

The Medicare Cataract Myth: Navigating Post-Surgery Vision Costs
“Free glasses after cataract surgery” is one of Medicare’s most expensive myths—because the real costs hide in premium lens upgrades and paperwork, not the surgery itself.
If you’re trying to pin down Medicare cataract surgery glasses coverage, you’re probably stuck between two voices: the plan language that sounds clean, and the optical counter that turns it into a checkout surprise. The confusion spikes when someone says “one pair per eye” and you assume that means progressives, premium frames, or a backup pair.
Keep guessing and you risk either overpaying fast—or getting a denial that feels final when it’s really a routing problem.
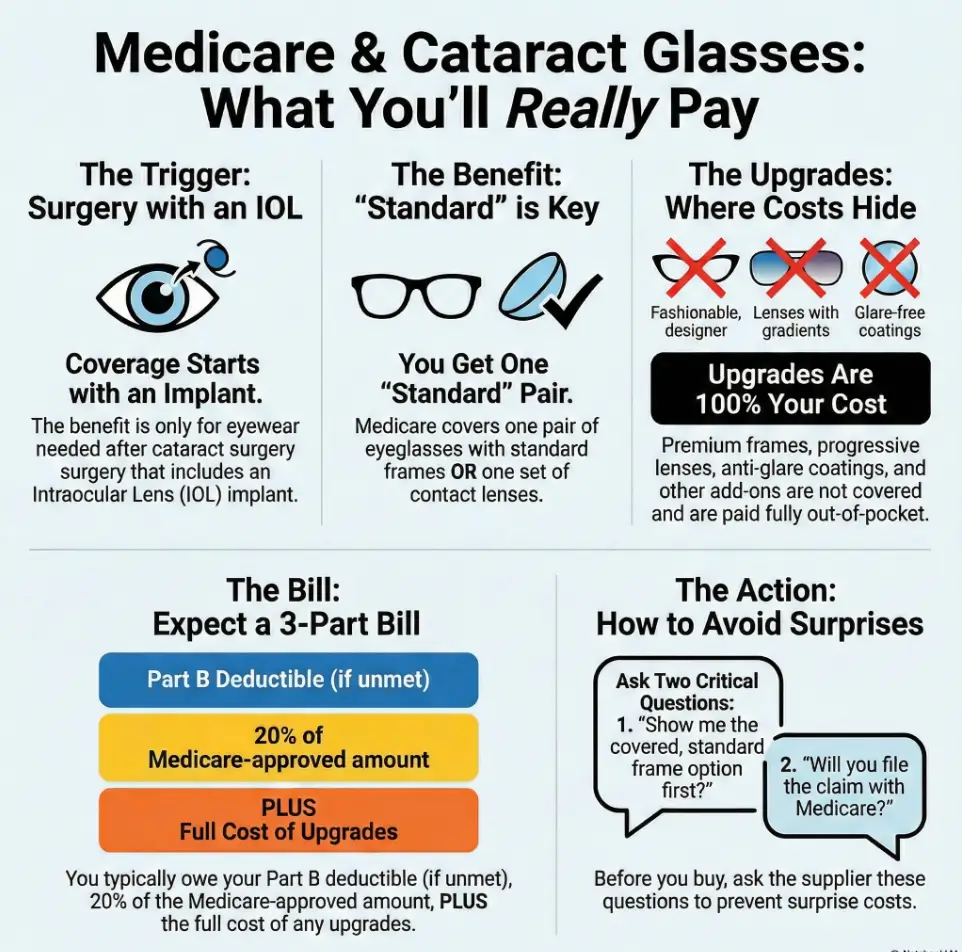
Under Medicare Part B cataract surgery coverage, after cataract surgery with an intraocular lens (IOL) implant, Medicare generally covers one pair of eyeglasses with standard frames or one set of contact lenses. You may still owe your deductible, 20% coinsurance, and the full cost of upgrades (progressives, AR coating, photochromic, premium frames).
