


Managing Glaucoma When You Already Have Other Eye Diseases: 11 Critical Questions I Wish I’d Asked Before My Next Visit
Managing Glaucoma When You Already Have Other Eye Diseases
The hard part isn’t “learning more.” It’s surviving the overlap: dry eye that mimics progression, cataracts that muddy visual fields, diabetic retinopathy or macular degeneration that hijacks the same symptoms, uveitis or post-surgery changes that turn every tweak into a trade-off.
Keep guessing, and you don’t just lose time—you risk losing clean baselines, months of momentum, and sometimes irreversible function.
Managing glaucoma alongside other eye diseases means building one coordinated plan that separates comfort from danger, sets a target intraocular pressure (IOP) for your optic nerve, and uses the right monitoring (OCT trends, visual field reliability, photos—the same core steps you’ll recognize in what happens during a glaucoma test) without getting fooled by “bad test days” or medication side effects.
I learned it the annoying way: the data wasn’t wrong, it was just noisy.
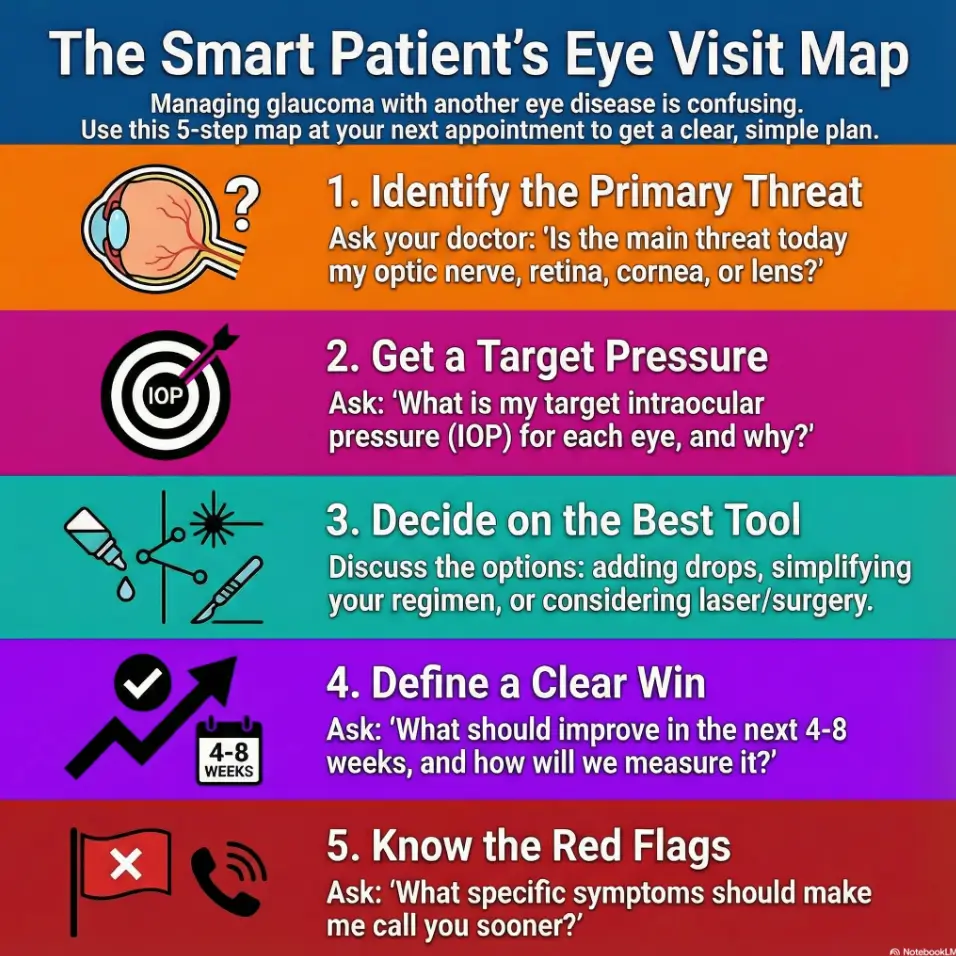
Your 11-Question Visit Script & One-Page Plan
Print this. Copy it into Notes. Bring it to the chair.- Lock a target IOP (each eye) so decisions stop drifting
- Spot when drops, preservatives, or timing are the real problem
- Know when laser/procedure is smarter than adding bottle #4
Table of Contents
Why glaucoma gets messy with other eye diseases
Glaucoma is already a quiet disease. Add dry eye, cataracts, diabetic retinopathy, macular degeneration, uveitis, or “I had surgery last year and nothing feels normal,” and it becomes a choir where every singer insists they’re the soloist.
