
Vision changes after 45
Presbyopia vs Early Cataracts:
How Older Adults Can Tell the Difference
There is a particular kind of panic that arrives with a restaurant menu held under the table lamp, then farther away, then almost into the neighboring booth. You may laugh it off as “my arms are getting shorter,” but a quiet question often follows: is this normal aging vision, or could something else be starting?
This guide separates two common suspects: presbyopia, the age-related loss of near focusing, and early cataracts, the slow clouding of the eye’s natural lens. They can overlap, imitate each other, and make everyday tasks feel oddly slippery: pill labels, phone text, headlights, TV captions, stairs, receipts, and the tiny print on things clearly designed by woodland elves.
You will not diagnose your eyes at home, and you should not have to. What you can do is notice the pattern: near versus distance, sharp versus cloudy, light helping versus light hurting. That pattern can save time, reduce guessing, and make your next eye exam far more useful.
Spot the pattern
Learn whether blur is mainly near, far, cloudy, or glare-heavy.
Prepare for the exam
Turn vague complaints into clear notes your eye doctor can use.
Protect daily safety
Know when driving, medication reading, and home routines deserve attention.
👓 Tiny clue, big value: If readers help close-up text but headlights still bloom like fireworks, you may be dealing with more than one vision issue.
Snapshot
This article is for adults 45+, older adults, and family caregivers who are trying to sort out near-vision trouble, cloudy vision, glare, faded colors, or night-driving hesitation. You will learn practical home clues, what those clues can and cannot tell you, when to seek help, and how to bring a simple two-column symptom note to an optometrist or ophthalmologist.
Table of Contents
Safety First: When Vision Changes Are Not “Wait and See”
Presbyopia and early cataracts are common, but vision changes should never be treated like a crossword puzzle you solve alone at the kitchen table. Your eyes are connected to driving, cooking, stairs, medication reading, bill paying, and the quiet confidence of moving through a room without bracing for surprises.
This guide is educational. It can help you describe patterns and prepare for an eye exam, but it cannot diagnose presbyopia, cataracts, glaucoma, diabetic eye disease, macular degeneration, dry eye, medication effects, stroke-related vision changes, or a prescription problem.
Sudden vision changes deserve faster action than gradual blur. If something changes quickly, hurts, flashes, doubles, or feels dramatically different from yesterday, do not file it under “aging.” Aging is gradual. Emergencies often have sharper elbows.
Key takeaway
- Gradual near blur often points toward presbyopia, but not always.
- Cloudy, glare-heavy, faded, or dim vision may suggest cataracts or another eye issue.
- Sudden vision loss, eye pain, new flashes, new floaters, or a curtain-like shadow should be treated urgently.
Apply in 60 seconds: Write down whether the change was sudden or gradual. That single word matters.
Urgent symptoms need urgent care
Seek urgent medical guidance for sudden vision loss, eye pain, new flashes or floaters, a dark curtain or shadow, sudden double vision, severe headache with vision changes, or vision changes after an injury. Those symptoms can signal problems that are not solved by stronger readers or brighter lamps.
For an older adult living alone, the safety stakes rise. A label misread at 9 p.m., a stair edge missed in dim light, or a glare-blinded turn while driving can change a week very quickly. Vision is not vanity. It is infrastructure.
Gradual changes still deserve a plan
Gradual symptoms are less dramatic, but they still deserve attention when they persist. If you keep enlarging phone text, avoiding night driving, buying stronger drugstore readers, or asking someone else to read medicine labels, your eyes are already sending a memo.
The goal is not to panic. The goal is to stop guessing. A comprehensive eye exam can separate a focusing issue from lens clouding, retina problems, dry eye, or other conditions that can wear the same blurry disguise.
Start With the “Where” of Blur, Not the Word “Blurry”
“Blurry” is a useful word at home and a slippery word in the exam room. It can mean fuzzy letters, dim rooms, haze over distance, glare around headlights, double images, poor contrast, watery eyes, or tired focusing after a day of screens.
