

Navigating the SSA Vision Consultative Exam
The letter feels ordinary until you notice the subtext: one appointment can quietly decide whether your file moves—or stalls.
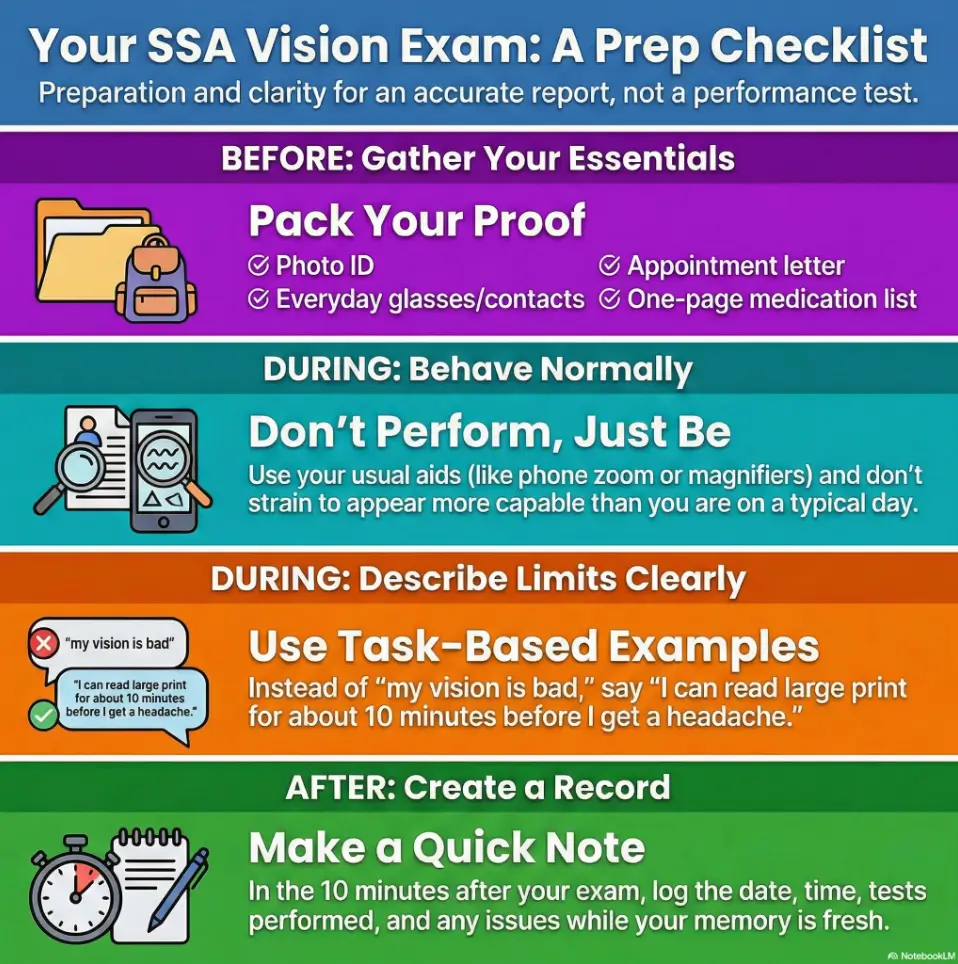
An SSA vision consultative exam (CE) checklist helps you show up as your typical self, not your bravest self and not your “best-day” version. Because the biggest risk isn’t saying something “wrong.” It’s walking in without the basics, leaving with results that don’t match how you actually function on a random Tuesday.
This post makes the day boring in the best way: what to bring, what they test, what gets observed (yes, even in the waiting room), and how to describe limits with task-based clarity.
Table of Contents
- Bring the right items so your results reflect your real-life functioning.
- Expect both testing and observation—yes, even the waiting room can matter.
- Use task-based examples instead of vague labels like “fine” or “terrible.”
Apply in 60 seconds: Put your glasses/contacts case and a one-page med list by your keys right now.
Vision CE purpose: why SSA ordered this exam
A consultative exam (CE) is an SSA/DDS tool for one simple problem: your file needs a current, specific measurement to move forward. That doesn’t mean your claim is doomed. It usually means the decision-maker can’t confidently answer one or two questions from your existing records.
