

Beyond Guesswork: Navigating Medication with Confidence
The bottle is right there, but the label has turned into gray weather and your hand has started its own tiny orchestra.
Low vision with essential tremor can make medication routines feel unfairly complicated: not because you are careless, but because the task demands clear reading, steady handling, accurate timing, and calm confidence all at once. A refill looks different, a cap refuses to open, a pill rolls across the tray, and suddenly “just take your medicine” becomes a small daily negotiation.
The real risk is not inconvenience. It is guessing.
And guessing can lead to missed doses, double doses, wrong bottles, unsafe pill splitting, or delayed calls to the pharmacist.
This guide helps you build a safer medication routine using large-print labels, talking prescription tools, tactile markers, stable dosing surfaces, and a simple no-guessing rule. The goal is not a perfect system. The goal is a routine that still works on tired mornings, shaky evenings, and low-light days.
The Safety Protocol:
- Confirm first, handle second.
- Record clearly.
- Call a human when the system stops protecting you.
Start with one bottle. Make one cue clearer. Let safety become ordinary.
Table of Contents
Fast Answer
Low vision with essential tremor makes medication safety harder because the same task often requires clear seeing, steady hands, memory, and timing. Safer routines usually combine large-print or talking labels, tactile organization, stable surfaces, pharmacy support, caregiver checks, and a “no guessing” rule. Never change doses, split pills, or combine medicines without a clinician or pharmacist’s guidance.
- Make labels easier to confirm.
- Give every bottle a consistent place.
- Pause when vision, tremor, or confidence drops.
Apply in 60 seconds: Pick one medication bottle and decide how you will confirm it without guessing.
Safety / Disclaimer: This Is a Medication-Safety Guide, Not Medical Advice
This guide is about safer daily routines. It is not a diagnosis, prescription plan, or replacement for instructions from your doctor, pharmacist, nurse, eye specialist, neurologist, or occupational therapist.
The U.S. Food and Drug Administration advises people to take medicines as prescribed and to talk with a health care professional before making changes. That sounds simple until a refill looks different, a label is unreadable, or a tremor turns the cap into a tiny locked vault.
Use This Alongside Your Doctor’s and Pharmacist’s Instructions
Medication safety begins with the official instructions, not with the kitchen counter improvisation committee. If your bottle says one thing, your discharge paperwork says another, and your memory says a third thing, that is not a personality test. It is a call-the-pharmacist moment.
I once watched someone spend 8 minutes trying to decide whether a pale tablet was the “morning one” or the “new one.” The problem was not intelligence. The problem was a system that asked a tired person to identify medicine by vibes and beige.
Do Not Guess When Vision, Tremor, or Fatigue Changes the Task
Low vision and essential tremor can both fluctuate. Lighting changes. Fatigue rises. Stress tightens the hand. A task that was easy at 10 a.m. may be risky at 9 p.m.
Medication safety has to respect bad days. A good system should not depend on perfect eyesight, perfect steadiness, perfect memory, or saint-level patience.
Keep Emergency Instructions Visible, Audible, and Shareable
Keep a current medication list where another person can find it quickly. Include prescription medicines, over-the-counter products, vitamins, supplements, allergies, pharmacy phone number, prescriber names, and emergency contacts.
For low vision, that list may need to exist in 2 formats: a large-print paper version and an audio or phone-accessible version. If a caregiver visits only once a week, the list should not live in a mystery drawer guarded by old batteries and takeout menus. A one-page medication list template can make that information easier to update, share, and find when the room suddenly feels too busy.
Start Here: The Real Problem Is Not “Small Print”
Small print matters. Of course it does. Prescription labels can look like legal contracts written for ants. But low vision with essential tremor is bigger than font size.
The real challenge is that medication tasks are stacked tasks. You may need to read, remember, open, pour, count, separate, swallow, record, and repeat at the right time. When one part fails, the whole routine wobbles.
Low Vision Changes the Reading Task
The National Eye Institute explains that low vision can make everyday activities difficult, including reading, even when regular glasses, contact lenses, medicine, or surgery do not fully correct the problem.