Here’s the core problem: symptoms don’t map neatly to diagnoses. Blurry vision can be pressure, cornea, lens, retina, or medication side effects. A “worse” visual field can be glaucoma—or a bad test day— or a retina issue tugging the same data. (If you’ve ever wondered what’s “normal aging” versus something that needs a closer look, glaucoma vs normal aging can help you put that confusion into words.)
I learned this the annoying way. I panicked over one scary test printout, then found out my eyes were just dry and my lids were twitching like they were auditioning for a drumline. The test wasn’t lying; it just wasn’t telling the whole truth.
- Ask which disease explains which symptom.
- Ask which test result actually changed.
- Ask what “success” looks like in 30–90 days.
Apply in 60 seconds: Write down your top 2 symptoms and when they happen (morning vs night).
Scannable reality check:
- Glaucoma damage is often painless; surface disease isn’t.
- One “bad” test can be a fluke; two trends are a pattern.
- Most plans fail because the visit ends without a clear target.
Question 1: What exactly is damaged right now—and how do we know?
This sounds basic. It’s not. When you have more than one eye disease, you need the clinician to point to the specific structure and the specific evidence.
Ask it like this: “Is the main threat today my optic nerve, my retina, my cornea, or my lens?” Then follow with: “Which test shows that, and what changed since last time?”
If they say “your scan,” ask which scan: optic nerve OCT, macular OCT, or something else. If they say “your field,” ask if reliability was good. These questions aren’t rude. They’re how you prevent a wrong turn that costs you 6–12 months—and it helps to know the usual lineup of tests in advance (see what happens during a glaucoma test if you want the “what are they actually measuring?” version).
My own mistake: I once assumed “pressure was fine” meant “glaucoma was fine.” Nope. My optic nerve was still showing progression, and pressure was “fine” only on paper, not for my nerve.
Show me the nerdy details
Glaucoma risk is about pressure relative to your optic nerve’s tolerance. Some nerves handle higher pressures; others don’t. OCT trends and visual field trends help detect progression, but both can be distorted by cataract, dry eye, poor fixation, macular disease, and test fatigue.
Quick mini-script (30 seconds):
- “What changed—structure, function, or just symptoms?”
- “Is the change big enough that you’d treat your own family member differently today?”
- “If we do nothing, what’s the likely downside in 12 months?”

Question 2: What is my target pressure—and what changes it?
If you remember only one question, remember this one. A plan without a target pressure is like dieting without a scale: you can work hard and still drift.
Ask: “What is my target intraocular pressure (IOP) for each eye, and why?” If you have asymmetric disease, your right eye and left eye may have different targets. That’s normal.
Then ask what changes it: thinner corneas, optic nerve appearance, family history of eye disease, past progression, steroid response, angle anatomy, and coexisting retinal disease that makes monitoring harder. If you have other eye diseases, your doctor may choose a more conservative target because the margin for error is smaller.
Personal confession: I used to treat IOP like a grade. Under 20? Gold star. Now I treat it like a speed limit that depends on road conditions. Rainy night? You slow down. Fragile optic nerve? You aim lower. (This is especially true if “normal pressure” glaucoma is on the table—see normal tension glaucoma after 60 if that phrase has ever shown up in your chart.)
