


The Safe 10-Minute Post-Meal Walk
Ten minutes after dinner is where a lot of “healthy intentions” quietly fail—because the walk turns into a power walk, the curb feels higher than it used to, and someone ends up dizzy on a bench pretending it’s fine.
If you’re trying to use 10-minute post-meal walks for diabetic retinopathy, the goal isn’t fitness drama. It’s a gentle, repeatable habit that supports postprandial glucose control without provoking blood-pressure spikes, strain, or fall risk—especially when vision and balance are part of the equation.
Keep guessing, and the cost is sneaky: missed consistency, unnecessary scares, and the kind of “one bad walk” that makes people stop moving altogether.
This routine gives you a safe weekly template, easy intensity cues (talk test, nasal breathing), and clear stop rules for red-flag symptoms—plus a simple script for your next ophthalmology/diabetes visit (including proliferative retinopathy treatment conversations (PRP vs anti-VEGF)).
It’s built for real life: predictable meal anchors, flat-route logic, and caregiver-friendly simplicity.
A 10-minute easy walk starting about 10–15 minutes after meals can help soften post-meal glucose spikes and is often easier to maintain than longer workouts. If you have diabetic retinopathy, keep intensity gentle, avoid straining or “burst” efforts that can spike blood pressure, and pause exercise if you notice new eye symptoms (sudden floaters, flashes, curtain-like shadow, or abrupt blur). When in doubt—especially with proliferative/unstable retinopathy—get individualized clearance from your eye clinician and diabetes care team.
Safety / Disclaimer (read first)
This is general education—not medical advice. Diabetic retinopathy can make certain activities riskier, especially when intensity or breath-holding triggers sharp blood-pressure swings. And because vision changes can affect balance, safety here isn’t “extra.” It’s the point.
- Get personalized clearance if you have proliferative or unstable retinopathy, recent eye procedures (laser/injection/surgery), a recent bleed, or new/worsening vision symptoms.
- Stop the walk and seek care if you get sudden floaters, flashes, a curtain/shadow over vision, sudden blur, severe eye pain, chest pain, fainting, or repeated near-falls.
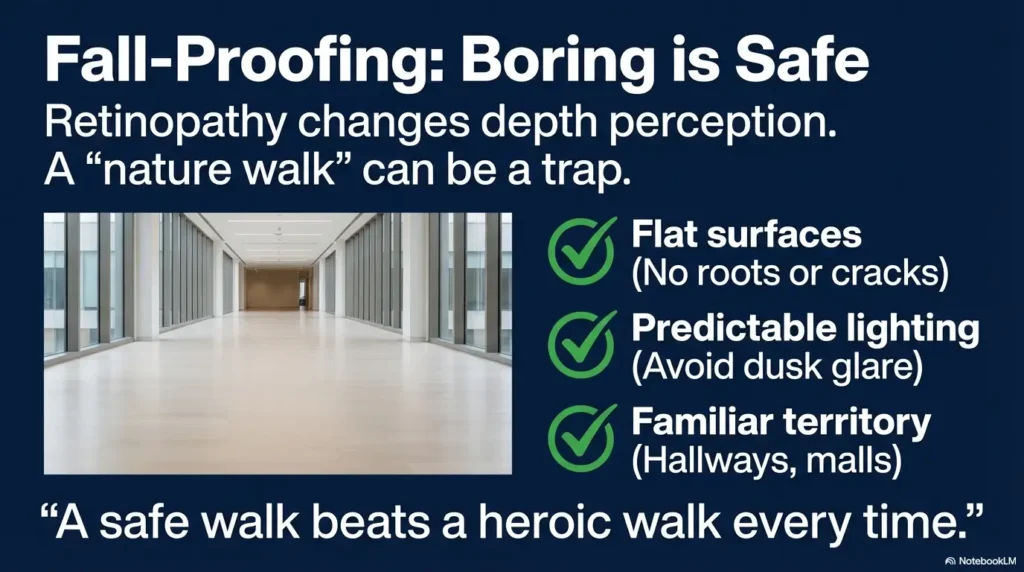
- Prioritize fall prevention over “fitness goals.” A safe walk beats a heroic walk every time.