That means the issue is not laziness or carelessness. It is visual access. A label that looks “clear enough” to someone else may be slow, blurred, low-contrast, glare-heavy, or exhausting to read.
Essential Tremor Changes the Handling Task
MedlinePlus describes essential tremor as involuntary shaking that often appears during action, such as reaching, writing, eating, or holding objects. That matters because medication routines are full of small action tasks.
Opening a cap, aiming an eye drop, pouring liquid to a line, or holding a tiny pill between thumb and finger can become a circus act performed over tile flooring. Nobody needs that kind of matinee.
The Risky Overlap: When Reading and Handling Fail Together
Low vision asks, “Can you identify this?” Tremor asks, “Can you handle this?” Medication timing asks, “Can you do both at the right moment?” That overlap is where errors breed.
Here is the quiet danger: people often compensate for one limitation by leaning harder on another ability. If sight is poor, they rely on bottle shape. If the hand is shaky, they rush before the tremor worsens. If memory is tired, they trust routine. Each shortcut can work once. Then one refill, one new bottle, one bad morning, and the shortcut becomes a trap.
Medication Safety Overlap Map
👁️
Low vision
Label reading, contrast, glare, pill appearance, refill changes.
✋
Essential tremor
Caps, pouring, counting, eye drops, tiny pills, spilled doses.
⏱️
Timing
Morning, noon, evening, bedtime, missed doses, double-dose risk.
Safer design goal: make the right medicine easier to confirm before the hand has to do anything delicate.
Who This Is For / Not For: Make the Reader Feel Seen Early
This guide is for adults who are still trying to manage daily routines with dignity. It is also for caregivers who want to help without turning the medicine shelf into a control tower.
There is a particular exhaustion that comes from needing help with a task you used to do automatically. The bottle did not become emotionally complicated overnight, yet here we are, negotiating with plastic at breakfast.
For Adults Managing Pills, Drops, Liquids, or Inhalers With Low Vision and Tremor
This article may help if you use tablets, capsules, eye drops, liquid medicine, inhalers, patches, injections prepared by a clinician, or over-the-counter medicines that must be taken on a schedule.
It may also help if you have ever said one of these sentences:
- “I know what this is, but I want to be sure.”
- “The pill changed color after the refill.”
- “My hand shakes more when I’m rushed.”
- “I can read it under bright light, but not at night.”
- “I hate asking someone to check this every time.”
For Family Caregivers Who Help Without Taking Over
A caregiver’s job is not to become the medication monarch. The better goal is to reduce risk while preserving as much independence as possible.
That may mean setting up large labels, arranging bottles in reliable zones, checking refills, or watching the routine once to identify where the task breaks down. It does not mean swooping in like a caffeinated raccoon and reorganizing everything without explanation.
Not For Emergencies, New Neurological Symptoms, or Unexplained Dosing Changes
This guide is not for sudden confusion, new severe weakness, chest pain, fainting, suspected overdose, allergic reaction, or sudden neurological changes. Those situations need urgent medical help.
It is also not a guide to changing medication dose, timing, pill splitting, or stopping treatment. Those decisions belong with a clinician or pharmacist who can review the actual medication and health context.
Eligibility Checklist: Is This Routine Ready for a Safety Upgrade?
| Question | Yes / No | Next step |
|---|---|---|
| Can the person confirm each medicine without guessing? | Yes / No | If no, improve label access first. |
| Can bottles be opened safely while seated? | Yes / No | If no, ask the pharmacist about easier containers. |
| Is there a backup plan for bad tremor days? | Yes / No | If no, create one before the next refill. |
Neutral action line: Use the first “No” as the next improvement target.
The “No Guessing” Rule: The Tiny Rule That Prevents Big Errors
The no guessing rule is blunt because medication errors do not reward elegance. If you cannot confirm it, you do not take it yet.
Not “probably.” Not “this feels like the blue one.” Not “I’ve been taking it for years.” The rule is not meant to frighten anyone. It is meant to remove the pressure to perform certainty when the task is uncertain.
If You Cannot Read It, Do Not Take It Yet
If the label is unreadable, pause. Use the magnifier, talking label, phone camera zoom, large-print list, caregiver check, or pharmacy call. The bottle does not get a vote.
