


Protect Your Vision: Navigating Medicare Step Therapy for Wet AMD
One missing detail in a prior-auth packet can turn a “routine” wet AMD injection into a two-week scheduling slip—and your eyesight doesn’t care that the delay was caused by a fax queue.
If you’re dealing with Medicare Advantage step therapy, the stress usually isn’t the needle. It’s the phone tag, the “pending review,” and the appointment date that keeps drifting while everyone swears it’s “just paperwork.”
Keep guessing, and the real loss isn’t convenience—it’s time-to-treatment (the part you protect by defending the wet AMD injection schedule like it’s part of care).
Access Mechanics
- Understand “Avastin first” protocols
- Billing differences for Eylea & Vabysmo
- Documentation triggers & status words
Protection Strategies
- Escalation paths clinics use daily
- Original Medicare vs. Medigap friction
- How to identify where delays hide
This guide helps you protect the calendar and keep “pending” from becoming your new schedule.
Table of Contents
Safety / Disclaimer (read first)
This article is general education, not medical or legal advice. Wet AMD is time-sensitive, and your best guidance comes from your retina specialist and your plan’s written materials. Insurance rules can differ by state, plan type, and whether your treatment is billed in a clinic, hospital outpatient department, or another setting.
If you’re choosing between drugs (Avastin, Eylea, Vabysmo), that is a medical decision. What we’ll do here is focus on access mechanics: step therapy, prior authorization, documentation, and what Medigap can change (mostly your out-of-pocket share and plan restrictions).
- Step therapy is about sequence (what first), not your doctor’s skill.
- Delays are the real risk—treat the calendar like part of treatment.
- Medigap can reduce cost stress, but it can’t replace good documentation.
Apply in 60 seconds: Put your next injection date and “authorization status” in one note on your phone.
When to seek help (don’t wait)
- Sudden vision changes, new distortion (straight lines look wavy), a dark spot, rapid blur: contact your retina clinic urgently.
- If treatment is being delayed due to authorization/step therapy: ask your clinic about expedited/urgent review and whether delaying injections could risk vision.
- If you can’t reach the clinic and symptoms feel scary: use urgent care guidance your clinic provided or seek emergency help per local instructions.
A common scene: someone says, “It’s just paperwork,” and weeks later they realize the paperwork quietly became a delay. Your eyes deserve a faster escalation path than “we’ll call you back.”
1) Step therapy—what it really changes (and what it doesn’t)
What “step therapy” means in plain English (injection path vs paperwork path)
Step therapy is a plan rule that can require trying a plan-preferred medication first before another is covered—often framed as “start with the most cost-effective option.” In the wet AMD world, this can look like “Avastin first,” then moving to Eylea or Vabysmo if needed.
Here’s the key: step therapy often changes paperwork more than medicine. The injection still happens in a retina clinic. The drug is still administered by a specialist. What changes is the sequence the plan wants to see and the documentation the clinic must submit to support that sequence.
The hidden variable: timing delays vs drug choice
The treatment decision is medical; the access decision can become logistical. And the logistical part has teeth: multiple calls, repeated faxes, “pending review,” and an appointment date that starts to slide.
- Drug choice is one decision.
- Time-to-injection is another decision—often made indirectly by paperwork speed.
- Site of care matters: clinic vs hospital outpatient can change billing and cost-sharing.
Open loop: Why two people on the “same plan” get totally different answers
It’s not your imagination. Two people can have the same insurance brand and still experience step therapy differently because: the plan’s utilization rules can vary by contract, the clinic’s billing pathways differ, and the prior authorization packet can be “complete” or “almost complete.” That last part—almost complete—causes the longest delays.
Money Block: Step-therapy eligibility checklist (yes/no)
- Is this a new start? Are you newly beginning a Part B-administered drug or restarting after a gap?
- Are you already stable? Are you actively receiving a specific drug on a regular schedule?
- Is the plan Medicare Advantage? (Step therapy rules typically live in plan documents, not in Original Medicare.)
- Where is the drug given? Retina clinic vs hospital outpatient can change billing and cost-sharing.
Neutral next step: Ask the clinic which rule is slowing you down: step therapy, prior auth, or site-of-care billing.
2) Avastin vs Eylea vs Vabysmo—how plans “think” about them
The cost ladder logic: why Avastin is often the first rung
Plans tend to see these medications through two lenses: clinical appropriateness and cost management. Avastin (bevacizumab) is widely used in retina practice and is often associated with lower acquisition cost compared to branded anti-VEGF drugs. That cost difference is a common reason it shows up as the “first step.”