So start with location. Where does the blur live? Is it on your phone, in the newspaper, on a pill bottle, across the room, on road signs, in bright sunlight, or around headlights at night?
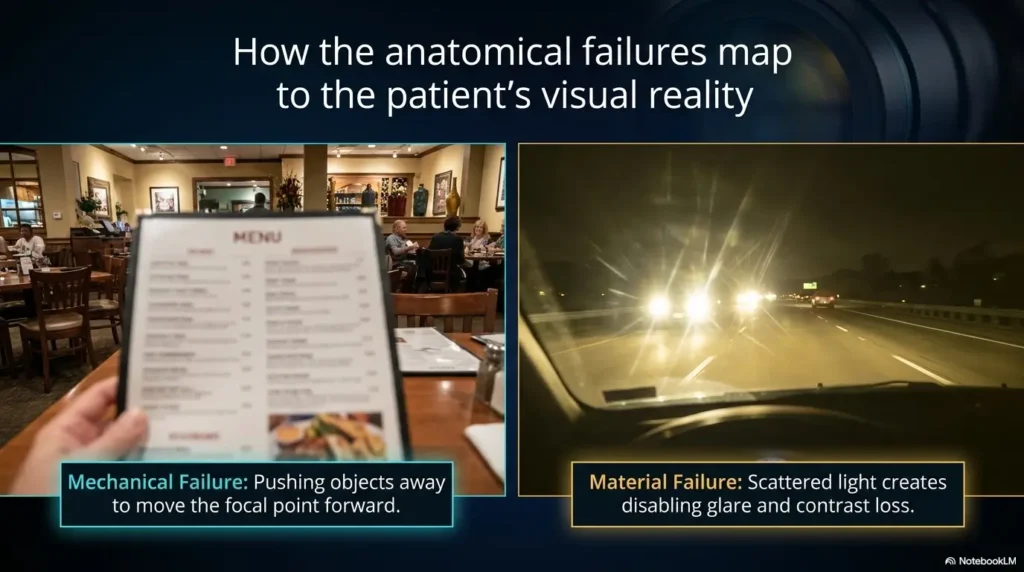
That “where” is the first breadcrumb. Presbyopia usually makes near tasks harder. Early cataracts often affect clarity, glare, color brightness, and contrast more broadly. There are exceptions, but this first sorting step keeps you from tossing every symptom into one messy drawer.
Near blur points toward presbyopia first
Presbyopia commonly appears when you read a menu, check a phone, thread a needle, look at a receipt, read a medicine label, or work on something close to your face. The page may look clearer when you move it farther away. You may need more light. You may remove your distance glasses to read, depending on your prescription.
The classic sign is not mysterious. It is the slow migration of books, phones, and menus away from your nose. At first, it feels like a small inconvenience. Then one day the print is at full arm extension and your elbows have joined the vision care team.
Distance haze deserves a different level of suspicion
If road signs, TV captions, faces across the room, or distance details look hazy or washed out, do not assume it is just presbyopia. Presbyopia is mainly a near-focusing issue. Distance haze can come from cataracts, prescription changes, dry eye, cornea issues, retina disease, or other causes.
Early cataracts may feel as if someone turned down the room’s contrast. Not black-and-white blindness, not a movie scene with dramatic music, just a low-grade fog that makes the world less crisp. People often adapt without noticing until driving, reading, or watching television becomes more effortful.
The 14-inch clue: why arm’s length matters
Many near tasks happen around 14 to 16 inches from the eyes. With presbyopia, that comfortable zone starts to slip away. You may hold a book farther out, lift your chin, tilt your head, or search for a brighter patch of light.
This clue is not a diagnosis. It is a pattern. If moving close text farther away makes it clearer, presbyopia becomes more likely. If the print still looks gray, low-contrast, or cloudy even with readers and good lighting, the story needs a professional reader, preferably one with a slit lamp and a calm chair.