This guide uses an operator-style method: confirm the trigger, control timing (especially with two eyes), and force itemized pricing before you say yes.
BEFORE YOU SIGN.
BEFORE THE “COVERED” LINE TURNS INTO A BILL.
Table of Contents
Medicare trigger: “after IOL” (not “after cataracts”)
Most confusion starts with one tiny word: after. Medicare’s eyewear benefit isn’t “because you had cataracts.” It’s tied to a specific scenario: cataract surgery with an intraocular lens implant (IOL). Medicare’s own coverage explanations (and reputable Medicare educators like Medicare Interactive) point to this as a narrow exception to routine vision coverage.
Here’s the scene that repeats: someone gets a beautiful surgery outcome, walks into an optician, says, “Medicare covers my glasses,” and the optician replies, “Sure—if the paperwork matches.” That last part is where bills are born.
- Ask the surgeon’s billing office to confirm the IOL was implanted.
- Ask how they document the post-cataract eyewear benefit.
- Buy only after you know who files the claim and how.
Apply in 60 seconds: Write down your surgery date(s) and whether you’re doing one eye or both—this changes the strategy.
The qualifying event: cataract extraction with IOL implantation
In plain English: Medicare’s eyewear exception is meant for the vision correction you need because a lens was implanted during cataract surgery. That’s why the benefit is often described as post-cataract eyewear “following IOL implantation.”
Curiosity gap: the one line on your surgery note that decides “covered vs denied”
If you remember one operator move, make it this: ask the billing office what the record will show for the procedure and the implanted lens. Not because you want to argue coding (you don’t), but because denials often happen when the claim can’t be matched to the right documented event. It’s the difference between “this is the cataract/IOL eyewear exception” and “this looks like routine glasses.”
What “one pair per eye” means (and what it doesn’t)
The phrase “one pair per eye” is helpful… until it isn’t. Think of it as shorthand: after surgery on an eye with an IOL implant, Medicare generally covers one of the following for that eye’s post-op correction: one pair of eyeglasses with standard frames or one set of contact lenses.
What it does not automatically mean: you get two designer frames, or progressives, or “a backup pair,” or “whatever the optical shop recommends.” Medicare’s benefit is narrow; the sales floor is wide.
Money Block: Eligibility checklist (yes/no)
- Yes — You had (or will have) cataract surgery with an IOL implant.
- Yes — You need post-op correction (glasses or contacts).
- Yes — You can use a supplier who can handle Medicare rules/claims.
- No / Not sure — You’re relying on routine vision benefits (that’s a different bucket).
Neutral next step: Call the surgeon’s billing office and ask what documentation will support post-cataract eyewear coverage.
Covered eyewear: “standard frames” in real life
The words standard frames sound like a neutral description. In practice, they’re a boundary. The optical shop’s “standard” and Medicare’s “standard” are not always the same species.
Here’s a little truth most people learn the hard way: “covered” usually means “covered at the base level.” The moment you pick the nicer thing—thinner lens, better coating, progressives—your out-of-pocket grows quietly, then suddenly.
Standard frames vs “what the shop defaults to”
Many optical shops start you in the upgrade lane. It’s not malicious; it’s just retail gravity. The frame wall you’re shown first is rarely the cheapest wall. If your goal is to use the Medicare benefit cleanly, you’ll want to ask, early and plainly: “Show me what counts as the covered standard frame option.”
Lenses: what’s usually included vs typically upgraded
Medicare’s post-cataract eyewear benefit is generally described in terms of basic correction. Upgrades often include: progressive/multifocal designs, high-index thinning, anti-reflective coating, photochromic (“Transitions-style”) lenses, blue-light filters, premium scratch protection packages, tinting, and premium lens upgrades.
You may want some upgrades! The goal isn’t to shame upgrades. It’s to make them intentional. A $0 base benefit with a $400 upgrade bundle is still a $400 decision—so treat it like one.
Here’s what no one tells you… “free glasses” can still cost you a lot
If a shop says “Medicare covers your glasses,” your next sentence should be: “Great—what’s the covered option without upgrades, and what do upgrades add?”