- Get a target number, not a vibe.
- Know what would trigger a plan change.
- Ask for a timeline: 4–8 weeks for pressure check, 3–6 months for trends.
Apply in 60 seconds: Put your target IOP in your phone notes and bring it to every visit.
Two numbers that keep you honest:
- 4–8 weeks: common window to reassess a med change’s pressure effect.
- 3–6 months: a reasonable interval to re-check trends if risk is higher.
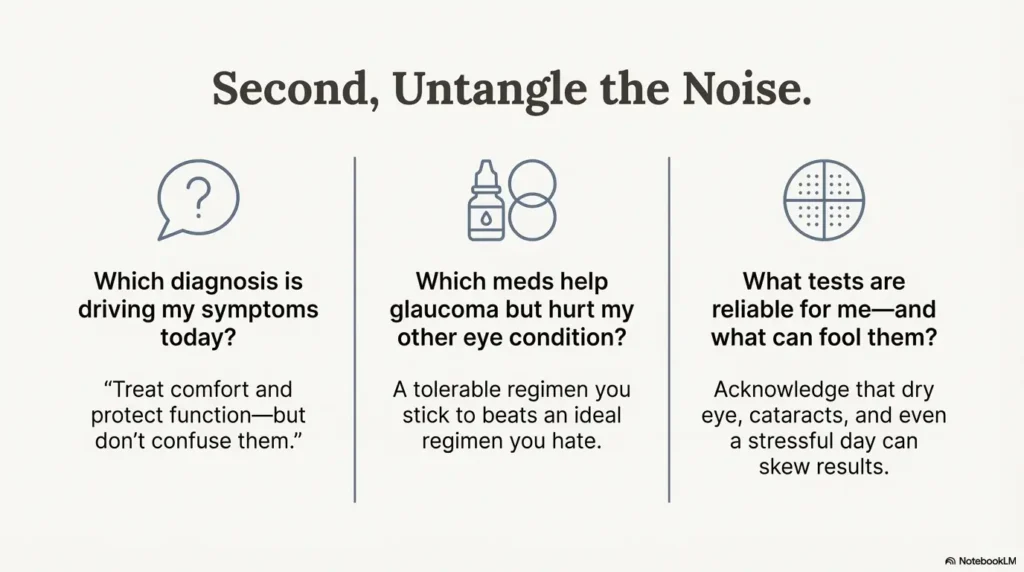
Question 3: Which diagnosis is driving my symptoms today?
When you have multiple eye diseases, your biggest suffering often comes from the one that’s most annoying, not the one that’s most dangerous. Dry eye can feel unbearable. Glaucoma can feel like… nothing. Until it isn’t.
Ask: “Which condition is most likely causing my current symptoms, and which condition is most likely causing irreversible loss if we miss it?” That forces the visit to separate comfort from safety.
Examples:
- If your eyes burn and fluctuate, dry eye or blepharitis may be louder than glaucoma.
- If your vision is hazy with glare, cataract may be the culprit (and if your clinician starts talking lenses, it helps to understand monofocal vs multifocal vs toric IOL options before you’re choosing under pressure).
- If straight lines bend, macular disease needs attention fast—especially if you’re trying to distinguish dry vs wet age-related macular degeneration.
I once chased “blur” for weeks with pressure anxiety, only to learn my contact lens habits plus dry indoor heat were wrecking my tear film. Fixing that improved my day-to-day vision in 7–14 days. Glaucoma still mattered—just not as the explanation for that particular misery.
Pull-quote to keep in your head:
Question 4: Which meds help glaucoma but hurt my other eye condition?
This is where overlap gets real. Glaucoma drops can dry you out, sting, inflame, blur, or mess with your surface—especially if you’re already dealing with dry eye, allergies, corneal disease, or post-surgery sensitivity. If you want a clear, practical breakdown of what side effects tend to show up (and what to do about them), read glaucoma eye drops side effects in seniors.