I’ll be honest: I’ve watched a loved one “power through” a walk because it sounded virtuous—only to end up dizzy and shaken, sitting on a curb with that stubborn look that says, “I’m fine,” while their hands say otherwise. We’re not doing that. We’re doing sustainable.
- Keep intensity easy (talk test, nasal breathing).
- Avoid strain, breath-holding, and jarring bursts.
- Use symptom-based stop rules—no heroics.
Apply in 60 seconds: Put a note on your phone: “Easy pace only. Stop for new floaters/flashes.”
Table of Contents

1) The “10 minutes” question: why this tiny habit can matter (and when it won’t)
1.1 The glucose-spike window most routines ignore
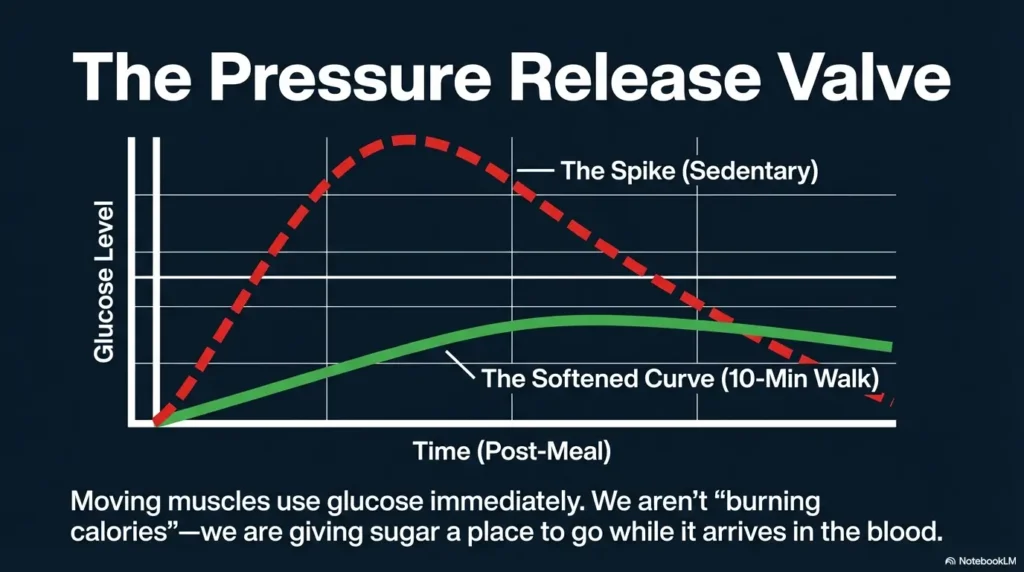
Most people picture exercise as a big, sweaty “session.” But post-meal walking works because it shows up during a very specific moment: when glucose is trying to climb. A gentle walk can act like a small “pressure release valve” for that climb—without demanding a gym membership, a special outfit, or the kind of motivation that mysteriously disappears after lunch.
I once tried to convince an older relative to do a “proper workout.” They nodded politely… and never did it. When we switched to “just 10 minutes after dinner,” it finally fit real life. Not inspiring. Just doable. And in health behavior, doable is often the secret engine behind results.
1.2 Retinopathy reality check: what walking can’t “fix”
Let’s keep this honest: walking after meals is not a treatment for diabetic retinopathy. Retinopathy is an eye disease linked to long-term blood sugar control, blood pressure, and other factors. The core care lives with your eye clinician (often an ophthalmologist/retina specialist) and your diabetes team. What post-meal walking can do is support better glucose patterns over time—one of the pieces that generally helps the bigger picture.
If you’ve ever felt that pang of disappointment—“So it won’t fix my eyes?”—I get it. But supporting glucose control is still meaningful. It’s not magic. It’s maintenance. And maintenance is how many people keep their future from shrinking.
1.3 Curiosity gap: Why do some people feel worse after “healthy” walks?
Because “healthy” is not one-size-fits-all. Some people feel worse because they accidentally:
- Walk too fast (turning “easy” into “effort”).
- Walk in heat or hills (blood pressure + dehydration + dizziness).
- Walk with low blood sugar symptoms (especially with insulin or certain meds).
- Choose uneven routes (trip hazards become bigger when vision is compromised).