The most common reasons are boring (in a good way): records are out of date, the notes don’t include the particular measurements SSA needs, or there’s a mismatch between what’s reported and what’s documented. If you’ve ever tried to explain a blurry photo to someone—“No, zoom in, the detail is right there!”—this is that, but with medical evidence.
Records gap triggers (not enough / not current)
- Missing measurements (for vision, fields and best corrected acuity are frequent culprits).
- Old testing that no longer reflects your current functioning.
- Inconsistency between providers or between symptoms and objective data.
- Specialized details that a general visit note simply doesn’t include.
Treating source vs independent examiner (what that means for you)
DDS often prefers a qualified treating source when possible, but it can also use an independent source if the treating provider can’t or won’t do the exam, if conflicts in the file can’t be resolved, or if another source is more practical for the needed test. In plain English: the person who examines you may not be “your eye doctor,” and that’s normal.
One small comfort: CE reports are not supposed to be a legal verdict. The examiner documents findings and function. They generally aren’t there to declare you “disabled” or “not disabled.” Your job is not to win an argument. Your job is to be a reliable narrator.
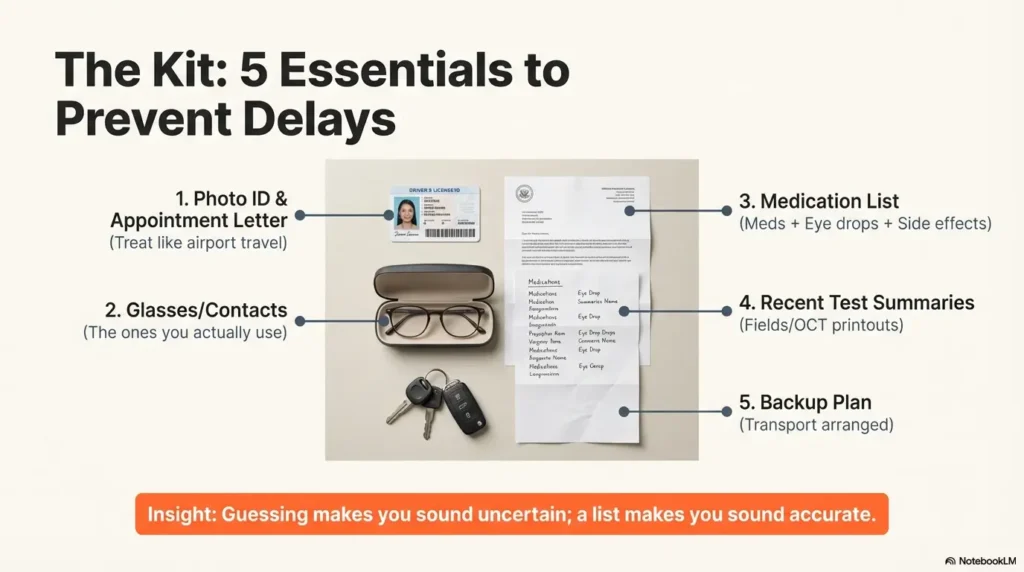
Bring-first checklist: the five items that prevent delays
The fastest way to sabotage a vision CE is accidentally making it a “best day” exam or a “stranded without my stuff” exam. We want your results to match typical functioning, because that’s what disability decisions are trying to measure.
1) Photo ID + appointment letter (non-negotiable)
Bring a current government photo ID and the letter. Not glamorous. Extremely effective. If you’re the kind of person who forgets paperwork, treat this like airport travel: wallet, phone, keys, letter.
2) Glasses/contacts you actually use (plus a backup plan)
Bring the corrective lenses you rely on day to day, not the “special occasion” pair you wear twice a year. If you wear contacts, bring your case and solution. If you switch between glasses and contacts, bring both.
3) Medication list (including eye drops + side effects)
Make a one-page list of meds, doses, and frequency. Include eye drops, injections, supplements, and any side effects you experience (dryness, headaches, dizziness). Guessing makes you sound uncertain; a list makes you sound accurate. Accuracy is the whole game here. If keeping meds straight is already hard because of print size or look-alike packaging, building your list using a low vision medication management system can make this step calmer and more consistent.