A small pause can prevent a large problem. I like to think of it as a drawbridge. When the fog rolls in, the bridge goes up until the harbor is clear.
If Your Hand Is Too Shaky, Pause Before Opening or Pouring
Tremor often worsens with stress, fatigue, rushing, hunger, or strong emotion. If your hand is shaking more than usual, change the task before forcing the hand.
Sit down. Use a tray. Rest your forearms. Open only one bottle at a time. Move the cat, the coffee, and the dramatic sleeve cuff out of the work zone. Tiny chaos counts.
If Two Bottles Feel Similar, Treat That as a System Failure
When 2 bottles feel nearly identical, the solution is not “remember harder.” The solution is to make them more different.
Use separate locations, tactile markers, rubber bands, high-contrast tape, large-print labels, or pharmacy packaging. The goal is not decoration. The goal is confirmation.
- Unreadable label means pause.
- Unsteady hand means change the setup.
- Similar bottles mean redesign the system.
Apply in 60 seconds: Write “No guessing” on a large card and place it near the medication area.

Reading Labels Safely: Build a Bigger, Louder, More Tactile System
Reading medication labels safely is not only about making words larger. It is about making the most important information available in more than one way.
A safer system gives the brain multiple confirmations: visual, tactile, auditory, spatial, and social. Think of it as a small choir. If one singer misses the note, the song still survives.
Ask the Pharmacy for Large-Print Labels
The FDA notes that pharmacists may be able to print prescription labels in larger type when reading the medicine label is difficult. Ask directly. Do not wait for the pharmacy to guess your access needs from across the counter. If you want the request to sound calm and specific, a low vision pharmacy help script can give you the words before the counter moment gets noisy.
Use plain language when asking: “I have low vision and a hand tremor. Can you provide large-print labels and review how I should take this medicine?”
Use Talking Prescription Labels When Available
Accessible prescription tools can read label information aloud. The American Foundation for the Blind describes options such as talking label systems and smartphone-based access to prescription information.
Some pharmacies and systems may support tools like ScripTalk or app-based label reading. Availability varies by pharmacy, location, insurance, and delivery method, so ask before assuming. The magic words are simple: “Do you offer accessible prescription labels?”
Make the Most Important Words Stand Out First
Not every word on the label has equal daily value. The most important routine words are usually the medicine name, dose, timing, route, warning instructions, and prescriber or pharmacy contact.
For many people, a large-print medication list is easier to read than a curved bottle label. Ask your pharmacist to help you create or confirm one. Keep it updated after each medication change. For label-specific setup ideas, see this guide to large-print prescription labels and how they fit into a safer refill routine.
Here’s What No One Tells You: Bigger Text Is Not Enough
Bigger text helps only if the lighting, contrast, angle, spacing, and fatigue level cooperate. A large label wrapped around a small round bottle may still be hard to scan.
Try placing the bottle on a dark or light contrast mat, depending on the bottle color. Use task lighting that points at the label without shining into the eyes. Glare is not brightness. Glare is brightness wearing a rude hat. If pill bottles are still difficult to visually separate, iPhone magnifier filters for pill bottles may help some readers test contrast before reaching for the cap.
Show me the nerdy details
Accessible medication confirmation works best when it reduces cognitive load. A person should not have to rotate a bottle repeatedly, decode small abbreviations, remember pill appearance from last month, and manage a shaky hand at the same time. Large print, audio labels, tactile markers, and fixed storage zones reduce the number of decisions required before each dose.
Pharmacy Prep List: What to Ask Before the Next Refill
- Can you provide large-print labels?
- Do you offer talking labels, QR code access, or accessible prescription information?
- Can this medicine be packaged by dose time?
- Can you use easy-open caps if no children are in the home?
- Can you explain what to do if a dose is missed?
Neutral action line: Bring this list to the counter or read it during a pharmacy phone call.
Tactile Sorting: Give Every Medicine a “Home Address”
A medication without a reliable home becomes a daily search party. And search parties are where mistakes sneak in wearing sensible shoes.
Tactile sorting gives each medicine a physical address. The point is not to make the shelf pretty. The point is to make the correct choice easier when vision is tired and the hand is not cooperating.