- Ask for a base quote first (covered option).
- Then add upgrades one-by-one.
- Stop when the price stops making sense.
Apply in 60 seconds: Request an itemized estimate that separates “covered base” from “upgrade add-ons.”
What you’ll pay: deductible + 20% + upgrades (the 3-part bill)
Let’s talk money with adult honesty, but without fake precision. Medicare cost-sharing is real: even when something is “covered,” you may still owe your Part B deductible (if it applies for you) and typically 20% coinsurance. Then come the upgrades, which are where most of the surprise lives.
Think of your cataract surgery bill as three layers: (1) Medicare rules, (2) your cost-sharing, and (3) your choices. Only the third layer is fully in your control—so we’ll make it easy to control.
The Part B cost structure (deductible, coinsurance)
Medicare Part B commonly involves a deductible and coinsurance. If you haven’t met your deductible, the first slice comes from you. After that, the coinsurance structure often means you pay a percentage of the Medicare-approved amount. If you have Medigap (Medicare Supplement) or other coverage, your out-of-pocket may be lower—but you have to confirm the exact mix.
Upgrade “price multipliers”: progressives, high-index, AR, photochromic
Upgrades don’t feel like big choices because they’re framed as “comfort.” But even one upgrade can stack: progressives + high-index + AR coating + photochromic can turn into a bundle. If you’ve ever seen a receipt where the base item is modest and the add-ons look like a restaurant bill, you understand.
A practical trick: decide your top one upgrade before you shop. For many people, AR coating is the “most felt” day-to-day upgrade. For others, it’s thinner lenses for comfort. Pick your hill. Don’t die on every hill.
Curiosity gap: why the lowest quote can become the highest checkout
The cheapest-sounding offer often hides the most aggressive upgrade path. “Covered glasses” is the headline; “premium digital progressive package” is the fine print. The fix is boring and powerful: itemize, slow down, decide.
Money Block: Mini calculator (quick estimate)
Mini calculator: Estimate your likely out-of-pocket for eyewear (very rough).
Note: This ignores deductible status and any Medigap/secondary insurance. Use it only to compare upgrade choices.
Neutral next step: Ask for the “covered base” estimate and then re-run the numbers with your preferred upgrades.
Timing rules: when to order so you don’t waste the benefit
The timing mistake is common because it feels responsible: “I’ll handle my glasses right away.” The problem is that your prescription can change as your eye heals. A rushed purchase can turn into a second purchase—especially if you’re doing both eyes on different dates.
If you’re someone who hates making phone calls, this section is your “make one call now, skip three later” moment.
Healing reality: why prescriptions can shift early on
After cataract surgery, your vision may stabilize over time. Your surgeon will guide you on when a final prescription is appropriate. The practical point: avoid committing to expensive upgrades before your eye is ready—and keep simple comfort tools (like preservative-free tears after cataract surgery) on your radar if dryness flares during recovery.
Provider + timing: why “wrong prescriber / wrong timing” triggers denials
Denials often don’t happen because you did something “wrong” morally. They happen because the claim doesn’t match the expected pattern. If the provider documentation doesn’t line up (or the eyewear is billed as routine rather than post-cataract/IOL), it can get kicked back. The fix is to confirm the workflow: who writes the prescription, who supplies the eyewear, and who files the claim.
Micro-check at your follow-up: 3 questions to ask before shopping
- “Is my vision stable enough for a final prescription?”
- “Should I wait because my second eye is scheduled soon?”
- “What’s the cleanest way for the optical supplier to file the post-cataract benefit?”
Show me the nerdy details
Post-op visual outcomes can shift as inflammation resolves and the eye adapts to the implanted lens. That’s why many surgeons time refraction and final prescriptions around follow-up milestones. The “best” timing isn’t one-size-fits-all—so treat your surgeon’s timeline as the primary authority for your eyes.