In other words: it’s not walking that’s the problem. It’s the unseen intensity and hidden hazards. We’ll remove both.
- Walking supports glucose patterns, not instant eye repair.
- Feeling worse usually means intensity or safety drifted.
- “Easy and consistent” beats “hard and occasional.”
Apply in 60 seconds: Decide your “easy cue” (nasal breathing or full-sentence talking) and stick to it.
2) Who this is for / not for
2.1 Good fit: stable walkers who want a low-friction routine
This plan fits if you (or your parent) can walk comfortably for 5–10 minutes on a flat surface, and you want a routine that doesn’t require willpower Olympics. You’re aiming for gentle glucose support and a habit that doesn’t argue with aging joints, vision changes, or energy fluctuations.
2.2 Good fit: caregivers building consistency for a parent
If you’re the caregiver, you’re not looking for a perfect plan—you’re looking for a plan that survives Tuesday. This approach is caregiver-friendly because it uses anchors (meals), small time commitments, and clear stop rules that reduce anxiety.
I’ve seen caregivers burn out trying to “motivate” exercise. The win often comes from removing negotiation: “After dinner, we do one loop. Then we’re done.” Simple. Predictable. Less emotional friction.
2.3 Not for (until cleared): recent bleed, rapidly changing vision, severe dizziness/falls history
Pause and get clinical guidance first if there’s a recent vitreous hemorrhage concern, sudden changes in vision, recent eye procedures, or a strong fall history. Also, if dizziness is frequent, you may need medical evaluation and route/assistive adjustments before this becomes safe.
2.4 “If you’re unsure”: the 30-second screening questions to ask your clinician
Bring these to your next visit (eye clinician and/or diabetes team). They’re quick, specific, and they show you’re being careful:
- “Given my retinopathy status, is gentle walking after meals okay? Any limits on pace, hills, or stairs?”
- “Are there any signs (floaters/flashes/blur) that mean I should stop activity immediately?”
- “If I use insulin or glucose-lowering meds, what’s the best way to reduce hypoglycemia risk with short walks?”
- Yes — I can walk 5–10 minutes on a flat surface without severe pain.
- Yes — I can speak in full sentences while walking slowly.
- Yes — I have a safe, well-lit route (or an indoor alternative).
- No / Not sure — I have new floaters/flashes, sudden blur, or a recent eye bleed.
- No / Not sure — I’ve had repeated falls or frequent dizziness.
Next step: If you answered “No / Not sure” to the last two, get clearance and route modifications before starting.
Neutral action: Put these questions in your phone notes for your next appointment.
3) Don’t do this: the BP-spike moves that can stress vulnerable eyes
3.1 The “pressure spike” list: straining, breath-holding, heavy resistance, all-out bursts
If you have diabetic retinopathy—especially proliferative or unstable forms—activities that sharply increase blood pressure are often the ones clinicians flag. The usual suspects:
- Straining (especially with breath-holding).
- Heavy lifting or high-load resistance work without careful technique.
- All-out bursts (sprints, “see how fast I can go” moments).
- Valsalva-style breath holding (that “brace and push” habit).
One of the sneakiest “BP spikes” in daily life? Carrying heavy grocery bags up stairs while holding your breath because you want to do it in one trip. It feels efficient. Your body reads it as a pressure event.
3.2 The “jarring” list: jumping, sprint intervals, steep downhill pounding (why it’s different)
Jarring movement isn’t just about joints. For some people, the combination of impact, strain, and sudden intensity shifts is exactly what you want to avoid when eye fragility is a concern. Skip:
- Jumping and plyometrics.
- Sprint intervals.
- Steep downhill “pounding” (it often increases impact and speed without you noticing).
3.3 What “safe intensity” feels like (talk test + nasal breathing cues)
Here’s the simplest intensity filter that doesn’t require gadgets:
- Talk test: You can speak a full sentence without gasping.
- Nasal breathing: You can breathe mostly through your nose.
- Quiet steps: Your footsteps sound soft, not stompy.
If you feel that “competitive itch” to speed up, you’re human. I’ve done it too—turning a calm walk into a personal audition for the Olympics. The trick is to remember: the goal is glucose support, not conquest.