Use Raised Dots, Rubber Bands, Tape, or Shape Cues Carefully
APH ConnectCenter’s VisionAware resources note that medication containers can be marked with large print, braille, label tape, or raised markings that can be read by touch. That idea is powerful, but it needs consistency.
Do not use random markers that only make sense on a good day. Decide what each marker means. One raised dot might mean morning. Two rubber bands might mean bedtime. A wide strip of textured tape might mean “ask before taking.” Keep a written or audio key. For a more detailed tactile setup, review pill bottle tactile label placement before turning every bottle into a tiny Braille-adjacent sculpture garden.
Separate Look-Alike Bottles Before They Become a Problem
Look-alike bottles are not harmless. They are future confusion waiting politely.
Separate similar bottles by location, container type, or tactile marker. If 2 medicines are both white tablets in orange bottles, do not store them shoulder-to-shoulder like twins plotting a prank.
Keep Morning, Noon, Evening, and Bedtime Zones Physically Different
Time-based zones work well when they are physically distinct. A drawer divider, tray, basket, or shelf row can become a medication map.
For example, morning medicines might live in a left tray with a rough-textured edge. Evening medicines might live in a right tray with a smooth edge. Bedtime medicines might be stored separately near the bedtime routine, but only if that location is safe, dry, and out of reach of children or pets. If bedtime is where glasses, drops, phone, and water already compete for territory, a low vision bedside organization system can keep the nightstand from becoming a small island nation with poor border control.
- Use one meaning per marker.
- Separate look-alike bottles.
- Keep a large-print or audio key.
Apply in 60 seconds: Move the most frequently confused bottle away from its look-alike today.
-
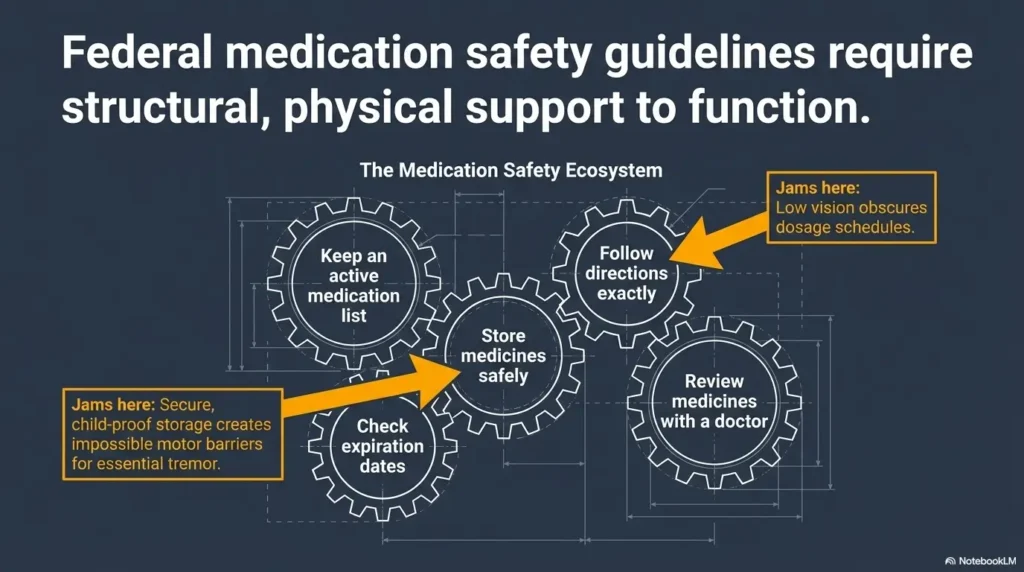
FDA: 5 Medication Safety Tips for Older Adults
This official FDA resource supports the article’s core medication-safety advice, including taking medicines as prescribed, asking health professionals before making changes, storing medicines safely, and avoiding risky dosing mistakes.
-
National Eye Institute: Low Vision
This National Eye Institute page explains how low vision can make everyday activities, including reading, more difficult even when regular glasses, contact lenses, medicine, or surgery cannot fully correct vision loss.