Quick pattern table
| What you notice | More consistent with | Next smart move |
|---|---|---|
| Phone text clears when held farther away | Presbyopia | Try proper near correction and schedule an exam if persistent |
| Headlights create halos or harsh glare | Cataracts or other eye issues | Mention night driving at the exam |
| Colors look faded or yellowed | Possible cataract-related change | Ask for lens and retina evaluation |
| One eye is much worse than the other | Needs professional evaluation | Book an eye exam rather than guessing |
Presbyopia Feels Like Your Arms Got Shorter
Presbyopia is one of the most democratic inconveniences of midlife. It does not care how healthy you eat, how many stairs you climb, or whether you still own concert T-shirts from 1987. Around midlife, the eye’s natural lens gradually loses flexibility, and close focusing becomes harder.
The key word is near. Presbyopia often shows up first during reading, phone use, crafts, mail sorting, cooking instructions, medication labels, and close repair tasks. It may be worse when you are tired or in low light.
For many people, the first fix is simple: reading glasses, bifocals, progressives, contact lens options, or prescription adjustments. But simple does not mean casual. A proper exam can confirm whether near blur is truly presbyopia or part of a larger vision change.
Phone text, menus, and pill labels become the early battleground
Near-vision trouble often becomes obvious in embarrassingly ordinary places. The restaurant menu looks printed for ants. The phone looks fine until the room is dim. The pill bottle label seems to have been designed by a committee that feared generous font sizes.
Caregivers may notice behavior before the older adult names the problem. A parent may stop reading novels, ask others to read labels, use a flashlight more often, or set the phone font to a heroic size. None of this is shameful. It is information.
A useful clue: if near text improves quickly with reading glasses or by holding it farther away, presbyopia is likely part of the picture. But if the text remains faded, dim, or low-contrast, keep the notebook open. Cataracts and other issues may be sitting in the same room.
Brighter light helps, but only up to a point
Many aging eyes need more light for close tasks. That can be normal. A brighter reading lamp, better task lighting, or a matte surface that reduces glare may make reading more comfortable.
But light is a clue with two faces. If brighter light helps close work, presbyopia may be the main nuisance. If bright light creates glare, halos, washed-out vision, or discomfort, cataracts, dry eye, cornea problems, or light sensitivity may need attention.
This is why “I just need more light” can be both true and incomplete. The question is whether light improves clarity or attacks it.
Readers help fast, but they do not solve everything
Drugstore readers can be useful for presbyopia, especially for people who need simple magnification for close work. They are affordable, easy to test, and sometimes wonderfully effective. A pair in the kitchen, a pair by the bed, and a pair mysteriously lost in the couch is practically a midlife rite.
But readers are not diagnostic tools. They do not check eye pressure, retina health, cataract severity, diabetic eye disease, macular degeneration, or whether your two eyes need different prescriptions. They magnify. They do not investigate.
Key takeaway
- Presbyopia usually starts with near tasks.
- Readers may help quickly, especially for close print.
- Readers cannot rule out cataracts or other eye disease.
Apply in 60 seconds: Test whether near text improves with readers, but write down anything readers do not fix.
Early Cataracts Whisper Through Glare Before They Shout Through Blur
Cataracts are often imagined as obvious cloudiness, but early cataracts can be quieter. They may start as glare, dimness, faded color, or reduced contrast. The room is still there. The road is still there. Yet the visual world feels less polished, as if someone smudged the glass between you and the day.
A cataract is clouding of the eye’s natural lens. As the lens becomes less clear, light can scatter inside the eye. Scattered light can make headlights, lamps, sunlight, or bright windows feel harsher. Reading may also become harder because contrast drops, not because the print is simply too close.
The trouble is that gradual change is easy to normalize. People adapt by driving less at night, sitting closer to the TV, turning on more lamps, avoiding glossy mail, or saying “I’m fine” while quietly redesigning their life around dimmer vision.
Night driving becomes the “truth serum”
Night driving reveals vision problems because it demands contrast, glare control, depth judgment, and fast decision-making all at once. Early cataracts can make headlights bloom, streetlights halo, lane markings fade, and rain-slick roads look like a silver puzzle.