3.4 If you do strength work: safer modifications to discuss (lighter loads, no Valsalva)
Strength training can be valuable for older adults—but with retinopathy, it’s worth discussing modifications with your clinician and possibly a physical therapist:
- Lower loads, higher control.
- No breath-holding; exhale on effort.
- Avoid maximal lifts and “grinding reps.”
- Choose stable positions (seated or supported when needed).
Think of strength work like seasoning: helpful in the right dose, unpleasant when dumped in.
4) Start-time strategy: why “10–15 minutes after eating” is the sweet spot
4.1 Here’s what no one tells you… “after meals” has a timer
“After meals” sounds vague until you live it. If you wait too long, you miss part of the post-meal glucose rise. If you start immediately, some people feel uncomfortable (especially after a larger meal). For many, a gentle start about 10–15 minutes after eating is a practical compromise: enough time to settle, soon enough to matter.
I like to call it the “dishwasher window.” When the plates are rinsed (or at least stacked with good intentions), it’s go time.
4.2 What the evidence suggests about early post-meal movement
Research on postprandial (post-meal) activity has repeatedly pointed to a simple mechanism: moving muscles use glucose. You’re not trying to “burn off” the meal like punishment. You’re simply giving your body a gentle place to put glucose while it’s arriving.
Show me the nerdy details
Post-meal glucose control is influenced by meal composition, medication timing, and how quickly glucose enters circulation. Light activity tends to increase glucose uptake in working muscle and can reduce the size of the post-meal rise. The goal here is not peak fitness; it’s nudging the curve gently and consistently.
4.3 If you can’t walk then: the backup windows that still help
Real life has meetings, weather, fatigue, and the occasional “I sat down and my body staged a coup.” If 10–15 minutes doesn’t happen, try:
- 20–30 minutes after the meal (still useful for many people).
- A 5-minute “micro-walk” now, and another 5 minutes later.
- Indoor loops (hallway, porch, mall) when outdoors is unsafe.
4.4 How to pair with meds/insulin timing (discussion prompts, not directives)
If you use insulin or glucose-lowering medications, short walks after meals can sometimes increase the risk of going low—depending on dosing, timing, and the meal. Don’t guess alone. Use prompts like:
- “Should I adjust timing or carry fast carbs for a 10-minute post-meal walk?”
- “Are there patterns in my CGM or fingersticks after dinner walks?”
- “What should my low-sugar plan be during walks?”
Consider this your permission slip to be boringly prepared. (If you’re on GLP-1 meds like semaglutide, it’s also worth scanning your own risk context—see Ozempic and diabetic retinopathy timing questions and sudden vision-loss red flags in older adults on semaglutide—then bring your specifics to your clinician.)
Input 1: Time you finish eating (e.g., 6:30 PM)
Input 2: Your “start delay” (10–15 minutes)
Input 3: Walk duration (10 minutes)
Output: Your walk window is 6:40–6:55 PM (start) and you’re done by 6:50–7:05 PM.
Neutral action: Set one repeating phone timer labeled “Easy 10-minute walk.”
5) The safe weekly routine: a 7-day template older adults actually follow
5.1 Your baseline week (Days 1–7): 10 minutes after 1 meal/day
Start with one meal per day. Pick the meal that’s most predictable—often dinner. Your only job is to show up for 10 minutes at an easy pace. That’s it. No upgrades. No “since I’m already out…” detours.
- Days 1–7: 10 minutes after your chosen meal, 10–15 minutes after eating.
- Pace: full-sentence talking pace; mostly nasal breathing.
- Route: flat, familiar, well-lit, low-clutter.
I’ve watched people fail not because they couldn’t walk—but because they tried to start as a new person. Start as yourself. The version of you who sometimes forgets, sometimes has low energy, and still deserves a plan that works.
5.2 Week 2: add a second meal (the “two anchors” method)
Once one walk feels normal-ish, add a second “anchor meal.” Many people choose breakfast + dinner or lunch + dinner depending on schedule and safety.
- Week 2: 10 minutes after two meals on most days.
- Still easy pace. If you’re tempted to speed up, shorten the route instead.
5.3 Week 3: build to all 3 meals—without intensity creep
If energy and safety allow, gradually add the third meal walk. The main risk here is “intensity creep”—that subtle slide from gentle to brisk because you’re feeling proud. Pride is lovely. It just shouldn’t run your blood pressure.