-
MedlinePlus Medical Encyclopedia: Essential Tremor
This MedlinePlus overview explains essential tremor, including involuntary shaking during action-based tasks such as holding objects, writing, or eating, which directly supports the article’s medication-handling safety guidance.
Dosing With Tremor: Stabilize the World Before You Stabilize the Hand
Essential tremor can make people feel as though the hand is the problem. Sometimes the better fix is to stabilize everything around the hand first.
The table, chair, tray, lighting, bottle position, and timing all matter. A shaky hand over a hard floor is risky. A shaky hand over a soft towel on a tray is still inconvenient, but less theatrical.
Use a Tray, Towel, or Non-Skid Mat as the “Landing Zone”
Create a dosing landing zone. Use a tray with a rim, a clean towel, or a non-skid mat. The goal is to catch dropped pills, stop rolling, and keep one task contained.
For many people, this one change reduces panic. When a pill drops onto a tray, it is a small event. When it drops onto a patterned rug, it becomes a treasure hunt with medical stakes.
Sit Down Before Opening Bottles or Handling Drops
Sitting reduces fall risk and gives both arms support. Rest your forearms on the table if that helps. Bring the bottle closer instead of reaching forward.
Do not dose while standing in a dim bathroom at 6:12 a.m. unless your routine has been designed for that. Bathrooms are excellent at adding moisture, glare, tile, and unnecessary suspense. For households where morning or nighttime bathroom routines are already risky, low vision nighttime bathroom safety deserves its own small audit.
Let’s Be Honest: The Kitchen Counter Is Not Always Your Friend
The kitchen counter is convenient, but it may also be cluttered, reflective, crowded, or busy. Dosing near coffee, crumbs, supplements, pet bowls, and mail can create confusion.
A dedicated medication spot does not need to be fancy. It needs 3 things: good light, low clutter, and a surface that stops small objects from escaping.
Mini Calculator: Your 3-Point Dosing Setup Check
Give yourself 1 point for each “Yes.”
- Can I sit while preparing the dose?
- Is there a tray, towel, or mat under the bottle?
- Can I confirm the medicine name before opening it?
Output: 3 points means the setup is ready. 1 to 2 points means improve the setup before dosing. 0 points means pause and ask for help.
Neutral action line: Raise the score by one point before your next dose.
Eye Drops, Liquids, and Tiny Pills: The High-Risk Mini Tasks
Some medications are hard because they are small. Others are hard because they require aim. Eye drops, liquids, and tiny pills deserve special treatment because they punish small errors.
These tasks are not “just medicine.” They are fine-motor events. Low vision and tremor can make fine-motor events feel like threading a needle during an earthquake that also wants you to remember breakfast.
Eye Drops Need a Different Setup Than Tablets
Eye drops often require identification, cap removal, hand positioning, head tilt, aim, and timing. That is a lot of choreography for one tiny bottle.
Ask your eye doctor or pharmacist whether an eye drop guide, assistive device, or specific technique is appropriate. Some people benefit from lying down or resting the hand against the face for stability, but technique should match the medication and clinician instructions.
Liquid Medicine Requires Better Lighting, Contrast, and Confirmation
Liquid medicine can be risky when the measuring line is hard to see. Ask whether an oral syringe, marked dosing cup, or pharmacy-provided measuring device is best for that medicine.
Never use a kitchen spoon for dosing. Spoons vary, and medicine is not soup. The soup will forgive you. The dose may not. If measuring tools are part of your daily routine, low vision measuring spoon strategies can also help you think through contrast, grip, and markings for non-medication kitchen tasks where accuracy still matters.
Tiny Pills Should Not Be Split Unless the Pharmacist Says It Is Safe
Some pills should not be split, crushed, or opened because they may be extended-release, coated, or designed to work in a specific way. Ask the pharmacist before changing the form of any medicine.
If a pill is too tiny to handle safely, ask about alternatives. Options might include a different strength, packaging, formulation, or dosing support. The answer depends on the medicine, so the pharmacist is your first practical ally.
Short Story: The Refill That Looked Like a Mistake
A woman I know once called her daughter because her “heart pill” had changed from round to oval after a refill. She was embarrassed, almost apologetic. The daughter wanted to say, “It’s probably fine,” because dinner was burning and the dog had stolen a napkin.