Many people first notice the problem not as blur, but as hesitation. They stop volunteering to drive after dinner. They avoid unfamiliar routes. They grip the wheel harder. They complain that “everyone’s headlights are too bright now.” Sometimes the headlights are brighter. Sometimes the lens inside the eye is scattering more light. Both can be true.
Night-driving changes deserve respect. They affect the driver, passengers, pedestrians, and the person crossing the parking lot with a grocery bag and too much faith in reflective paint.
Colors start losing their music
Cataracts can make colors seem faded, yellowed, or less bright. Whites may look cream. Blues may feel dull. The world may not look dark, exactly, but less alive. The volume knob on color gets turned down one tiny notch at a time.
This can be hard to catch because your brain adjusts. You do not compare today’s blue towel with the blue towel of six years ago. You simply live inside the new version of blue. After cataract treatment, some people are startled by how bright colors look again.
Faded color alone is not proof of cataracts. But faded color plus glare, cloudy vision, night-driving trouble, or frequent prescription changes deserves an eye exam.
One eye may tell a different story
Cataracts can develop at different rates in each eye. One eye may see clearer, brighter, or sharper than the other. That difference can hide in daily life because both eyes work together, smoothing over the weaker partner like a polite duet.
At home, you can safely compare one eye at a time while sitting still, looking at a familiar object, and avoiding any risky task. Do not do this while driving or walking. Cover one eye, then the other, and notice whether the same scene looks equally clear, bright, and comfortable.
If one eye is suddenly worse, seek urgent guidance. If one eye is gradually worse, schedule an exam. Either way, one-eye differences are not a contest to win with denial.
The Kitchen-Table Test: Four Safe Clues to Compare at Home
A home check should be gentle, safe, and humble. It should not pretend to replace an exam. Think of it as gathering clues, not delivering a verdict. You are not the judge. You are the note-taker with a lamp, a cereal box, and reasonable boundaries.
Choose a time when you are not rushed. Sit at a table. Use familiar objects. Avoid driving, stairs, sharp tools, or anything that turns a vision experiment into a safety incident. The goal is to compare near tasks, distance clarity, glare, and one-eye differences.
Read a label close up
Pick a medicine label, food package, mail notice, or receipt. Hold it at your usual reading distance. Then move it farther away. Try reading glasses if you already use them. Notice whether the print becomes clear, merely bigger, or still gray and difficult.
Presbyopia clue: close text improves with distance, readers, or proper near correction. Cataract or contrast clue: text may remain dull, low-contrast, or cloudy even when magnified.
Look across the room
Look at a clock, TV caption, framed photo, calendar, or appliance display from across the room. Do not squint as your first move. Notice whether the object is sharp, hazy, ghosted, faded, or harder to read than it used to be.
Distance haze is less typical of pure presbyopia. It can be a prescription issue, cataracts, dry eye, retina disease, or another cause. That is why distance symptoms deserve a professional check, especially when they change daily routines.
Check glare in normal lighting
Use ordinary household lighting, not a flashlight pointed at your eyes. Notice whether lamps, window light, glossy paper, or a bright screen feel unusually harsh. Glare that feels new, worse, or paired with halos can be meaningful.
Glare is not automatically cataracts. Dry eye, cornea changes, medication effects, migraine, light sensitivity, and screen settings can all play a role. Still, cataracts are famous for making light scatter and misbehave.
Compare one eye at a time
While seated, cover one eye and look at the same object, then switch. Do not press on the eye. Do not test while moving. Notice differences in clarity, brightness, color, glare, or distortion.
A small difference between eyes is common, but a clear difference deserves attention. If the difference is sudden, urgent care is appropriate. If it is gradual, book an exam and bring your notes.
Home clue checklist
- Near print clears when held farther away.
- Readers help close-up text but not distance haze.
- Headlights, lamps, or sunlight feel unusually harsh.
- Colors look faded, yellowed, or dim.
- One eye sees noticeably worse than the other.
- Daily habits have changed: less reading, less night driving, more help with labels.