Show me the nerdy details
Short post-meal bouts can sometimes produce stronger postprandial glucose effects than a single longer session because they repeatedly target the glucose rise after eating. Consistency matters more than speed. For retinopathy safety, stable intensity is the priority.
5.4 Optional: “micro loops” indoors (hallway laps, mall walks, porch circuits)
Indoor loops aren’t “less real.” They’re often safer: better lighting, flatter surfaces, fewer surprises. A mall walk can be the most underappreciated health hack in America—quietly climate-controlled and full of benches.
5.5 If fatigue hits: deload week rules (keep the habit, shorten time)
When fatigue shows up (and it will), don’t quit. Deload.
- Drop to 5 minutes after one meal.
- Keep the routine cue (timer + shoes).
- Return to 10 minutes when energy stabilizes.
- Choose three 10s if your goal is post-meal glucose support and habit consistency.
- Choose one 30 if scheduling one block is easier and you can keep intensity gentle throughout.
- Choose “two 10s” if fatigue, vision, or weather makes three unrealistic.
Neutral action: Pick the option you can repeat for 14 days without “pushing.”
6) Vision-first fall-proofing: make walking safer when sight is compromised
6.1 Route design: flat, familiar, well-lit, low-clutter surfaces
Retinopathy can reduce contrast sensitivity and make uneven surfaces feel like booby traps. Your route is a medical decision, not a scenery decision. Prioritize:
- Flat sidewalks or indoor corridors.
- Predictable lighting (avoid dusk glare if it’s tricky; if glare is a recurring enemy, consider a few glare-control lighting fixes at home too).
- Minimal trip hazards (roots, cracked pavement, loose gravel).
I used to romanticize “nature walks.” Then I watched someone step on a hidden pinecone and wobble like a cartoon. Now I’m a proud fan of boring routes. Boring routes keep you walking.
6.2 Gear that quietly prevents accidents (shoes, cane/trek pole, ID, glucose tabs)
- Stable shoes with good grip (no slick soles).
- Assistive support if balance is uncertain (cane, walking stick, or trekking pole used correctly).
- ID + phone on your body (not in a bag you might set down).
- Fast carbs if hypoglycemia is a possibility (glucose tabs are tidy and predictable).
If nighttime trips are part of the fall-risk story, build a safety runway at home too—especially with vision changes. A simple low-vision nighttime bathroom safety checklist can prevent the kind of “tiny slip” that turns into weeks of fear.
6.3 Let’s be honest… your eyes get tired before your legs
Visual fatigue is real. Some older adults feel mentally exhausted from scanning the ground, not physically tired from walking. If that’s you, shorten the route and improve the surface rather than forcing distance. “Easy” includes your eyes.
6.4 Walking with a buddy: the caregiver pacing script (no nagging, just cues)
If you’re walking with a parent, try cueing safety instead of speed:
- “Let’s keep it easy—I want you comfortable.”
- “Eyes first. We’re watching for cracks and curbs.”
- “If anything feels off—dizzy, shaky, weird vision—we stop. No debate.”
A caregiver’s calm tone is a safety tool. It lowers stress, and stress can raise blood pressure. Yes, your vibe matters.
7) Common mistakes (the “I was trying to be healthy” traps)
7.1 Mistake: turning a gentle walk into a “power walk” sprint
This is the most common failure mode: you start gently, then the brain whispers, “We should make it count.” Suddenly you’re speed-walking past a neighbor like you’re late for a flight. For retinopathy safety, resist the urge to “upgrade” intensity. If you want to progress, add consistency first (more days), not speed.
7.2 Mistake: hills + heat + dehydration = dizziness + falls risk
Heat and hills can spike effort quickly. Dehydration can worsen dizziness, especially in older adults. The fix isn’t toughness—it’s planning:
- Choose flat routes.
- Walk indoors when it’s hot or icy.
- Bring water if needed, and keep walks short.
7.3 Mistake: breath-holding on stairs or while carrying groceries
Breath-holding is sneaky. It shows up on stairs, when carrying bags, or when “bracing” the core. If you do stairs, do them gently, hold the rail, and breathe out on effort. Better yet, keep the post-meal walk flat and save stairs for when you’re not rushed.