The National Eye Institute explains that anti-VEGF injections are the most common treatment to slow vision loss from wet AMD. Your plan’s job, bluntly, is to pay the least it can while still meeting coverage rules. Your clinic’s job is to keep your care on time. You’re stuck in the middle unless you know what to ask—especially if this is your first anti-VEGF injection for wet AMD.
Not interchangeable in paperwork: brand names, billing codes, and documentation
Even when two drugs treat the same condition, they can be treated very differently by billing systems. Wet AMD injections are commonly billed under Medicare Part B pathways when administered in a clinic setting, and Medicare.gov notes that Part B may cover certain injectable treatments for AMD and that people often pay a share of the Medicare-approved amount (unless they have supplemental coverage).
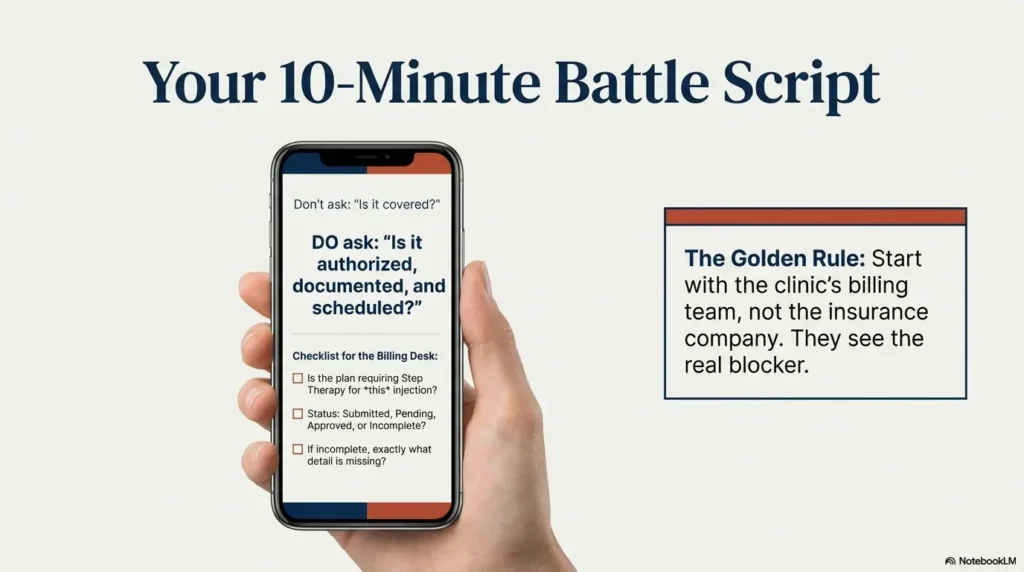
Translation: the “is it covered?” question is often less useful than: “Is it authorized, documented, and scheduled?”
If you’re trying to decode the paperwork side of branded drugs, it can help to read a plain-English explainer on Medicare coverage for Eylea injections so you know what questions to bring to the billing desk.
Show me the nerdy details
Step therapy and prior authorization often hinge on documentation terms: diagnosis detail, prior treatment history, imaging references (like OCT findings), and a stated rationale for medication choice. The plan isn’t reading your whole chart; they’re reading a distilled packet. Small missing details can trigger an “incomplete” loop.
Let’s be honest… your retina doctor isn’t picking based on coupons
If you’ve ever watched a retina clinic run on injection day, it looks like controlled chaos: technicians, imaging, consent, pharmacy workflows, and a schedule that can’t absorb repeated delays. Doctors are balancing disease activity, response, safety, and practical access. The insurance layer can force extra steps, but it doesn’t replace clinical judgment.
Another common scene: someone assumes “cheaper drug” means “worse drug” or “better drug” means “best for everyone.” The truth is calmer than that: different patients respond differently, and plans use broad rules that don’t always fit individual biology. (If you want that bigger picture in one place, start with how AMD injections work in real life.)
3) The clinic’s workflow that decides your real access
Buy-and-bill basics (why Part B-style drugs feel different than pharmacy meds)
Many wet AMD injections are handled as “clinic-administered” medications. That means your doctor’s office may obtain the drug and bill the plan after it’s administered. This feels different from picking up a prescription at a pharmacy because you’re paying for: the professional service, the drug itself, and sometimes a facility charge depending on the setting.