Two-eye strategy: don’t lose a benefit between Eye #1 and Eye #2
If you’re planning cataract surgery: one eye or both (often staged), this is where people accidentally pay twice. Not because they’re careless—because nobody explains the strategy in a way that matches real life.
Here’s the uncomfortable truth: your first eye may feel amazing, and your second eye may still be foggy. That “in-between” period is where many people buy glasses, then buy again. If you want to protect your budget, treat the two-eye plan like a project with a timeline, not a shopping trip.
The “both eyes, staged” scenario—why it’s the most expensive mistake
A common scenario: Eye #1 is done, the world turns HD, and suddenly your old glasses feel wrong. You buy a shiny new pair. Then Eye #2 is done, your prescription shifts again, and the shiny new pair becomes the “backup pair.” The backup pair is nice. The unplanned payment is not.
The overlooked rule: if you don’t get eyewear between surgeries, coverage may land only after the second
Some billing/coverage discussions emphasize that the benefit is tied to the post-op correction for an eye. In practice, the safest approach is to ask the surgeon’s billing office how they recommend timing eyewear purchases if you’re doing both eyes. If you plan to wait, confirm that the post-op eyewear claim will be filed cleanly after the appropriate visit.
Let’s be honest… the optical shop won’t manage your timing—you have to
Optical staff are usually helpful, but they aren’t your project manager. Your job is to bring the plan: “I’m doing Eye #2 on [date]. I want the most cost-effective approach.” Then ask them to quote two options: a minimal interim solution vs your final pair.
Money Block: Decision card (When A vs B)
Decision card: Should you buy glasses after Eye #1?
- Choose “Wait for Eye #2” if Eye #2 is soon, your current glasses are tolerable, and you want to avoid buying twice.
- Choose “Interim fix” if you must drive/work safely now and your vision mismatch is causing headaches or unsafe blur.
- Choose “Final pair now” only if your surgeon says your prescription is stable enough and Eye #2 timing won’t disrupt it.
Neutral next step: Ask for both an interim quote and a final quote before you decide.
Supplier rules: where you buy matters more than people expect
This section is unglamorous, but it saves real money. Some denials are caused by one thing: the supplier can’t (or won’t) file the claim correctly under Medicare rules. The patient hears “not covered,” pays out of pocket, and later learns it might have been covered if routed differently.
You don’t have to become a billing expert. You just have to ask two questions that force clarity.
Medicare pays only through Medicare-enrolled suppliers (what to verify)
Medicare coverage is not just “what is covered,” but also “who can bill it.” Ask the optical supplier if they are Medicare-enrolled and if they will file the claim for post-cataract eyewear. If the answer is vague, treat it as a “no” until proven otherwise.
Denial trigger: when the claim can’t be processed because it’s routed wrong
A denial can be as simple as: the claim doesn’t match the expected category, or paperwork isn’t attached in the way the payer expects. This is why the safest workflow is to confirm the claim filing path before you order.
The DME angle (why some post-cataract eyewear claims behave differently)
Post-cataract eyewear coverage is sometimes discussed alongside durable medical equipment (DME) concepts because it has a “medical benefit” flavor rather than routine vision. You don’t need to memorize categories; you just need to ensure the supplier knows how it’s billed and that they’ll do it.
Money Block: Supplier verification checklist
- “Are you Medicare-enrolled as a supplier?”
- “Will you file the post-cataract eyewear claim?”
- “Can you show the estimate with the covered base separated from upgrades?”
- “What documentation do you need from my surgeon?”
- “If it’s denied, what is your process for correcting and resubmitting?”
Neutral next step: If you can’t get clear answers, shop for a supplier who can.
If you want the official framing in Medicare’s own language, this page is a good reference point:
Plan type split: Original Medicare vs Medicare Advantage (same surgery, different friction)
Two people can have the same surgery and wildly different eyewear experiences because they’re in different plan structures. Original Medicare (Part B) tends to be more standardized in how benefits are described. Medicare Advantage (Part C) can add extra vision perks—but often adds network rules, authorizations, or vendor requirements.