Don’t Blame Every Vision Change on “Just Getting Older”
“Just getting older” is sometimes true, but it is also a phrase that can hide treatable problems. It can turn a useful symptom into background noise. Older adults often minimize vision changes because they happen slowly, and families may not notice until behavior changes.
The better question is not “Am I getting older?” Of course you are. We all are, with varying degrees of grace and snack preferences. The better question is: “What changed, and is it affecting safety or daily life?”
Mistake: buying stronger readers again and again
Stronger readers may help for a while. But if you keep increasing strength and still struggle, the problem may not be simple near focusing. You may need a different prescription, better lighting, dry eye treatment, cataract evaluation, or a retina check.
Readers also have limits when the two eyes need different correction. Over-the-counter readers usually use the same power in both lenses. That may not match your eyes, especially if astigmatism or unequal prescriptions are involved.
Mistake: ignoring night-driving changes
Night-driving trouble is not a small lifestyle complaint. It can be a safety issue. If headlights feel harsher, lane lines vanish in rain, or you avoid dusk errands, do not wait until driving feels scary.
Family caregivers should listen for indirect phrases: “I don’t like driving after dinner,” “traffic feels worse now,” “the road paint is terrible,” or “I’ll go tomorrow morning.” Those may be preference, but they may also be vision clues wearing a cardigan.
Mistake: assuming cataracts only happen when vision is “terrible”
Early cataracts can be subtle. You may still pass through the day, read some things, watch TV, and recognize faces. The issue may be quality, not total loss: duller colors, more glare, less contrast, and more visual fatigue.
Waiting until vision is terrible can mean months or years of unnecessary struggle. Cataract surgery is not always needed early, but knowing what is happening helps you plan with less anxiety and fewer expensive guesses.
Key takeaway
- Repeatedly stronger readers are not a full plan.
- Night-driving changes should be treated as safety information.
- Early cataracts may show up as glare and contrast loss before obvious blur.
Apply in 60 seconds: Ask, “What task have I quietly stopped doing because seeing it became annoying?”
Short Story: The Menu Under the Lamp
Marilyn first blamed the restaurant. The print was tiny, the lighting was dramatic, and the menu seemed designed for owls with graduate degrees.
At home, she noticed the same thing with soup cans and pharmacy labels. Readers helped. Then came the second clue: headlights at night looked harsher, almost wet around the edges.
Her daughter did not argue. She simply asked Marilyn to write two columns for one week: close-up problems and light problems. The list was short, but clear. Menus, labels, and phone text sat in one column. Headlight glare and faded colors sat in the other.
At the eye exam, the note changed the conversation. Marilyn did need better near correction, but she also had early cataracts. The practical lesson was gentle: the right question was not “Which one is it?” It was “What pattern is my life already showing me?”
The Overlap Zone: When Presbyopia and Cataracts Both Show Up
Here is what no one tells you loudly enough: two things can be true. An older adult can have presbyopia and early cataracts at the same time. That overlap is why symptoms can feel confusing, and why a single pharmacy purchase may only solve half the problem.
Presbyopia changes focusing. Cataracts change lens clarity. A person may need readers for close work and still struggle with glare, faded colors, or cloudy distance vision. Treating one issue does not erase the other.
A new prescription may help, but not always enough
A new glasses prescription can sharpen vision when focusing or refractive error is part of the problem. It may make reading, TV, and driving clearer. For early cataracts, updated glasses may help for a while, especially if the cataract is mild.
But glasses cannot make a cloudy lens clear. If cataracts progress, the improvement from glasses may become limited. That is when people often say, “These glasses are better, but something still feels off.”
“Better” is not the same as “clear”
This is a useful phrase to bring to an eye exam. If readers make print bigger but not crisp, say that. If new glasses improve road signs but headlights still flare, say that. If TV captions look sharper but colors remain dull, say that too.
Doctors and eye-care professionals can use these distinctions. “Blurry” opens the door. Details turn on the lights.