Instead, they called the pharmacy. The pharmacist confirmed it was the same medicine from a different manufacturer, then reviewed the dose. The call took less than 5 minutes. The relief lasted all week. That is the point of a good system: it makes caution feel ordinary, not dramatic.
Common Mistakes: Small Shortcuts That Create Medication Drift
Medication drift happens when the routine slowly moves away from the instructions. No one plans it. It begins with one shortcut, one busy morning, one “I’ll remember.”
For people managing low vision with essential tremor, drift can happen faster because each shortcut may feel like a reasonable adaptation. The problem is that reasonable adaptations need labels, boundaries, and backup checks.
Mistake 1: Keeping All Bottles in One Crowded Basket
A crowded basket feels tidy until it becomes a rummage zone. Rummaging increases handling, bottle confusion, dropped pills, and frustration.
Use smaller groups. Sort by time of day, purpose, or risk level, with pharmacist input when needed. Keep discontinued or expired medicines out of the active area.
Mistake 2: Trusting Memory After a Shaky or Painful Morning
Memory is not a reliable witness after stress. If the dose was difficult, record it immediately using a checkmark sheet, voice assistant, phone reminder, or caregiver-visible log.
The question is not “Should I be able to remember?” The question is “Can the system remember for me?” A low vision medication tracker printable can turn that question into a simple, visible record instead of a late-night debate with memory.
Mistake 3: Pouring Pills Into the Palm Without a Backup Surface
A palm is not a stable pharmacy workstation. Pills can bounce, stick, roll, or disappear.
Pour over a tray or towel. Open one bottle at a time. Close it before opening the next. This may add 20 seconds, but it can save 20 minutes of crawling around under furniture muttering ancient curses.
Mistake 4: Removing Labels, Boxes, or Inserts Too Soon
Boxes and inserts may contain important instructions, especially for eye drops, inhalers, topical medicines, and new prescriptions. Do not discard them until the medicine is clearly identified and the routine is understood. When inserts feel visually punishing, use a separate strategy for reading medicine leaflets with low vision instead of tossing the paper into the drawer of future regret.
Mistake 5: Letting a Caregiver “Fix” the System Without Explaining It
A caregiver may create a beautiful system that fails the moment they leave. The person using the medicine must understand the layout, markers, and backup plan.
- Reduce rummaging.
- Record hard doses immediately.
- Explain every new marker or storage change.
Apply in 60 seconds: Remove discontinued, expired, or unclear bottles from the active medication area and set them aside for pharmacist review.
Don’t Do This: Safety Traps That Feel Efficient
Some medication shortcuts feel efficient because they reduce friction today. Unfortunately, they may also remove the very cues that prevent tomorrow’s mistake.
Efficiency is not the enemy. Fragile efficiency is. A system is too fragile when it works only in perfect lighting, with perfect memory, on a perfect hand day, under a perfect moon. Very poetic. Terrible for dosing.
Do Not Combine Different Pills in One Unlabeled Container
Combining different pills in one unlabeled container can make identification difficult or impossible, especially after a spill, refill, dose change, or caregiver handoff.
If you use a pill organizer, fill it according to clinician or pharmacist guidance, keep the original bottles available, and make sure the organizer is labeled clearly enough for the person using it.
Do Not Take Medicine From a Bottle You Cannot Confirm
If a label is damaged, smeared, too small, missing, or confusing, pause. Call the pharmacy. Confirm the medication before taking it.
Do Not Change Dose Timing Because the Routine Feels Annoying
Medication timing can affect safety and effectiveness. Some medicines must be taken with food, away from other medicines, at bedtime, or at consistent intervals.
If timing is hard, ask the pharmacist or prescriber whether the schedule can be simplified. Do not freelance the schedule unless your health care team approves it.
Do Not Use Someone Else’s Assistive Setup Without Testing It
A system that works beautifully for one person may fail for another. One person prefers tactile dots. Another needs audio labels. One can use a phone camera. Another finds phone scanning exhausting.
Test the setup with the actual person, actual medicines, actual lighting, and actual shaky-hand conditions. Medication safety is not a showroom. It is Tuesday morning.