This is where caregivers earn their keep. One phone call to the plan can save a week of “why is this being denied?”
Original Medicare: consistent rules, narrow benefit
With Original Medicare, the post-cataract eyewear benefit is typically described as a specific exception with clear boundaries. It’s not a broad vision plan. It’s a narrow post-surgery benefit.
Medicare Advantage: possible extra vision perks, but more gatekeeping
Medicare Advantage plans may include routine vision allowances, networks, and preferred vendors. That can be great—if you use the right channel. It can also be frustrating if you assume it works like Original Medicare and buy from an out-of-network supplier.
Curiosity gap: the one question that reveals whether “vision benefits” are real (or marketing)
Ask your plan this exact question: “For post-cataract eyewear, do I have to use a specific in-network optical supplier or vendor, and do I need prior authorization?” If they can’t answer quickly, ask to be routed to the department that handles vision benefits.
- Confirm network/vendor requirements before you order.
- Ask about prior authorization (even if it sounds annoying).
- Get the representative’s name and reference number if available.
Apply in 60 seconds: Write down your plan type (Original + Medigap vs Advantage) at the top of your notes before making calls.
Premium IOL twist: when “upgrade lenses” collide with coverage
If you’re choosing an IOL (or already chose one), you deserve a calm explanation of what’s realistic. Premium IOL options—like toric or multifocal designs—can be valuable. They can also introduce cost and documentation complexity. Coverage discussions may separate what’s medically necessary from what’s elective.
Here’s the practical framing: paying more for an IOL doesn’t automatically mean you won’t need glasses. Some people still need correction for reading, night driving, or fine detail. So the smart move is to plan for eyewear as a possible “Phase 2,” not as a failure.
Premium IOLs are often treated as elective—coverage can get harder
Many coverage frameworks treat certain enhancements as elective upgrades. That can affect what the plan pays for and how claims are processed. The safest play is not to assume; it’s to ask your surgeon’s office how your choices might affect post-op correction needs and billing. If you’re weighing lens types, a side-by-side guide to monofocal vs multifocal vs toric IOL options can make the tradeoffs feel less foggy.
Exception pathways: “medical necessity” and why documentation becomes the whole game
“Medical necessity” is not a magic phrase. It’s a documentation standard. If a plan requires additional justification for certain items, you want that conversation before money changes hands. In optometry billing circles, the American Optometric Association’s coding guidance is often referenced by clinics trying to file correctly.
If you’re choosing an IOL today, read this section first.
Ask two questions while you’re still in decision mode: (1) What visual tasks do I care about most—reading, night driving, screen work? (2) If I still need glasses after, what’s the simplest path to get the covered base option? These questions keep your choices aligned with your life and your budget.
Who this is for / not for (quick eligibility filter)
Let’s save you time. If you’re not in the narrow exception, you shouldn’t waste energy trying to squeeze Medicare into being a routine vision plan. If you are in the exception, you shouldn’t overpay out of confusion.
For you if: cataract surgery + IOL + you need corrective lenses after
If you’re having cataract surgery with an IOL implant and you expect to need glasses or contacts for best vision after, you’re the person Medicare’s exception is meant to help.
Not for you if: you want routine eyewear coverage without surgery
Routine glasses are generally not a broad Medicare benefit. Many people use Medicare Advantage vision allowances or separate vision plans for routine eyewear. Don’t let the post-cataract exception trick you into thinking routine coverage is hiding somewhere.
Edge cases: Medigap, Medicaid, retiree plans, dual eligibility
This is where the math can improve. If you have Medigap (supplemental insurance), retiree coverage, or Medicaid (dual eligibility), your coinsurance may be reduced or handled differently. The only safe statement is: it depends—so confirm your specific coordination of benefits. And if diabetes is part of your medical picture, planning can look a little different—especially around timing and follow-ups—so it’s worth reviewing cataract surgery for diabetics considerations with your care team.