Ask: “Which glaucoma meds are best for pressure, and which are best for my ocular surface?” Then ask: “Can we reduce preservatives, simplify the regimen, or switch classes if side effects hit?”
Also ask about systemic interactions. If you have asthma, COPD, low heart rate, certain heart rhythm issues, or are on blood-pressure meds, some eye drops may need extra caution. Don’t self-diagnose—just declare the facts and let your clinician do the risk math.
My lived lesson: I once “powered through” a drop that made my eyes feel like sandpaper. I thought toughness was a virtue. It was not. My adherence fell apart after 10 days. A simpler plan I could actually follow beat the “perfect” plan I quietly avoided.
- Ask about preservative-free options if irritation is chronic.
- Ask how many “drops per day” is the realistic max for you.
- Ask what to do if you miss doses for 2–3 days.
Apply in 60 seconds: Take photos of all your bottles and put them in an album named “Eye meds.”
Mini eligibility checklist (yes/no):
- Yes/No: I can name my other eye diagnoses (even if I can’t spell them).
- Yes/No: I can list my inhalers, heart meds, and steroid use.
- Yes/No: I know which eye gets which drop and at what time.
- Yes/No: I have a plan if burning or redness spikes within 72 hours.
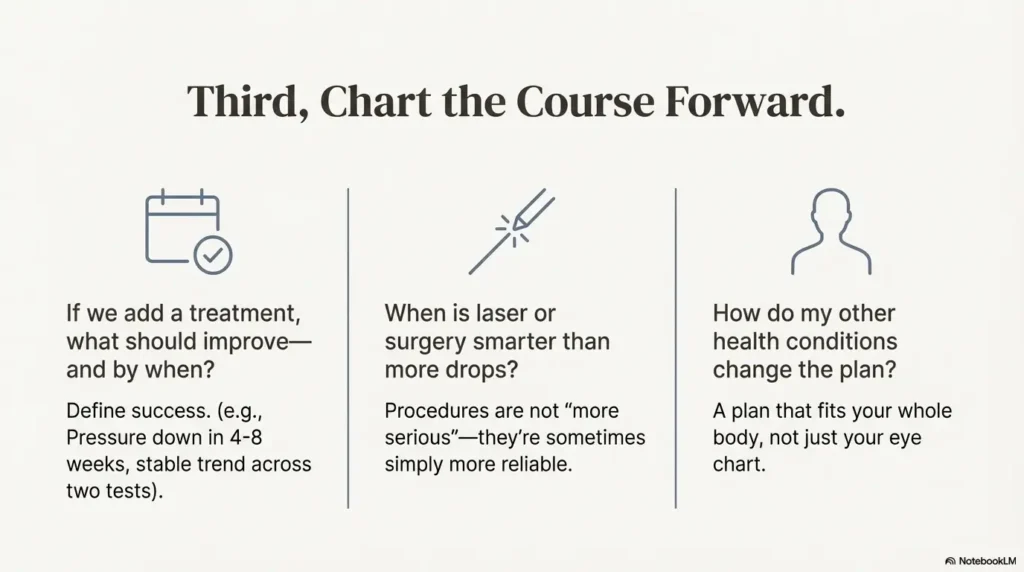
Question 5: If we add a treatment, what should improve—and by when?
When you’re managing more than one eye disease, a treatment change can improve one thing while worsening another. That’s why you need a clear “win condition.”
Ask: “What is the goal of this change—lower pressure, stabilize the nerve, improve symptoms, or reduce risk?” Then: “How will we measure success, and when?”
Examples of success metrics that don’t waste your time:
- Pressure down by a meaningful amount at the next check (often 4–8 weeks).
- Fewer side effects within 7–14 days after a switch.
- Stable trend on OCT/field across two time points, not one.
My humor-free memory: I once assumed a laser was a “cure.” The doctor said, kindly, “It’s a tool.” That sentence saved me from unrealistic expectations and helped me track what actually changed.
