeon.
- Start a simple “eye folder” (paper or digital) with estimates, instructions, and your own notes.
You don’t have to become an eye expert. You just have to become the quiet project manager of your own surgery—steady, curious, and willing to ask for clear explanations.
- Questions turn vague fear into clear decisions.
- Clear decisions protect both vision and money.
- Protected vision makes every other diabetes decision easier.
Apply in 60 seconds: Choose a date for surgery—or for a second opinion—and put it on the calendar with one note: “Bring questions.”
Last reviewed: 2025-12; sources included major ophthalmology and diabetes organizations and recent clinical guidelines. This guide is educational and does not replace personalized advice from your own eye-care and diabetes teams.
cataract surgery for diabetics, diabetic macular edema, diabetic retinopathy and cataract, cataract surgery costs 2025, questions to ask cataract surgeon