4) Recent eye testing summaries (fields/OCT/imaging if you have them)
If you have recent printouts or portal summaries for visual fields, OCT, or imaging notes, bring them. You may not need them, but when you do, you really do. Think of it as bringing an umbrella: it won’t cause rain, but it can save your day. If your vision history includes macular degeneration, it can help to know what “low vision care” typically covers—see what a low vision specialist does for macular degeneration.
5) Your “one-page timeline” (optional, quietly powerful)
On one page: onset, progression, procedures, and how your daily tasks changed. Keep it factual. This isn’t a memoir (even if your life deserves one). It’s a map that helps you answer quickly and consistently. If your symptoms began after a neurologic event, it can help to reference the pattern as vision loss after stroke so your timeline stays clear (what changed, when, and what never fully returned).
- Did you receive an official CE notice with date/time/location?
- Do you have a current photo ID ready?
- Do you have the glasses/contacts you normally use?
- Do you have a one-page med list (name/dose/frequency)?
- Do you have transportation arranged (and a backup)?
Neutral next action: If you answered “no” to any item, fix the easiest one today.
Vision CE tests: what they actually measure (not vibes)
Most consumer articles hand-wave this section with “they’ll test your vision.” That’s not helpful. A vision CE is built around specific measurements that can be compared, reviewed, and summarized in a report. Knowing the buckets helps you avoid two traps: (1) assuming the exam was “too easy” to matter, or (2) treating it like a stage audition.
Best corrected visual acuity (and why refraction matters)
“Best corrected” means your acuity is measured with the proper correction documented—not just “whatever you walked in wearing.” If you’ve ever had your glasses slightly off and thought, “I can manage,” you already know why this matters: managing is not the same as seeing.
Visual fields: confrontation first, then perimetry rules
Many exams start with confrontation fields (a simple check). If there’s a history of glaucoma or other field loss, or if confrontation isn’t normal, more formal field testing can be needed. In SSA guidance for CE report content, restricted fields should be confirmed with acceptable perimetry methods— including automated static threshold testing that measures the central 24 to 30 degrees, with common examples like Humphrey 24-2 or 30-2, or kinetic perimetry such as Goldmann.
Pupils + extraocular movements (double vision & tracking clues)
The exam may document pupil response and eye movements. This can matter for conditions involving diplopia (double vision), neurologic issues, or situations where tracking and coordination affect functional ability.
IOP, slit lamp, fundus exam (what they’re documenting)
Intraocular pressure (IOP) is relevant for glaucoma history. Slit lamp and fundus exams document structures like the cornea, lens, optic disc, vessels, macula, and peripheral retina. The goal is not to impress you with equipment. It’s to document findings in a standard way.
Show me the nerdy details
The “why” behind these tests is reporting reliability. A CE report is designed to let an independent reviewer understand severity and functional limits, and to reconcile subjective symptoms with objective findings. For vision cases, that often hinges on best corrected acuity plus fields, supported by documented methods and printouts where applicable. If the report is incomplete, DDS can send it back for missing pieces, which can delay decisions.
- Bring your everyday correction so results reflect your normal functioning.
- If you have a field-loss history, expect the possibility of formal perimetry.
- Don’t self-grade the exam based on how “hard” it felt.
Apply in 60 seconds: Write down your top 2 vision triggers (glare, low contrast, fatigue) on your phone notes.
Observed behaviors: what gets written down when you think it “doesn’t count”
Here’s the part that people learn too late: the CE report can include observed visual behaviors. Not in a creepy, “gotcha” way—more like the mundane notes a clinician makes without thinking: how you navigate, how you reach for objects, whether you’re using your phone comfortably, whether you need guidance in the space.
If that makes you tense, let me take the pressure down a notch: you don’t have to “act blind” or “act fine.” You just have to behave normally and describe your limits honestly. Normal is easier than performance. Normal is also more consistent.
Navigation, reaching, phone use—yes, it can appear in the report
Official guidance for adult CE report content for visual disorders includes examples like navigating the office, reaching for items handed to you, and using a cellphone in the waiting room. That doesn’t mean the examiner is hunting for contradictions. It means function is part of the picture. If your phone is one of your main coping tools, it’s worth knowing how to reduce glare and strain—many people use a way to make an iPhone screen dimmer than the minimum so “typical function” stays typical.
Curiosity gap: which tiny moments become “functional notes”?