Decision card (When A vs B):
- Pressure is above target and you tolerate drops well.
- You can keep the schedule with <2 missed days/month.
- Dry eye or irritation is wrecking adherence.
- Multiple eye diseases make symptom tracking confusing.
- You’re already at 2–3 meds and still above target.
- Side effects or schedule fatigue are constant.
Question 6: What tests are reliable for me—and what can fool them?
Testing is where overlapping disease can quietly mislead you. Visual field testing depends on attention, comfort, and fixation. OCT depends on clean optics and correct segmentation. Cataract, corneal dryness, macular disease, and even eyelid position can skew results.
Ask: “For me specifically, which test is the best compass: optic nerve OCT, visual field, photos, or pressure trend?” Then: “What conditions in my eyes can make this test look worse than it is?”
If you have macular degeneration or diabetic retinopathy, ask whether your macula changes could affect field results. If you have cataracts, ask whether blur could reduce field sensitivity. If you have severe dry eye, ask whether the test day should start with lubrication to improve reliability.
My small confession: On one test day, I arrived late, stressed, and dehydrated. My results looked like my vision had resigned. The next test, calm and lubricated, looked stable. That was a 45-minute lesson in how fragile data can be.
Show me the nerdy details
In the US, common billing codes you may see include optic nerve OCT (often coded as 92133) and standard automated perimetry/visual field testing (often 92083). Codes vary by payer and country. The bigger point: ask what your clinic uses to track progression over time and how they confirm a real trend.
Scannable “better test day” checklist:
- Arrive 10 minutes early (stress changes everything).
- Use your usual dry-eye routine beforehand if allowed.
- Ask for a short break mid-test if tearing or burning spikes.
- Confirm which eye is tested first; fatigue matters.
Question 7: When is laser or surgery smarter than more drops?
If you have multiple eye diseases, the trade-offs change. More drops might worsen dry eye. Surgery might affect the surface, the lens, or the inflammation balance. And if you already have retinal care, scheduling and recovery windows matter a lot.
Ask: “At what point do you recommend laser or surgery for someone with my mix of conditions?” Follow with: “What is the realistic goal—fewer drops, lower pressure, or both?”
Also ask about sequence. If cataract surgery is likely soon, it can affect pressure and angle anatomy—especially if you’re still deciding cataract surgery one eye or both. If you have uveitis, inflammation control may be the gatekeeper before any procedure. If you have diabetic retinopathy, coordination between glaucoma and retina teams can prevent mixed messaging (and it helps to understand the basics of diabetic retinopathy if that diagnosis is in the mix).
Short Story: The day I stopped trying to be “easy” (120–180 words) …
At one visit, I tried to be the low-maintenance patient. I nodded. I smiled. I didn’t ask the “annoying” questions because the clinic was busy and I didn’t want to be a problem. Then I got home and realized I couldn’t explain the plan to my own partner in a single sentence. One drop changed, another stayed, and the next follow-up was “sometime.” I spent the next week doom-scrolling and second-guessing.
At the next appointment, I brought a one-page list: diagnoses, meds, side effects, and the one thing I feared most—progression. The doctor didn’t roll their eyes. They looked relieved. We clarified the target pressure, picked a measurable goal, and set a time window to reassess. The visit took maybe 6 minutes longer. It saved me weeks of mental static.
- Ask what success looks like at 1 month and 6 months.
- Ask how it affects your other eye disease monitoring.
- Ask what you’ll do if pressure rebounds.
Apply in 60 seconds: Write: “Goal = lower IOP / fewer meds / both” and circle one.
Question 8: How do my systemic health conditions change the plan, 2025?
Glaucoma care does not live in a bubble. If you have diabetes, hypertension, sleep apnea, autoimmune disease, migraines, asthma/COPD, or long-term steroid exposure, your “eye plan” may need guardrails.