This is why a retina clinic’s billing/authorization team is often your best first call. They’re the ones who see exactly what the plan is asking for—and what’s missing.
Prior authorization & re-authorization cycles: where delays actually happen
Prior authorization isn’t a single gate; it can be a repeating cycle: approve, treat, re-approve, treat. The friction usually shows up in three places:
- First-time approval for a new drug or new patient.
- Switch approval when the clinic is changing drugs due to response or tolerance.
- Continuation approval where the plan asks for proof that ongoing treatment is still medically necessary.
Open loop: The one line in the chart note that can unlock coverage faster
Clinics vary, but one consistent “unlock” is a clear, plain statement that ties: diagnosis + current disease activity + rationale for the chosen medication + urgency of maintaining schedule. Not emotional urgency—clinical urgency.
If you want a practical way to help: ask the clinic whether the authorization packet includes a concise rationale and recent imaging summary. You’re not telling them how to practice; you’re helping them send the plan what it demands.
Money Block: Paperwork timeline estimator (no medical math—just calendar math)
Use this to estimate how authorization delays can push your schedule. It doesn’t predict outcomes. It just helps you decide when to escalate calls.
Neutral next step: If the delay pushes you past your cushion, ask the clinic whether an expedited request is appropriate.
4) Medicare Advantage vs Original Medicare + Medigap—what changes with Medigap
What Medigap can help with (cost-sharing) vs what it doesn’t (drug choice rules)
Medigap is supplemental insurance you can buy only if you have Original Medicare. Medicare.gov explains that Medigap generally helps pay your share of costs for services covered by Original Medicare (Part A and Part B), like copayments, coinsurance, and deductibles. That matters because wet AMD injections often run through Part B-style billing when administered in a clinic setting.
What Medigap typically doesn’t do: it doesn’t run a “preferred drug ladder” the way many Medicare Advantage plans can. Medigap isn’t a managed-care plan with prior authorization rules for most Part B services. But the doctor still has to document medical necessity, and the claim still has to be clean.
Why “no step therapy” doesn’t mean “no friction”
People sometimes switch expecting a magical world where every injection is instantly approved and scheduled. Reality is gentler and more boring: you can still see friction from billing issues, Medicare rules about what’s “reasonable and necessary,” and provider participation.
- Less plan friction often means fewer surprise hurdles.
- Not zero friction means you still need good clinic documentation and correct billing.
- Costs can become more predictable with the right Medigap plan.
The practical difference: fewer plan rules, but you still need clean billing + medical necessity
Here’s the most honest comparison: Medicare Advantage can add administrative steps like step therapy and prior authorization rules for Part B drugs. Original Medicare + Medigap can simplify the managed-care layer, but it doesn’t eliminate the need for proper documentation and consistent scheduling.
- Original Medicare is generally less “managed,” but still rule-bound.
- Medigap can reduce coinsurance shock for Part B-type services.
- The schedule is still king—keep injections from drifting.
Apply in 60 seconds: Ask the billing desk: “Will this be billed as Part B, and what will my share likely be with my coverage?”
5) Who this is for / not for
This is for you if…
- You’re on Medicare Advantage and you heard: step therapy, Avastin first, or prior authorization.
- You’re considering switching to Original Medicare + Medigap because of delays or out-of-pocket uncertainty.
- You’re a caregiver trying to keep injection visits from slipping.
This is not for you if…
- You only want drug efficacy comparisons (that belongs with your retina specialist).
- You’re in an employer retiree plan or Medicaid-only situation (rules can differ).
- You need immediate medical triage for new symptoms (call your clinic now).
A small empathy note: if you’re overwhelmed, you’re not failing. Insurance language is designed like a hedge maze. The goal is to find the one straight path through it: the clinic’s billing team + a simple script + a calendar you protect.
6) The “approval story” your plan expects to see
Medical necessity signals (what the plan wants documented)
Plans generally don’t want a novel. They want a tight story: diagnosis, evidence of disease activity, what’s been tried, response, and why the requested drug is appropriate now. Medicare.gov’s AMD coverage page notes that Part B may cover certain diagnostic tests and treatments, including certain injectable drugs, when medically appropriate. That “medically appropriate” part is where documentation lives.
- Diagnosis clarity: wet AMD (neovascular) vs other macular conditions.
- Current status: what the clinician sees now (not last year).