Decision Card: Original Bottles vs Pill Organizer
Use original bottles when:
- Medicine changes often.
- The pill appearance needs confirmation.
- Instructions vary by dose.
Consider a pill organizer when:
- The schedule is stable.
- Compartments are large and tactile.
- A pharmacist or caregiver can help verify filling.
Neutral action line: Ask the pharmacist which setup fits the current medication list.
Caregiver Checks: Help Without Creating Dependence or Confusion
Good caregiver support is a handrail, not a takeover. It helps the person move through the routine with more safety and less shame.
The best caregiver checks are specific, respectful, and repeatable. They do not begin with “Are you fine?” because “fine” is where useful details go to nap.
Ask Functional Questions, Not Vague Ones
Instead of asking, “Did you take your medicine?” ask questions that reveal system problems:
- “Was any label hard to read this week?”
- “Did any bottle feel too hard to open?”
- “Did your hand shake more during morning or bedtime doses?”
- “Did any pill look different after the refill?”
- “Did you skip, delay, or wonder about any dose?”
Watch the Task Once Before Redesigning the Whole Routine
Observation is better than assumption. Watch the person read the label, open the bottle, prepare the dose, record the dose, and put the medicine away.
You may discover the real problem is not the label. It might be glare from the window, a cap that requires too much grip, a pill that rolls, or a reminder alarm that sounds during a noisy part of the day. For a wider home routine view, low vision medication management can help caregivers notice the difference between a one-bottle problem and a whole-system wobble.
Create a Backup Plan for Bad Tremor Days
Bad tremor days deserve a written plan. Decide who to call, what to pause, what tools to use, and when to contact the pharmacist or clinician.
The backup plan should protect independence, not punish difficulty. A good plan says, “Here is what we do when the hand is having a loud day.”
- Ask specific questions.
- Watch one real routine.
- Create a backup plan before the bad day arrives.
Apply in 60 seconds: Ask, “Which bottle felt least safe this week?” and improve that one first.
When to Seek Help: Red Flags That Deserve a Human, Not a Hack
Some problems should not be solved with better tape, brighter lamps, or a clever tray. They need a pharmacist, clinician, emergency service, or rehabilitation professional.
Knowing who to call is part of the safety system. It removes the awful little pause where everyone wonders whether the problem is “serious enough.”
Call a Pharmacist When Labels, Doses, Refills, or Pill Appearance Changes
Call the pharmacist if a pill looks different, a label is hard to read, a refill seems wrong, a dose instruction is unclear, or you are unsure whether 2 medicines can be taken near each other.
Pharmacists can also discuss large-print labels, accessible prescription information, easier containers, packaging options, and what to do after a missed dose.
Contact a Clinician for New Confusion, Falls, Severe Dizziness, or Missed Doses
New confusion, repeated missed doses, falls, faintness, severe dizziness, new weakness, or medication side effects should be discussed with a clinician. These may signal a medication problem, health change, or safety risk that needs more than a household workaround. When several medicines are involved, polypharmacy and vision problems can make the safety picture more complicated than one confusing bottle.
Seek Urgent Care for Allergic Reaction, Chest Symptoms, Severe Weakness, or Suspected Overdose
Seek urgent help for trouble breathing, swelling of the face or throat, chest pain, severe weakness, fainting, severe allergic reaction, or suspected overdose. When in doubt, use emergency services or poison control guidance in your area.
Ask About Vision Rehabilitation or Occupational Therapy When Workarounds Stop Working
Low vision rehabilitation and occupational therapy can help people adapt everyday tasks. MedlinePlus also notes that occupational therapy may help people manage daily challenges caused by tremor.
This is not an admission of defeat. It is calling in the person who knows where the better tools are kept. For reading-heavy routines, a stand magnifier for tremor may be one of the tools worth asking about, especially when hand-held magnifiers add more shake than clarity.
FAQ
What is the safest way to read medication labels with low vision?
Use more than one confirmation method. Ask for large-print labels, keep a large-print medication list, use strong task lighting without glare, consider audio or talking label tools, and call the pharmacy if anything is unclear. The safest method is the one that lets you confirm the medicine name, dose, and timing before opening the bottle.