Caregivers may see the overlap before the parent does
A parent may say they are fine while quietly changing routines. They may stop reading at night, avoid evening errands, sit closer to the TV, use more lamps, enlarge phone text, or ask for help with mail. These changes can be small enough to miss unless you know to look.
Use curiosity, not interrogation. Try: “I noticed the lamp is always on when you read now. Is the print harder, or is the light bothering you?” That question invites a useful answer without turning the kitchen into a courtroom.
Caregiver observation map
| Changed behavior | Possible meaning | Helpful question |
|---|---|---|
| Avoids menus or mail | Near blur, low contrast, or fatigue | “Is the print too small, or does it look faded?” |
| Stops driving after dusk | Glare, halos, contrast trouble | “Are headlights bothering you more lately?” |
| Keeps buying stronger readers | Presbyopia, prescription change, or more | “Do they make things clear or just bigger?” |
The Eye Exam Decodes What Home Clues Cannot
A home clue can point. An eye exam can measure. That difference matters. Presbyopia, cataracts, dry eye, glaucoma, diabetic eye disease, macular degeneration, medication effects, and prescription changes can overlap in real life, especially for older adults.
A comprehensive eye exam can include vision testing, refraction, eye pressure checks, slit-lamp evaluation, dilation, retina evaluation, and questions about symptoms and daily tasks. The exact exam depends on the provider and your situation.
Refraction checks the focusing problem
Refraction is the part of the exam that helps determine glasses or contact lens prescription. It can identify nearsightedness, farsightedness, astigmatism, and presbyopia-related correction needs.
If your main issue is near blur, refraction may lead to readers, prescription reading glasses, bifocals, progressives, or contact lens options. If vision still is not clear despite correction, that tells the provider to look deeper.
Dilated exam checks the lens and retina
Dilation allows the eye-care professional to examine internal eye structures more fully, including the lens and retina. This matters because cataracts are only one possible cause of blurry or dim vision.
Retina problems can affect central vision, reading, distortion, night vision, or blind spots. Glaucoma can affect peripheral vision. Diabetic eye disease can be silent until it is not. Dry eye can make vision fluctuate. A dilated exam helps sort the crowd.
Medicare, insurance, and exam expectations
Coverage depends on the plan, diagnosis, provider, and exam type. Routine vision exams, refraction fees, medical eye exams, and cataract-related visits may be treated differently. Before the appointment, ask whether the visit includes dilation, refraction, and medical evaluation if symptoms suggest more than routine glasses.
If cost is a concern, say so when scheduling. Ask what is covered, what may be billed separately, and whether you should bring medical insurance, vision insurance, or both. This avoids the thrilling little billing surprise nobody ordered.
Show me the nerdy details
Presbyopia happens because the eye’s natural lens becomes less flexible with age, making it harder to change focus for close objects. Cataracts involve clouding of that same natural lens, which can scatter light and reduce clarity, contrast, and color brightness. This is why the two conditions can feel related, but they are not the same problem.
A person with presbyopia may see distance clearly but struggle with close print. A person with cataracts may notice cloudy vision, glare, halos, faded colors, or trouble in low light. When both occur together, near tasks may improve with readers while glare and dimness remain. That mixed response is a clue worth bringing to an eye exam.
Treatment Paths: Readers, Prescriptions, Drops, or Cataract Surgery?
The best fix depends on the real cause. That sounds obvious until you have spent money on three pairs of readers, two lamps, one anti-glare screen protector, and a magnifier that now lives in a drawer with batteries from 2019.
Presbyopia care usually starts with optical correction. Cataract care depends on how much the cataract affects daily life. Other conditions need their own plan. Diagnosis is the money-saving step, not the expensive one.
Presbyopia options usually start simple
Options may include drugstore readers, prescription reading glasses, bifocals, progressives, contact lens strategies, or prescription drops in selected patients. Not every option fits every person, especially if there are other eye conditions, dry eye, medication concerns, or driving needs.
For many adults, a good pair of readers is enough for a while. For others, progressives or task-specific glasses make more sense. A person who uses a computer all day may need a different working distance than someone reading paperback novels in a chair.