- Response history: improvement, stability, or non-response to previous therapy.
- Rationale: why this drug, why now, why staying on schedule matters.
“Fail first” without harm: how doctors frame step progression clinically
“Fail first” is a crude phrase, but the plan’s logic is often: start with the preferred option, then move up if needed. Clinicians can frame that progression in a medically responsible way: monitoring response, documenting disease activity, and changing therapy when there’s a justified reason.
Open loop: When an exception request is more realistic than “trying it anyway”
Sometimes you don’t have the luxury of “wait and see.” If a physician believes a particular drug is necessary due to prior response, clinical urgency, or a history that makes a step inappropriate, an exception process may be the cleaner path. The point is not to argue. The point is to submit the right rationale fast—before the calendar drifts.
Show me the nerdy details
Medicare Advantage step therapy for Part B drugs has guardrails in federal guidance and regulation, including protections intended to avoid disrupting ongoing therapy and rules about applying step therapy to new administrations. In practice, clinics still have to prove whether a patient is “new” to a drug and whether the requested therapy is a continuation or a new start.
Short Story: A caregiver keeps a sticky note on the fridge: “Right eye—every 6 weeks.” It started as a simple reminder. Then the clinic called: the plan needed prior authorization again. The caregiver assumed it was routine and waited for the clinic to “handle it.” Two weeks passed. Appointment moved. Then moved again.
When they finally asked the billing desk what was missing, it was one small thing: the plan wanted a specific phrase in the chart note tying the medication choice to current imaging. The clinic corrected it in a day. The authorization cleared. The next appointment still wasn’t perfect, but it stopped sliding. The caregiver didn’t become an insurance expert. They just learned the one lesson that matters: treat “pending” like a countdown, not a status.
7) Switching paths—when Medigap helps most (and when it won’t)
Scenario A: you’re stable on Eylea/Vabysmo and the plan wants Avastin
If you are stable on a specific therapy, the most important question is: does the plan consider this a “new administration” or a continuation? Federal guidance has emphasized that step therapy programs shouldn’t disrupt ongoing Part B drug therapy for beneficiaries already receiving an affected medication. The practical move: have the clinic clarify—on paper—that this is continuation and provide treatment history.
Switching to Original Medicare + Medigap can reduce the managed-care rule layer, but switching itself can create a short-term paperwork transition. If you’re considering it, plan the timing carefully with your clinic so you don’t create a gap.
Scenario B: you’re newly diagnosed and want the fewest delays
Newly diagnosed patients are the most exposed to step therapy rules because everything is “new.” If you’re time-poor (and who isn’t), the best focus is not “Which brand should I demand?” but: “How do I keep the first injection from being delayed?”
- Ask the clinic what the plan requires before the first injection day.
- Ask whether the plan’s rule is step therapy, prior auth, or both.
- Ask what documents you can sign or provide to speed release of records.
Scenario C: you’re traveling/snowbirding and need consistent scheduling
Wet AMD treatment is a schedule sport. If you travel, you need predictable billing pathways and a clinic that can coordinate. Medicare Advantage networks can complicate out-of-area care. Original Medicare often offers broader provider choice, but logistics still exist: transfer records, confirm participation, and ensure the new clinic can obtain and bill the drug.
Money Block: Decision card (access-first, not brand-first)
Choose Medicare Advantage when you value plan extras and your clinic confirms your plan’s injection workflow is smooth.
- Trade-off: more plan rules may mean more paperwork steps.
- Best for: stable routine, strong clinic admin support, clear authorizations.
Choose Original Medicare + Medigap when you want fewer managed-care hurdles and more predictable cost-sharing for Part B services.
- Trade-off: premiums and enrollment timing matter; availability varies by state.
- Best for: people burned by repeated delays or network constraints.
Neutral next step: Ask your clinic which option reduces “administrative touches” per injection visit.
8) Common mistakes that quietly cost vision (and time)
Mistake #1: Treating prior auth like “paperwork later” (timing is treatment)
Prior auth is not a background task. It’s a moving part that can change your appointment date. If you remember only one thing, make it this: “pending” is a countdown.
Mistake #2: Calling the insurer before the clinic’s billing team (wrong starting point)
Insurers often can’t see what’s missing in a packet the way the clinic can. The clinic knows whether the form is incomplete, whether a note needs a specific detail, or whether the request was submitted under the wrong pathway.