How can someone with essential tremor open pill bottles more safely?
Sit down, use a stable table, rest the forearms if helpful, and open one bottle at a time over a tray or towel. Ask the pharmacist about easier-to-open containers if child-resistant caps are difficult and if children are not present in the home. Never force a cap while standing over a hard floor if the hand is shaking badly.
Are pill organizers safe for people with low vision?
They can be helpful, but only when filled correctly, labeled clearly, and matched to the person’s vision, touch, memory, and medication schedule. Large compartments, tactile markers, and caregiver or pharmacist verification may help. Keep original bottles available so medicines can be confirmed if questions arise.
What should I do if my pill looks different after a refill?
Pause and call the pharmacy before taking it. Pill appearance can change when the manufacturer changes, but you should not guess. Ask the pharmacist to confirm the medicine name, strength, directions, and reason for the appearance change.
Can a pharmacist help with large-print or accessible prescription labels?
Yes, pharmacists may be able to help with large-print labels, accessible prescription information, easier containers, medication reviews, refill questions, and missed-dose instructions. Services vary, so ask directly and describe both the low vision and tremor challenges.
How do I make eye drops easier with shaky hands and poor vision?
Use a seated or stable position, confirm the bottle before opening it, improve lighting and contrast, and ask your eye doctor or pharmacist about eye drop guides or techniques. Do not touch the dropper tip to the eye, fingers, or skin unless your clinician has instructed otherwise. If drops are repeatedly missed, ask for help quickly.
Should a caregiver pre-sort medication every week?
Sometimes, but it depends on the medicine list, dose changes, cognition, vision, tremor severity, and the person’s preferences. If a caregiver sorts medication, the system should be clearly labeled, verified, and explained. The person taking the medicine should still know how to pause and ask for help if something looks wrong.
What should I do after missing a dose?
Do not automatically double the next dose. Check the medication instructions and call the pharmacist or prescriber if the missed-dose plan is unclear. Different medicines have different rules, and guessing can be risky.
Next Step: Make One Bottle Safer Today
The hook at the beginning was not really about one stubborn bottle. It was about that moment when the label, the hand, and the clock all ask too much at once.
You do not have to rebuild the whole medication routine today. In fact, please do not turn the medicine area into a 4-hour home improvement opera. Start with one bottle.
Choose the Riskiest Medicine First
Pick the medicine most likely to cause confusion. It may be the one with the smallest label, the bottle that looks like another bottle, the eye drop used at night, or the pill that changed after a refill.
Add One Large-Print, Tactile, or Talking Identifier
Add one clearer confirmation method. That might mean asking for a large-print label, adding a tactile marker, moving the bottle to its own tray, or setting up an audio label option.
Write One “If I’m Not Sure” Rule and Place It Near the Medicine
Write a simple rule in large print:
If I am not sure, I pause and call the pharmacist before taking it.
That sentence is small, but it changes the room. It removes the pressure to be brave when what you need is confirmation.
Medication Safety Setup: Tier Map
| Tier | What changes | Best for |
|---|---|---|
| Tier 1 | Better light and clear surface | Mild reading or handling trouble |
| Tier 2 | Large-print list and fixed bottle zones | Multiple daily medicines |
| Tier 3 | Tactile markers and tray-based dosing | Low vision plus tremor |
| Tier 4 | Talking labels or accessible pharmacy packaging | Hard-to-read labels or frequent confusion |
| Tier 5 | Caregiver verification and clinician review | Missed doses, falls, confusion, or high-risk medicine |
Neutral action line: Choose the lowest tier that reliably prevents guessing.
Conclusion
Low vision with essential tremor does not mean medication independence is over. It means the routine needs more design and less wishful thinking.
The safest routines are usually ordinary-looking. A tray. A large-print list. A pharmacy call. A tactile marker. A chair pulled close to the table. A caregiver who asks better questions. A rule that says no bottle gets swallowed on a hunch.
Within the next 15 minutes, choose one medication bottle and improve one thing: the label, the location, the surface, the lighting, the tactile cue, or the backup plan. Not everything. One thing. Safety often enters the house quietly, wearing sensible shoes and carrying a label maker.
Last reviewed: 2026-04.