For more practical near-vision strategies, this related guide on senior near vision problems can help readers think through everyday tasks and common fixes.
Cataract treatment depends on daily-life impact
Early cataracts may simply be monitored. Updated glasses, better lighting, glare reduction, or adjusted routines may help for a time. Cataract surgery is usually discussed when cataracts interfere with ordinary activities such as driving, reading, working, cooking, hobbies, or safe movement.
The decision is personal and medical. It should include your symptoms, exam findings, health history, visual needs, lens options, recovery expectations, costs, and risks. A patient who drives at night for work may have a different threshold than someone who rarely drives and reads comfortably.
If cataract surgery is already on the horizon, you may also find this internal guide on Medicare cataract surgery cost in 2026 useful for planning questions.
The best fix matches the real cause
Near blur from presbyopia may improve with readers. Cloudy vision from cataracts may not. Glare from dry eye may need tear-film care. Distortion from retina problems needs retina evaluation. Dizziness plus blur may involve medications or blood pressure. One symptom can have several doors behind it.
That is why a symptom timeline matters. You are not trying to impress the eye doctor with medical vocabulary. You are giving them clean data from real life.
Treatment path comparison
| Path | Often used for | Limitation |
|---|---|---|
| Drugstore readers | Simple near blur | Do not diagnose eye disease or unequal prescriptions |
| Prescription glasses | Near, distance, astigmatism, mixed needs | Cannot remove lens clouding |
| Prescription drops for presbyopia | Selected near-vision cases | Not right for everyone and requires professional guidance |
| Cataract surgery | Cataracts affecting daily life | Requires medical evaluation, planning, and risk discussion |
Vision Clue Flow: Near, Distance, Light, Safety
1. Near tasks
Phone text, menus, labels, receipts. If farther distance or readers help, presbyopia may be involved.
2. Distance clarity
TV, road signs, faces, room details. Haze or dullness deserves an eye exam.
3. Light behavior
If lamps help, note it. If lights glare, halo, or wash things out, note that too.
4. Safety trigger
Driving, stairs, cooking, and medication reading changes move the issue from annoying to important.
When to Seek Help or Stop Guessing
Vision changes become easier to manage when you separate routine scheduling from urgent action. Not every symptom is an emergency. Not every symptom can wait six months. The trick is knowing which lane you are in.
For gradual but persistent symptoms, schedule a comprehensive eye exam. For sudden, painful, or dramatic symptoms, seek urgent care. For safety-related changes, such as driving or medication reading, move sooner rather than later.
Schedule a routine eye exam if symptoms are gradual but persistent
Book an optometrist or ophthalmologist visit if readers no longer solve the problem, glare is worsening, colors look faded, night driving is harder, one eye seems different, or daily tasks are changing. A routine exam can still be important even when symptoms are not urgent.
Bring your glasses, readers, medication list, medical history, and symptom notes. If you have diabetes, a history of eye disease, eye surgery, steroid use, trauma, or a family history of glaucoma or macular degeneration, mention it clearly.
For home safety context, this related article on bedroom safety for seniors with poor vision can help families reduce risk while waiting for appointments or treatment.
Seek urgent care for sudden changes
Urgent symptoms include sudden vision loss, eye pain, flashes, new floaters, a curtain-like shadow, sudden double vision, trauma, severe headache with vision change, or sudden weakness or speech trouble with visual symptoms. Do not test readers first. Do not sleep on it and hope the morning is friendlier.
Sudden symptoms can come from serious eye or neurologic problems. Quick evaluation can protect vision and, in some cases, overall health.
Bring a symptom timeline, not just a complaint
“My vision is blurry” is a start. “My phone text got harder this year, readers help, but headlights started flaring two months ago and my left eye seems dimmer” is much more useful.
A timeline does not need to be elegant. It needs to be honest. Dates, tasks, lighting, one-eye differences, and what helps or does not help are enough.
Key takeaway
- Gradual symptoms deserve an eye exam when they persist or affect daily life.