Usually the tiny moments you don’t script: reading a sign, finding a doorway, recognizing a face at a normal distance, filling out a form, or adjusting to bright lighting. These are the moments your body answers before your mouth has time to be polite.
Here’s what no one tells you… the waiting room can be “data,” too
Waiting rooms are fluorescent, reflective, and full of small print. In other words: a greatest-hits album of visual triggers. If your vision gets worse with glare or low contrast, you don’t need to announce it like a town crier. Just note it if asked and stay consistent with your usual coping tools. If bright task lighting at home is a known trigger, you might recognize the same pattern in clinical spaces; practical fixes like glare-free under-cabinet lighting map surprisingly well to what “good lighting” means for real-world function.
Later, she realized the exam didn’t capture her typical functioning—it captured her pride. The second time around (yes, sometimes there’s a second appointment), she used her normal tools, described her triggers plainly, and let her pace be what it was. Same person, same condition—completely different clarity. That’s the lesson: the goal isn’t to suffer bravely. The goal is to be accurately understood.
Vision story that lands: how to describe limits without exaggerating
The fastest credibility leak is the phrase “It’s bad.” It’s not dishonest—it’s just useless. What helps is a simple structure that makes your symptoms legible: task → trigger → consequence. This isn’t “being coached.” This is being understandable.
Task-first language (reading, stairs, screens, faces, cooking)
Pick a handful of tasks that represent your day. Examples:
- Reading mail or medication labels (if labels are the bottleneck, see large-print prescription labels as a practical workaround you can mention as a coping tool)
- Using a computer or phone for more than a short period
- Stairs, curbs, and uneven sidewalks
- Recognizing faces at a normal conversational distance
- Cooking safely (timers, measuring, distinguishing similar items)
A quick anecdote that stays factual can help: “I stopped driving at night two months ago because glare from headlights makes lane markings disappear.” Notice how it’s specific without being theatrical.
Trigger map (glare, low contrast, fatigue, night, rain)
Triggers are often the missing link in medical records. Many people can “pass” a bright-room chart and still struggle in the real world. If your vision changes with lighting, contrast, or fatigue, say so in plain terms: what changes, how fast, and what you do to cope. If fatigue and screens are part of the picture, it can help to frame it like digital eye strain in seniors—not as a label, but as a pattern you can describe (time limits, symptom spike, recovery).
Open loop: the one sentence that keeps you consistent on good-day/bad-day
Try this: “My vision varies, but my limits show up reliably with these triggers, and this is what I can typically do on an average day.” Then name the triggers and tasks. That sentence keeps you anchored when nerves try to turn you into a philosopher.
Enter 3 numbers (rough estimates are fine):
- A: Minutes you can read small print before symptoms spike
- B: Minutes of travel time to the clinic (door to door)
- C: Hours it usually takes to recover after a visually demanding outing
Output: If B is long and C is high, plan your day like a battery: do the CE, then protect a recovery window. If A is short, bring your normal aids (zoom, magnifier, tinted overlay) so the day reflects how you actually function.
Neutral next action: Block recovery time on your calendar and arrange a ride if you’ll be depleted.
Common mistakes: the credibility leaks people don’t notice
Most people think the danger is “saying the wrong thing.” The more common danger is accidentally being unclear. Clarity isn’t just nice writing—here, it’s functional evidence.
Mistake #1: forgetting corrective lenses (creates “not typical” results)
If you normally use glasses or contacts and you show up without them, the exam may document your vision under conditions you do not actually live under. It’s like timing your mile with your shoelaces untied. Technically possible. Not representative.
Mistake #2: vague answers (“fine / terrible”) instead of examples
Replace labels with outcomes: “I can’t read” becomes “I can read large print for about 5–10 minutes, then I lose my place and get headaches.” “I’m okay walking” becomes “I use the handrail on stairs because I miss the edge in low light.” If night navigation is one of your hardest zones, it may help to think through it the same way you would a low-vision nighttime bathroom safety plan: task, lighting, contrast, fall risk, recovery.
Mistake #3: minimizing because you feel judged (accuracy > bravery)
Many time-poor, responsible adults default to minimization: “It’s not that bad, I manage.” Managing can be expensive. It can cost time, safety, errors, and recovery days. You’re allowed to describe that.