Mistake #3: Assuming “covered” means “available next week”
“Covered” is a benefits concept. “Scheduled” is a reality concept. Many people learn this the hard way: you can have coverage and still face delay if the request hasn’t been approved or the clinic can’t obtain the drug in time.
- Start with the clinic’s billing desk; they see the real blocker.
- Ask for the exact status: submitted, received, pending, approved, or incomplete.
- Get the next appointment date in writing (even if it’s “tentative”).
Apply in 60 seconds: Text yourself: “Drug + status + next date” after each phone call.
9) Don’t do this—two traps that trigger denials
Trap #1: Switching providers mid-authorization without transferring notes
Switching retina clinics can be necessary, but doing it mid-authorization can create an “information vacuum.” Plans don’t approve a vibe. They approve documentation. If records aren’t transferred quickly, the new clinic may have to restart the process.
A common scene: you book a new provider because you’re frustrated, but the old clinic’s notes don’t arrive for two weeks. Meanwhile, the plan says “no documentation,” and the calendar slips again.
Trap #2: Asking for a brand switch without a documented reason (plans key off the “why”)
“I prefer Vabysmo” is human. “Medical necessity for switching based on disease activity/response” is what plans can evaluate. If your doctor is switching you, ask what the clinical reason is—so the packet reflects it clearly.
Here’s what no one tells you… denials often come from missing details, not bad medicine
Denials can feel personal. They’re usually mechanical. Missing a diagnosis detail. Missing a date. Missing the explicit rationale tying the request to current disease activity. When you reframe denial as “incomplete,” you stop spiraling—and start fixing.
Show me the nerdy details
Medicare Advantage plans must publish coverage rules in plan documents (like Evidence of Coverage) and communicate changes through required notices. Many plans also have internal utilization management systems that flag missing elements and auto-generate “additional information requested” messages. When you ask the clinic for the exact missing element, you’re shortcutting that loop.
10) Your 10-minute call script (to reduce delays)
What to ask your retina clinic (billing/authorization checklist)
- “Is my plan requiring step therapy, prior authorization, or both for my injection?”
- “What drug name is on the request: Avastin, Eylea, or Vabysmo?”
- “What is the status: submitted, received, pending, approved, or incomplete?”
- “If incomplete, what exact detail is missing—and can it be corrected today?”
- “Do you recommend an expedited request given my schedule?”
What to ask your Medicare Advantage plan (step rules + exception pathway)
- “Is there step therapy for Part B drugs for wet AMD injections on my plan?”
- “Does step therapy apply only to new starts or also to continuation?”
- “What is the process for a step therapy exception, and what documentation is required?”
- “Is there an expedited review option if treatment is time-sensitive?”
What to ask if you’re considering Medigap (timing, provider acceptance, out-of-pocket structure)
- “If I move to Original Medicare, will my retina specialist accept it, and do they bill injections under Part B?”
- “Which Medigap plans help with Part B coinsurance for clinic-administered drugs?”
- “What is the earliest safe date to switch without interrupting scheduled injections?”
Money Block: Quote-prep list (what to gather before comparing)
- Your current plan name and plan type (HMO/PPO), plus the Evidence of Coverage.
- Drug name currently used (Avastin, Eylea, Vabysmo) and whether it’s continuation or a new start.
- Site of care (retina clinic vs hospital outpatient) and your usual injection frequency.
- Whether you travel and need out-of-area flexibility.
- Your comfort level with prior authorization cycles (high, medium, low).
Neutral next step: Bring this list to the clinic’s billing desk and ask what coverage setup causes the fewest delays.
12) Next step (one concrete action)
Call your retina clinic’s billing/authorization desk today and ask:
“Is my plan requiring step therapy or prior authorization for anti-VEGF injections, and what’s the fastest path for an exception if delaying treatment risks vision?”
Before you end the call, request three items:
- Exact drug name on the request.
- Authorization status (submitted/received/pending/approved/incomplete).
- Next appointment date (even if tentative).
If you’re time-poor, this is the highest-return call you can make. It compresses confusion into a simple status update.
FAQ
Does Medicare Advantage require step therapy for wet AMD injections?
Some Medicare Advantage plans can use step therapy for certain Part B-administered drugs, with rules and protections defined in federal guidance and regulation. The specifics vary by plan and whether your situation is considered a new start or continuation. The fastest way to know is to check your plan’s Evidence of Coverage and ask your clinic’s billing team what your plan is requiring right now.
Is Avastin covered for wet AMD under Medicare Advantage?