Ask: “Which of my health conditions changes glaucoma risk, treatment choice, or monitoring?” Then: “Do any of my meds—especially steroids—affect pressure or inflammation?”
Here’s the time-poor version: your clinician can’t factor in what you don’t tell them. I once forgot to mention a short steroid course because it felt unrelated. It wasn’t. Pressure shifted, and we lost a clean baseline. (And if a new systemic medication is in the picture—especially something like a GLP-1 drug—bring it up plainly; this kind of “it feels unrelated” trap is exactly why topics like semaglutide and sudden vision loss in seniors get discussed at all.)
Two numbers that help you think like an operator:
- 72 hours: if a new drop causes severe pain, sudden vision change, or intense redness, don’t “wait it out.”
- 15 minutes: how long it takes to prepare a medication list that prevents mistakes.
Region note (Korea): If you’re in South Korea, you may be navigating National Health Insurance coverage, tertiary hospital referrals, and different appointment intervals than you’d see in the US. Ask your clinic whether OCT/visual field scheduling is bundled or separate, whether your prescriptions can be synchronized to reduce pharmacy runs, and whether you can get a printed “진료의뢰서/요약” style summary if you see both retina and glaucoma services. This can save 1–2 hours of repeat explanations across departments.
Show me the nerdy details
Systemic conditions can affect optic nerve perfusion, inflammation risk, medication tolerability, and surgical planning. The details are individualized, which is exactly why you ask the question: you want a plan that fits your whole body, not just your eye chart.
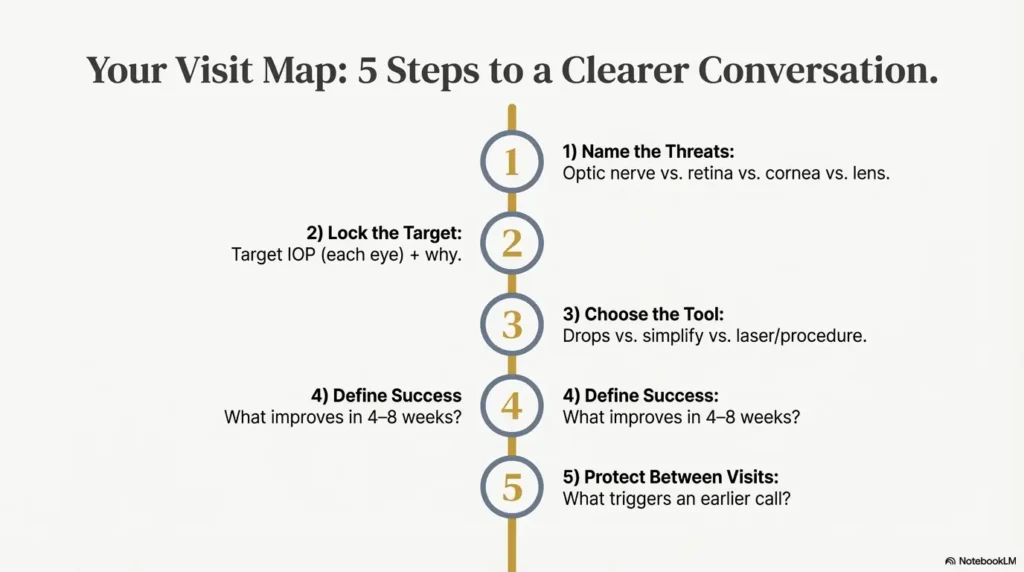
Question 9: What should I do between visits so we don’t lose months?
Most people lose ground between visits, not during them. Life happens. Drops get skipped. Symptoms get normalized. Records don’t move. And then the next visit becomes “catch up” instead of “protect vision.”
Ask: “What do you want me to track between now and the next appointment?” Then: “What would make you want to see me sooner?”
Tracking doesn’t need to be fancy. Two checkboxes per day is enough:
- Did I take my drops as prescribed?
- Any new symptom: pain, halos, sudden blur, new floaters, curtain, distortion?