- Sudden vision loss, pain, flashes, new floaters, or a curtain-like shadow deserves urgent attention.
- A symptom timeline helps the eye-care professional separate focusing, lens, retina, and safety issues.
Apply in 60 seconds: Put “sudden or gradual?” at the top of your vision note.
FAQ
Can presbyopia and cataracts happen at the same time?
Yes. Presbyopia is an age-related focusing change, while cataracts involve clouding of the eye’s lens. Many older adults can have both, which is why symptoms may feel mixed.
How can I tell if I need readers or have cataracts?
Readers usually help near blur from presbyopia. Cataracts may cause cloudy vision, glare, halos, faded colors, or trouble seeing at night. An eye exam is the only reliable way to separate them.
Do cataracts make reading harder too?
They can. Cataracts may reduce contrast and clarity, so reading can become harder even with good lighting or readers. If text gets bigger but not clearer, mention that at your exam.
Is blurry vision after 45 always presbyopia?
No. Presbyopia is common after midlife, but blurry vision can also come from cataracts, dry eye, diabetes-related eye disease, glaucoma, macular degeneration, medication effects, or an outdated prescription.
Are early cataracts dangerous?
Early cataracts are often gradual, but they can still affect driving, falls, reading, and quality of life. The bigger risk is ignoring symptoms that change daily safety.
Can new glasses fix early cataracts?
Sometimes a new prescription helps for a while. Glasses can improve focusing, but they cannot remove lens clouding. If cataracts progress, surgery may eventually be discussed.
Why is night driving suddenly harder?
Night driving can reveal glare, halos, reduced contrast, cataracts, dry eye, or prescription changes. It is worth discussing with an eye-care professional, especially if the change is new.
Should I see an optometrist or ophthalmologist?
Either can perform eye exams and identify many causes of vision change. An ophthalmologist is a medical doctor and surgeon, often involved when cataracts, surgery, or complex eye disease need evaluation.
Do the Two-Column Vision Note Tonight
The most useful next step is not buying another gadget. It is writing a clear note. In 15 minutes, you can create a simple two-column record that turns a foggy complaint into a practical exam conversation.
Use one column for near tasks and one column for distance and light. Do not overthink it. You are not writing a medical memoir. You are leaving breadcrumbs for someone trained to read them.
Column one: near tasks
Write what happens with phone text, books, menus, medicine labels, sewing, receipts, mail, cooking directions, and computer work. Note whether readers help, whether distance helps, and whether brighter light improves clarity.
Column two: distance and light
Write what happens with TV captions, road signs, faces across the room, night driving, glare, halos, sunlight, lamps, and color brightness. Note whether one eye seems worse or whether symptoms change during the day.
Two-column vision note template
| Near tasks | Distance and light |
|---|---|
| Phone text: | TV captions: |
| Menus or labels: | Road signs: |
| Readers help? Yes / No / Somewhat | Headlight glare? Yes / No / New |
| Better with more light? Yes / No | One eye different? Yes / No |
Bring the note to your next eye exam
Bring the note, your current glasses, any readers you use, your medication list, and your questions. Tell the scheduler if you are having glare, night-driving trouble, cloudy vision, or one-eye differences, not just “I need new glasses.”
That small distinction can change the appointment from a quick prescription conversation into a fuller vision-health check. The whole point of this article is simple: presbyopia and early cataracts can feel similar from the inside, but your daily-life clues can help the right professional look in the right direction.
Tonight, choose one label, one distant object, one light source, and one quiet comparison between eyes. Write down what you notice. In a world that loves complicated answers, this is refreshingly small: one note, 15 minutes, and a clearer path toward safer sight.
Key takeaway
- Near blur, distance haze, glare, and one-eye differences tell different stories.
- The safest answer comes from an eye exam, not a pharmacy aisle diagnosis.
- A two-column note can make your appointment faster, clearer, and more useful.
Apply in 60 seconds: Start the note now with two headings: “Near” and “Distance/Light.”
Last reviewed: 2026-05