Coverage depends on the plan and how the drug is billed. In practice, many plans treat Avastin as a common first option in a step therapy pathway for wet AMD injections. Your clinic can confirm whether it’s the preferred first step for your specific plan contract.
Can a plan force me to switch from Eylea to Avastin?
Plans may try to apply step therapy rules to new administrations, but protections exist aimed at avoiding disruption of ongoing therapy. Whether a switch is demanded can hinge on whether the plan considers you “actively receiving” the drug. If you’re stable on a drug, ask the clinic to document continuation and request a clear exception pathway if needed.
Is Vabysmo covered under Medicare Part B or Part D?
Wet AMD injections administered in a clinic are commonly handled under Part B-type coverage pathways, but the exact billing route can depend on setting and plan design. Your retina clinic’s billing team can tell you how your injections are being billed and what that means for prior authorization or cost-sharing.
Does Medigap cover Eylea or Vabysmo costs?
Medigap generally helps pay your share of costs for services covered by Original Medicare (Part A and Part B), like coinsurance and deductibles. If your injection is covered by Original Medicare and billed through Part B, the right Medigap plan may reduce your out-of-pocket share. Medigap doesn’t usually impose step therapy rules the way a managed-care plan might, but your provider still must document medical necessity.
How long does prior authorization take for anti-VEGF injections?
Timelines vary widely by plan, clinic workflow, and whether the request is complete on the first submission. The most practical approach is to ask the clinic for the exact status and whether anything is missing, then request the next appointment date while the authorization is pending.
What is an exception request for step therapy and when is it approved?
An exception request asks the plan to cover a non-preferred drug without requiring the usual “first step,” based on medical necessity and documented rationale. Approval depends on the plan’s criteria and the clinical facts. If time is tight, ask the clinic whether an expedited review option is appropriate.
If my doctor says I need Eylea/Vabysmo, can the plan deny it anyway?
Plans can deny or delay requests that don’t meet their documentation or utilization criteria, even when a doctor recommends a medication. Many denials are effectively “incomplete packet” situations. Ask what exact element is missing and whether it can be corrected the same day.
Will switching from Medicare Advantage to Original Medicare stop step therapy?
Step therapy is generally a managed-care utilization tool. Original Medicare typically doesn’t operate with the same plan-level step therapy structure for Part B services. However, claims still need to meet coverage rules and be billed correctly. Also, switching coverage can create transition paperwork—plan the timing with your clinic to avoid a gap.
What documents does my retina clinic need to get injections approved?
Plans typically want a concise medical necessity story: diagnosis, evidence of disease activity, treatment history, response, and rationale for the requested drug. Your clinic’s billing/authorization team knows the plan’s specific requirements and can tell you what’s missing if the request is delayed.
Wrap-up: keep the shot on schedule
Let’s close the loop from the beginning: why do two people on the “same plan” get different answers? Because the real system isn’t just the plan. It’s the plan plus the clinic’s authorization workflow plus whether the documentation packet is complete on the first try. That’s why one person glides through and another gets stuck in “pending.”
Infographic: The 5-step access pathway (and where delays hide)
Symptoms + imaging → treatment plan
🟢 Usually fast
Avastin / Eylea / Vabysmo chosen clinically
🟡 Plan may prefer one
Diagnosis + rationale + history
🔴 Delay hotspot
Approved / incomplete / denied
🔴 Delay hotspot
Drug obtained → injection date locked
🟡 Capacity matters
Use it: When you’re stuck, ask which step you’re in. Then ask what specific detail moves you to the next step.
If you want the simplest, fiercest practical advice: make the calendar visible. Put the next injection date somewhere you’ll see it. Treat “pending authorization” like a countdown. And when you call, don’t ask, “Is it covered?” Ask: “Is it approved and scheduled?”
If you’re supporting someone who’s older, anxious, or exhausted by appointments, it’s normal for the “needle fear” to become part of the logistics. In that case, it can help to skim practical coping tools for wet AMD injection anxiety in your 70s—not as therapy, but as a way to keep fear from turning into missed visits.
And if the day-to-day life side is getting harder (reading labels, organizing drops, keeping a safer home path at night), don’t wait until you’re “bad enough.” Consider a low vision specialist for macular degeneration, use a simple low-vision medication management workflow, and keep a practical wet AMD home safety checklist nearby so “small hazards” don’t become big problems.
Last reviewed: 2026-01.