My practical win: I started writing “missed dose” instead of pretending I’d remember. It reduced my guilt and improved the accuracy of the conversation. Weirdly, honesty saved time. About 10 minutes of “maybe” became 30 seconds of “here’s the pattern.” If you want something you can actually print (or hand to a family member without turning it into a “whole project”), use a printable symptom diary for seniors and keep it brutally simple.
Scannable “call sooner” list:
- Sudden severe eye pain, headache, nausea, or rainbow halos.
- Sudden drop in vision, a dark curtain, or new distortion.
- New flashes/floaters with vision changes (especially if you have retinal disease).
- Medication reaction that makes you stop drops.
Question 10: What will this cost me in time, money, and hassle—and how do I lower it?
This is the question many patients feel awkward asking. Don’t. Cost and friction drive adherence. And adherence drives outcomes.
Ask: “What is the simplest effective plan—fewest bottles, fewest daily steps—given my other eye diseases?” Then ask: “Are any of these meds likely to require prior authorization or be placed in a higher coverage tier?”
If you’re in the US, the words to know are: deductible, copay, coverage tiers, prior authorization, and your plan’s formulary. If you’re on Medicare Part D, plan choice can change medication affordability year to year. If you have private coverage, pharmacy benefit managers and step-therapy policies can add delays. This is not you being “difficult.” This is you preventing a two-week gap in treatment because paperwork moved at human speed. (If your clinician has already called you “high risk,” it’s worth knowing what Medicare recognizes as high risk—see high risk for glaucoma on Medicare.)
- Ask which options are usually easier to fill.
- Ask what to do if the pharmacy says “not covered.”
- Ask for the generic name and the class, not just the brand.
Apply in 60 seconds: Screenshot your insurance card (front/back) and store it with your med photos.
Coverage tier map (general, confirm with your plan):
Mini calculator (60 seconds): estimate annual “friction cost”
This is not medical advice—just a planning tool. Use it to justify simplifying your regimen.
Question 11: What is the one-page plan I should leave with today?
This is the “save me from chaos” question. Ask for the plan in a way you can follow when you’re tired, busy, and human.
Ask: “Can we write a one-page plan: diagnosis list, target pressure, meds (which eye, when), and the next test date?” Then: “What is the single biggest risk for me in the next 6 months?”
Also ask for coordination if you see multiple specialists: glaucoma, retina, cornea. Mixed disease means mixed teams. A one-page plan reduces contradictions like “increase steroid” versus “avoid steroid.”
I started doing this after one visit where two doctors told me two opposite things in the same week. Nobody was wrong; they were just looking at different threats. The one-page plan made the trade-off explicit.
Quote-prep list (what to gather before comparing coverage or refills):
- Medication names (generic + brand), dosage, and bottle size if known.
- Your plan details (deductible status, pharmacy network, prior authorization rules).
- Clinic notes or printouts (targets, last OCT/field dates).
- A list of intolerances (“this drop caused X within 3 days”).
Neutral next step: Save this list and confirm current coverage rules on your plan’s official portal.
FAQ
Q1) If I have glaucoma and dry eye, should I stop my drops when my eyes burn?
A: Don’t stop on your own. Burning can be a side effect, but pressure control matters. Call your clinic and ask about preservative-free options, spacing drops, or switching classes. Apply in 60 seconds: Write down which drop burns and how long it lasts after each dose.
Q2) Can cataracts make my visual field look worse even if glaucoma is stable?
A: Yes, cataracts can reduce clarity and test performance, which can lower visual field sensitivity. Ask your doctor whether your changes look like progression or optical noise. Apply in 60 seconds: Ask for your test reliability notes and whether the trend is confirmed on repeat testing.
Q3) I have diabetic retinopathy or macular degeneration—how do we tell what’s causing my vision changes?