7.4 Mistake: walking with low blood sugar symptoms (what to do instead)
If you feel shaky, sweaty, confused, unusually irritable, or weak—treat it as a possible low. The correct move is not “walk it off.” Stop, check if you can, and follow your clinician’s guidance for lows. Keep fast carbs on you if lows are plausible.
7.5 Mistake: ignoring new floaters/flashes because “it’ll pass”
New floaters, flashes, sudden blur, or a curtain/shadow are not “wait and see” moments—especially with retinopathy. These symptoms can signal urgent eye issues. The safe rule: stop activity and contact your eye care team or seek urgent evaluation. (If you’re unsure what “blurry” is telling you, it may help to compare patterns like waking up with blurry vision or medication-related causes such as Topamax and sudden blurry vision—then treat new retinopathy-type warning signs as urgent, not educational.)
7.6 Mistake: skipping foot checks (blisters become the silent stopper)
Foot discomfort is one of the fastest ways older adults quietly abandon walking. Quick check after walks:
- Red spots, blisters, rubbing areas.
- Socks that slide or bunch.
- Shoes that feel “fine” for 3 minutes and terrible at minute 9.
My own wake-up call was a blister that seemed small until it became the reason I avoided movement for a week. Feet are the gatekeepers. Treat them like VIPs.
- Keep walks flat, cool, and easy.
- Never walk through low-sugar symptoms.
- New eye symptoms mean stop and seek help.
Apply in 60 seconds: Put glucose tabs and an ID card in the same pocket every walk.
8) When to seek help (and pause the routine)
8.1 Eye red flags: sudden floaters, flashes, curtain/shadow, sudden blur
If any of these show up, stop walking and seek urgent eye guidance:
- Sudden shower of floaters.
- Flashes of light.
- A curtain or shadow in your vision.
- Sudden new blur or distortion.
8.2 Body red flags: chest pain, fainting, severe shortness of breath, repeated falls
These are medical red flags in any context. Don’t “push through.” Stop and seek urgent care or emergency services as appropriate.
8.3 Diabetes red flags: recurrent lows, confusion, “can’t recover” fatigue
If short walks repeatedly trigger lows—or you feel confused, unusually fatigued, or unable to recover—pause the routine and talk with your diabetes team. The plan may need medication timing or snack adjustments.
8.4 Post-eye treatment rules: what to ask after injections/laser/surgery (checklist)
After an eye injection, laser treatment, or surgery, activity limits can vary. Ask your eye clinician:
- “When can I resume gentle walking?”
- “Are there restrictions on bending, lifting, or straining?”
- “What symptoms mean urgent evaluation?”
Show me the nerdy details
Retinopathy risk discussions often focus on avoiding sudden spikes in blood pressure and minimizing activities that combine strain + impact. Post-procedure guidance can vary because healing, bleeding risk, and eye pressure considerations differ by individual situation and procedure type.
- Your retinopathy status (nonproliferative vs proliferative, stable vs changing—ask if you’re unsure).
- Recent eye treatments (laser/injection/surgery) and dates.
- Your fall history (any falls in the last 6–12 months?).
- Medication list (especially insulin and glucose-lowering meds).
- Typical post-meal glucose pattern (CGM trend or a few fingerstick notes).
Neutral action: Bring this list to your next appointment so advice can be specific.
FAQ
1) Is it safe to walk after meals if I have proliferative diabetic retinopathy?
Often, gentle walking can be acceptable, but proliferative or unstable retinopathy is exactly where individualized clearance matters most. Ask your ophthalmologist/retina specialist about limits on pace, hills, stairs, and any restrictions related to recent bleeding or procedures. Use strict stop rules for new floaters, flashes, curtain/shadow, or sudden blur. If you’re trying to understand what “proliferative” means in real-life treatment terms, you may want a quick refresher on PRP vs anti-VEGF for PDR before your visit.
2) How soon after eating should I start the 10-minute walk—immediately or after 15 minutes?
For many older adults, starting around 10–15 minutes after finishing the meal is a practical sweet spot: soon enough to matter, late enough to feel comfortable. If you get reflux or stomach discomfort, shift slightly later. If you can’t walk then, use a backup window (20–30 minutes) or split into two 5-minute walks.