Common mistakes: 9 ways people accidentally overpay (or get denied)
Think of this list as your “preventable losses” section. Not because you’re careless—but because this system rewards people who ask one extra question.
Mistake #1: assuming progressives or premium frames are included
This is the classic: you hear “covered,” you choose progressives, and you meet a bill. Upgrades are fine. Unplanned upgrades are not.
Mistake #2: ordering from a supplier who can’t file the claim
If the supplier can’t bill Medicare properly, you may end up paying out of pocket even when the benefit exists.
Mistake #3: missing the timing window or ordering before your prescription stabilizes
The early prescription can shift. That’s biology, not bad luck.
Mistake #4: treating Medicare Advantage rules like Original Medicare
Advantage plans may require network vendors or authorizations. Confirm first. Buy second.
Mistake #5: doing Eye #1 and Eye #2 without a plan (and paying twice)
The staged-surgery period is a budget trap. Decide in advance: wait, interim fix, or final pair now.
Mistake #6: not getting an itemized estimate before you say “yes”
Itemization turns confusion into choice. Without it, you’re shopping blind.
Mistake #7: not asking how the claim is filed (routing blind spot)
You don’t need coding mastery. You need the workflow: who files, what documentation is needed, and what happens if denied.
Mistake #8: assuming vision insurance stacks cleanly with Medicare
Sometimes it does. Sometimes it doesn’t. Ask both payers how coordination works before you commit.
Mistake #9: waiting until after denial to gather documentation
The best time to get clarity is before you order. The second-best time is immediately after you sense confusion.
- Base quote first.
- Upgrades one-by-one.
- Confirm who files the claim before ordering.
Apply in 60 seconds: Ask for an estimate that shows “covered base” and “upgrades” on separate lines.
When to seek help: medical red flags + billing escalation paths
This is the part nobody wants to read—until they need it. Most cataract recoveries go smoothly, but it helps to know the warning signs of cataract surgery complications in seniors—and if you experience alarming symptoms, don’t “wait it out” because you’re busy. And if your claim is denied, don’t assume denial equals truth. Sometimes denial equals missing paperwork.
Urgent symptoms after cataract surgery: call your surgeon promptly
If you have severe pain, sudden vision loss, or new flashes/floaters, contact your surgeon’s office right away or seek urgent care as directed. Your eyes are not the place to be brave.
Coverage disputes: provider billing office → plan member services → Medicare support resources
For coverage issues, start where the documentation lives: the surgeon’s billing office. Then call your plan’s member services (or Medicare if you’re in Original Medicare). If you need help understanding options, many states have SHIP (State Health Insurance Assistance Program) counselors who can help explain plan rules.
If you’re stuck: benefits counseling options (what they can actually do)
A counselor can help you interpret benefits, appeal pathways, and coordination of coverage. They usually can’t override a plan’s rules—but they can help you present your case clearly, which matters more than people think.
FAQ
Does Medicare cover glasses after cataract surgery?
Medicare Part B generally covers a limited eyewear benefit after cataract surgery with an intraocular lens (IOL) implant—often described as one pair of eyeglasses with standard frames or one set of contact lenses. Your cost-sharing and upgrades can still create out-of-pocket costs.
Is it really “one pair per eye,” or one pair total?
The common shorthand is “one pair per eye,” tied to the post-op correction after surgery on an eye with an IOL implant. But real-world rules can hinge on timing, documentation, and plan type—so confirm with your surgeon’s billing office and your plan, especially if you’re doing both eyes.
Does Medicare cover progressive lenses after cataract surgery?
Progressives are often treated as an upgrade. Medicare’s covered option is typically the basic correction; progressives and other premium lens designs frequently add cost. Ask for a base quote first, then price the progressive upgrade separately.
Are premium or designer frames covered?
The “standard frames” wording generally points to a basic frame option. Premium/designer frames usually add cost. The best approach is to ask the optical supplier to show you the covered standard frame selection and then price upgrades openly.
Can I choose contacts instead of glasses after cataract surgery?