A: You separate structure and function: retina imaging for the macula/retina and glaucoma monitoring for the optic nerve/field. Ask which finding changed, and which team owns it. Apply in 60 seconds: Bring a list of symptoms with timing (distortion vs blur vs blind spots).
Q4) When should I consider laser treatment instead of adding a third or fourth drop?
A: Consider it when you’re above target, struggling with side effects, or missing doses. The right time depends on your risk and your other eye conditions. Apply in 60 seconds: Count how many doses you take per day and share that number—honestly—at the visit.
Q5) What if my insurance denies a glaucoma medication or requires prior authorization?
A: Ask your clinic for an alternate in the same class, a step-therapy pathway, or a prior authorization submission plan. Coverage tiers and rules change. Apply in 60 seconds: Call your pharmacy and ask which tier your medication is in today.
Q6) How often should I be monitored if I have multiple eye diseases?
A: It varies by risk. The practical question is: what interval is safe for your optic nerve and your other condition’s activity? Ask for a schedule you can follow. Apply in 60 seconds: Ask your clinician to state your next test date out loud and write it down. (If you need a simple baseline for preventive care conversations, how often should seniors get dilated eye exams can help you frame the question.)
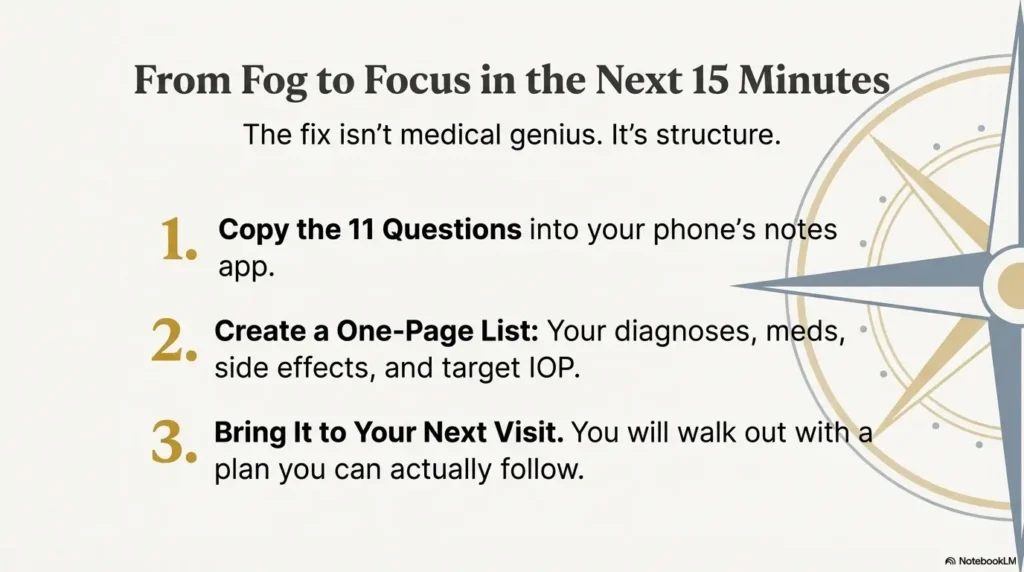
Conclusion: what to do in the next 15 minutes
Remember the hook—me leaving a visit with three new drops and zero clarity? The fix wasn’t medical genius. It was structure. Once I started asking for a target, a success metric, and a one-page plan, the fog lifted. Not because the disease got simpler, but because the plan did.
Your next step (15 minutes, tops): Copy the 11 questions into your notes app, run the 60-second “friction cost” estimator once, and create a one-page list: diagnoses, meds, side effects, and your target IOP. Bring that to your next visit. You’ll save 20–30 minutes of confusion—and you’ll walk out with a plan you can actually follow.
Last reviewed: 2025-12. Reviewed against major ophthalmology patient guidance and adult glaucoma management guidance, plus current prescription-coverage basics where relevant. If diabetes is part of your story, make sure you also understand Medicare glaucoma screening for diabetics so you can ask coverage questions without burning a whole afternoon.