- Bring your everyday correction so your results represent typical function.
- Swap labels for task outcomes (time, errors, safety, fatigue).
- Describe coping tools without shame; tools are part of function.
Apply in 60 seconds: Write 2 task examples you can say in one breath.
Don’t do this: “helpful” moves that backfire in a vision CE
This is the section where I gently take your inner overachiever by the hand and say: “Sweetie, no.” A vision CE is not a character test. It’s not a pain tolerance contest. It’s not even a “how composed can I look” competition.
Don’t overcompensate (strain-reading the chart to look capable)
If you normally use tools—zoom, magnification, tinted lenses, screen readers—use them as you ordinarily do. Straining through tasks you can’t sustain can create a picture of functioning you cannot replicate in daily life. If you want one concrete “tool example” that doesn’t sound like a performance, something as simple as a giant print reading setup for macular degeneration illustrates the principle: you read when the format matches what your eyes can handle—then you stop when it doesn’t.
Don’t guess meds/dates—bring the list
Guessing is human. It also creates inconsistencies that live forever in paperwork. Your one-page list is your calm anchor. Bonus: it helps you answer faster, which lowers stress and makes you more consistent.
Let’s be honest… most people lose clarity, not credibility
The exam day is noisy: travel, fluorescent lighting, forms, new faces, pressure. Under stress, your brain turns sentences into soup. A tiny prep page (tasks, triggers, meds) keeps you from free-styling your history like it’s open mic night. If you’re the kind of person who remembers symptoms better when you can see them written down, a printable symptom diary for seniors can also help you capture patterns (how long, under what lighting, what recovery looks like) without relying on memory alone.
Who this is for / not for (so expectations don’t wreck your day)
A CE can feel insulting if you think it’s a replacement for your medical care. It’s not. It’s an evidence-gathering visit purchased to answer specific questions.
This is for
- SSDI/SSI applicants scheduled for an SSA/DDS vision CE
- People with field loss, acuity loss, fluctuating vision, or low-vision functioning issues
- Anyone whose records don’t include current measurements SSA needs
This is not for
- Getting a new prescription, treatment plan, or long-term care recommendations
- A deep relationship-based exam like you get with a long-time specialist
- Proving worthiness through suffering
One more human note: you can be a competent adult and still be disabled by vision limits. The goal isn’t to prove you’re helpless. The goal is to document the limits that show up even when you’re trying. If your home environment is part of your safety story (falls, missed steps, hazards you can’t see until they’re too close), a wet AMD home safety checklist is a helpful example of how “function” often lives in tiny, practical details.
Missed appointment risk: what happens if you don’t attend (and the fastest fix)
If you’re tempted to skip the CE because it feels pointless or overwhelming, pause. Missing a scheduled CE can stall your claim or force a decision based on an incomplete record. If you truly can’t attend, the best move is to reschedule quickly and document the reason.
SSA may decide using what they have—denial risk is real
The CE exists because the file needs something. If the “something” never arrives, the system may proceed without it. That’s not fairness; that’s bureaucracy. But we can plan for bureaucracy.
Reschedule path (document the reason; call immediately)
If illness, transportation failure, or another serious barrier prevents attendance, call the number on your notice as soon as possible. Keep a simple log: who you spoke to, date/time, what was said. If you need a language interpreter, DDS guidance notes interpreters can be provided at no charge when needed—ask early so the day doesn’t become chaos.
- You can safely travel and function with your normal aids.
- You have your ID, letter, and meds list ready.
- Skipping would mean weeks of delay and more stress.
- You have an unavoidable medical or transportation barrier.
- You can’t safely attend without essential aids/support.
- Language access or accommodations weren’t arranged in time.
Neutral next action: Choose one path and take one concrete step today (confirm attendance or request reschedule).
After the CE: your “receipt trail” in 10 minutes
When you walk out, you’ll be tempted to mentally toss the day into the ocean. Don’t. Give yourself 10 minutes to create a simple “receipt trail.” This isn’t about suspicion; it’s about protecting your memory while it’s fresh.
What to log: date/time/location, tests performed, unusual issues
- Date and time you arrived and left (round to the nearest 5 minutes)
- Clinic name/address (from the letter)
- What tests you remember (acuity, fields, dilation, etc.)