The post-cataract benefit is often described as either glasses with standard frames or one set of contact lenses. Whether contacts make sense depends on your eyes, your habits, and what your provider recommends. Confirm both clinical suitability and plan rules before ordering.
Do I have to buy from my surgeon’s office, or can I use an outside optician?
You may be able to use an outside optician, but the supplier’s ability to handle Medicare billing and documentation matters. Ask the supplier if they are Medicare-enrolled and whether they will file the post-cataract eyewear claim.
What if my optical shop says nothing is covered?
Don’t assume that’s the final answer. Ask: “Are you Medicare-enrolled, and do you file the post-cataract eyewear claim?” Then verify with your surgeon’s billing office that your surgery documentation supports the post-cataract eyewear benefit.
What if I chose a premium IOL and still need glasses?
Needing glasses after a premium IOL isn’t automatically a problem—it can be normal for certain tasks. Coverage and billing can be more complex, so ask your surgeon’s office how they recommend documenting and routing post-op correction needs, and request an itemized eyewear estimate.
When should I order glasses if my second eye surgery is scheduled soon?
This is a strategy decision. If Eye #2 is soon, you may choose to wait for a more stable prescription, or use an interim solution if safety/work demands it. Ask your surgeon when a final prescription is appropriate and get both interim and final quotes if needed.

Close the loop: your “one pair per eye” plan in 15 minutes
Remember the curiosity loop from the beginning—the fear that “covered” would turn into a surprise bill? Here’s the honest closure: the benefit is real, but it’s narrow. Your savings come from routing and choices, not from hoping Medicare behaves like a full vision plan.
Short Story: The receipt that almost doubled (120–180 words) …
Short Story: A caregiver named Lena had Eye #1 scheduled on a Tuesday and Eye #2 two weeks later. After the first surgery, her dad felt euphoric—“I can read street signs again!”—and the old glasses suddenly felt crooked and wrong. They went to an optical shop that said, “Medicare covers it,” and offered a premium package with progressives and coatings. Lena hesitated and asked for an itemized base quote.
The base option was modest; the upgrades were most of the bill. She made one more call to the surgeon’s billing office and learned the prescription could shift after Eye #2. They chose a minimal interim fix, waited for the second eye, then used the benefit cleanly for the final pair. The “surprise” didn’t vanish by magic—it vanished because Lena slowed down for ten minutes and forced the numbers into daylight. …
Your 15-minute action plan (the calm version)
- Write down your plan type (Original Medicare vs Medicare Advantage) and whether you’re doing one eye or both.
- Call the surgeon’s billing office and ask: “Was an IOL implanted, and how should I time eyewear if I’m doing both eyes?”
- Call the optical supplier and ask: “Are you Medicare-enrolled, and will you file the post-cataract eyewear claim?”
- Request an itemized estimate showing covered base vs upgrades.
- “Will you file the claim?”
- “Show me the covered base option first.”
- Then upgrade intentionally.
Apply in 60 seconds: Put “covered base first” at the top of your notes before your optical appointment.
Infographic: The “One Pair Per Eye” reality check
Step 1: Trigger
Cataract surgery with IOL implant → unlocks narrow eyewear exception.
Step 2: Covered base
Typically standard frames (or contacts) + basic correction.
Step 3: Your bill comes from
Deductible (if applicable) + 20% coinsurance + upgrades.
Operator tip: If any box feels uncertain, you’re not behind—you’re early. Confirm the workflow before you buy.
If you want a trusted Medicare educator’s explanation of cataract coverage (helpful for plan conversations), this page is a solid reference:
And if you want a clinic-facing view of how optometry offices think about billing and coding for post-cataract eyewear, the American Optometric Association’s guidance can clarify why the paperwork matters:
Last reviewed: 2026-01. If you’re also planning the practical side of recovery—lighting, routines, and reducing “oops” moments at home—this guide to the best home setup after cataract surgery can help. And when you’re thinking about real-life milestones like driving after cataract surgery, treat your surgeon’s guidance as the final authority.