3) What pace is “safe” if my eye doctor warned me about pressure spikes?
Aim for “easy”: you can speak full sentences, breathe mostly through your nose, and keep your steps quiet. Avoid breath-holding, hills, and any urge to “burst” faster. If you feel strain in your face/neck, you’re likely pushing too hard—slow down immediately. (If your doctor is also tracking blood pressure effects on the retina, it can help to understand adjacent conditions like hypertensive retinopathy so the “why” behind the caution feels less mysterious.)
4) Will post-meal walking improve diabetic retinopathy, or just blood sugar control?
Post-meal walking is best viewed as a glucose-support habit, not a direct treatment for retinopathy. Retinopathy care is managed with eye clinicians and depends on disease status, blood sugar patterns over time, blood pressure, and other medical factors. The walk is a practical way to support one piece of the broader picture. If you also have swelling-related symptoms, it’s worth knowing the basics of diabetic macular edema symptoms so you can describe changes clearly.
5) What if I use insulin—can walking after meals cause low blood sugar?
Yes, it can for some people, depending on dosing, timing, and meal size. Talk to your diabetes care team about post-meal movement and hypoglycemia prevention. Carry fast carbs, know your low-sugar symptoms, and don’t treat a walk like a test of toughness.
6) Is indoor walking (mall/hallway) as effective as outdoor walking?
For post-meal glucose support, indoor walking can work just fine—and it’s often safer due to flat surfaces and steady lighting. Choose the option you can repeat consistently without fall risk or weather stress. If screens and indoor lighting leave eyes feeling “fried,” you may also want a quick read on digital eye strain in seniors so you can tweak the environment, not just the walk.
7) How many days per week do I need to walk to see a benefit?
Consistency matters more than perfection. Many people start noticing better post-meal patterns with most days of the week, but the safest path is progressive: one meal per day for a week, then add anchors if tolerated. If you can only do 4–5 days, that’s still a meaningful habit—especially if it’s stable and safe.
10) Next step: one concrete action (do this today)
10.1 Set a repeating timer: “Walk 10 minutes” for your largest meal
Pick the meal that tends to create the biggest post-meal rise (often dinner). Set one repeating timer for 10–15 minutes after that meal. The timer is your “starter pistol.” No decision-making required.
10.2 Print a one-page “retinopathy-safe walking rules” card for your wallet
- Easy pace only: full sentences, mostly nasal breathing.
- No strain: no breath-holding, no heavy carrying, no bursts.
- Flat route: stable surface, good lighting.
- Stop for eye symptoms: new floaters, flashes, curtain/shadow, sudden blur.
- Stop for body symptoms: chest pain, fainting, severe shortness of breath, repeated near-falls.
10.3 Bring 3 questions to your next eye/diabetes visit (ready-to-read script)
Read these directly from your phone if you need to (I’ve done the same when nerves steal my words):
- “Is gentle post-meal walking safe for my current retinopathy status?”
- “What symptoms mean I should stop activity and seek urgent eye care?”
- “Given my meds/insulin, what’s my safest plan to prevent lows during short walks?”
💡 Read the official diabetic retinopathy warning-sign guidance
Conclusion
Remember the quiet worry from the beginning—the fear that exercise advice might accidentally make things worse? Here’s the closure: the safest routine isn’t the one that demands more effort. It’s the one that keeps intensity gentle, removes fall hazards, and respects retinopathy-specific red flags.
If you do nothing else, do this: pick one meal, set a timer for 10–15 minutes after, and take a 10-minute easy walk on a flat, familiar route. Let it be small. Let it be boring. Let it be yours. In 15 minutes, you can complete your first “baseline walk” and prove to your nervous system that health doesn’t have to feel like a gamble.
Start 10–15 minutes after eating (use a timer). If needed: 20–30 minutes, or split into two 5s.
Easy pace: full-sentence talk test, mostly nasal breathing, quiet steps. No “burst” moments.
Stop for new floaters/flashes, curtain/shadow, sudden blur, chest pain, fainting, severe shortness of breath, repeated near-falls.
Flat, familiar, well-lit route. Indoors is great. Boring is safe. Safe is consistent.
Last reviewed: 2026-01.