- Anything unusual (equipment issues, communication barriers, severe symptom flare)
Open loop: how to spot missing tests without sounding combative
If you expected certain testing because of your condition history (for example, known field loss) and you don’t think it happened, you don’t need to accuse anyone of wrongdoing. You simply note what occurred and keep your documentation tidy. If later you learn the report is missing key information, your calm notes help you communicate clearly with whoever is assisting your claim.
- Your CE appointment letter (photo or PDF)
- One-page meds list
- Two task examples + two triggers (written)
- Recent visual field/OCT summaries (if you have them)
- Post-CE receipt trail note (10 minutes)
Neutral next action: Put these in one folder (paper or digital) so you’re not hunting later.
Safety / Disclaimer + when to seek urgent help
This article is educational and isn’t legal or medical advice. Exam steps can vary by state agency and clinic. If you’re unsure what to bring, call the number on your appointment notice and ask what they require.
And because vision is high-stakes: if you have sudden vision loss, severe eye pain, or new flashes/floaters with a curtain-like shadow, seek urgent medical care. Claim logistics can wait; your eyes can’t.
FAQ
It’s an exam SSA/DDS purchases when your file needs current, specific evidence to decide your claim. For vision cases, that often means measurements like best corrected acuity and visual fields, plus functional observations.
Common buckets include best corrected visual acuity, visual field evaluation (sometimes with perimetry if needed), eye movement checks, and ocular health documentation such as intraocular pressure, slit lamp findings, and fundus exam details.
Bring and use what you normally rely on. If you switch between contacts and glasses, bring both with your normal care items. The goal is for testing and observations to reflect your typical daily functioning, not a one-off scenario.
The report can include observed visual behaviors. Don’t panic—just be normal. Use your usual tools and pace. If you struggle with glare, low contrast, or fatigue, describe that plainly when asked.
Not always. Some visits start with a basic field screen. If there’s known or suspected field loss, more formal perimetry may be needed. The exact workflow varies by clinic and what DDS requested.
Yes—bring what you have, especially recent field tests or imaging summaries. You may not need them, but they can help prevent gaps and misunderstandings when your condition is complex or changing.
Usually it’s a sign that the file needs one more piece of evidence—often measurements—before a decision can be made. Treat it like a documentation step, not a verdict.
Missing it can delay your claim or lead to a decision based on incomplete information. If you can’t attend, request rescheduling as soon as possible and keep a simple record of your calls.
It varies by clinic and testing needs. Many are relatively short, but a visit can run longer if additional measurements are required. Plan for extra time anyway so you’re not rushing.
Typically, no. The examiner documents findings; the disability decision is made by SSA/DDS after reviewing the full record.
Conclusion + next step: walk in ready, leave a trail
Let’s close the loop from the beginning: what do they “actually test”? They test measurements—acuity and often fields—and they document function through observation and your description. The win is not “doing well.” The win is being accurately understood.
If you do one thing, do this: bring your normal correction, bring your med list, and show up as your everyday self. Not your bravest self. Not your most polished self. Your typical self—the one who has to live with this on Tuesday, not just survive an appointment on Thursday.
Next step (15 minutes): build your one-page “Vision Limits Snapshot”
- Top 5 task failures: reading labels, stairs, screens, faces, cooking—choose yours.
- Top 3 triggers: glare, low contrast, fatigue, night, rain—choose yours.
- Your tools: glasses/contacts, magnifier, zoom, tinted lenses, screen reader—what you actually use.
- Your meds list: name, dose, frequency, side effects you notice.
- Key dates: onset, major changes, procedures, recent tests.
- ID + appointment letter in one folder
- Glasses/contacts + backup items
- One-page meds list
- 2 tasks + 2 triggers written down
- Use normal aids and pace
- Answer with task → trigger → consequence
- Stay consistent on “average day” functioning
- Don’t self-grade the exam
- Write your receipt trail note
- List tests you remember
- Log any severe flare or barriers
- Protect recovery time
- Typical functioning beats “best day” or “hero day.”
- Clarity protects you when nerves try to scramble details.
- A 10-minute receipt trail can save hours later.
Apply in 60 seconds: Start the Vision Limits Snapshot with just two bullet points—one task, one trigger.
Last reviewed: 2026-01