


Normal-Tension Glaucoma After 60: Silent Vision Loss, Key Tests, and Treatment Costs on Medicare
Your eye pressure can look “perfect” on the screen while tiny chunks of your world are already missing. That’s the quiet trap of normal-tension glaucoma after 60: you pass quick pressure checks at the optical shop, but the optic nerve is thinning, and Medicare paperwork feels just as confusing as the diagnosis.
Left alone, this slow damage can cost you safe driving, confident reading, and the independence you’ve spent decades building. If you’re not sure whether new vision quirks are just getting older or something more serious, this guide pairs well with our overview of when age-related eye changes signal real disease.
This guide helps you translate normal-tension glaucoma after 60 into plain English, see which tests (visual fields, OCT scans, full dilated exams) actually protect your optic nerve, and estimate what Medicare Part B is likely to pay—and what you’re likely to owe—before you’re sitting at the front desk. It’s built from current Medicare rules, real-world fee ranges, and the testing patterns glaucoma specialists use every day.
Here’s where normal-tension glaucoma gets unusually sneaky.
Here’s how to bring it into the light—clinically and financially.
First, get clear on what it actually is.
Normal-tension glaucoma after 60 is a form of open-angle glaucoma where the optic nerve is damaged even though eye pressure readings stay in the statistically “normal” range. It tends to steal peripheral vision first, progresses silently over years, and requires specific tests and ongoing monitoring to slow or prevent further vision loss.
In the next scroll, you’ll:
- Spot early patterns that pressure-only screenings miss.
- Learn which tests to ask for and what they feel like.
- Roughly map your Medicare Part B costs for exams, OCT, and visual fields.
- Build small, repeatable habits that defend both your sight and your budget.
Table of Contents
What is normal-tension glaucoma after 60, in plain English?
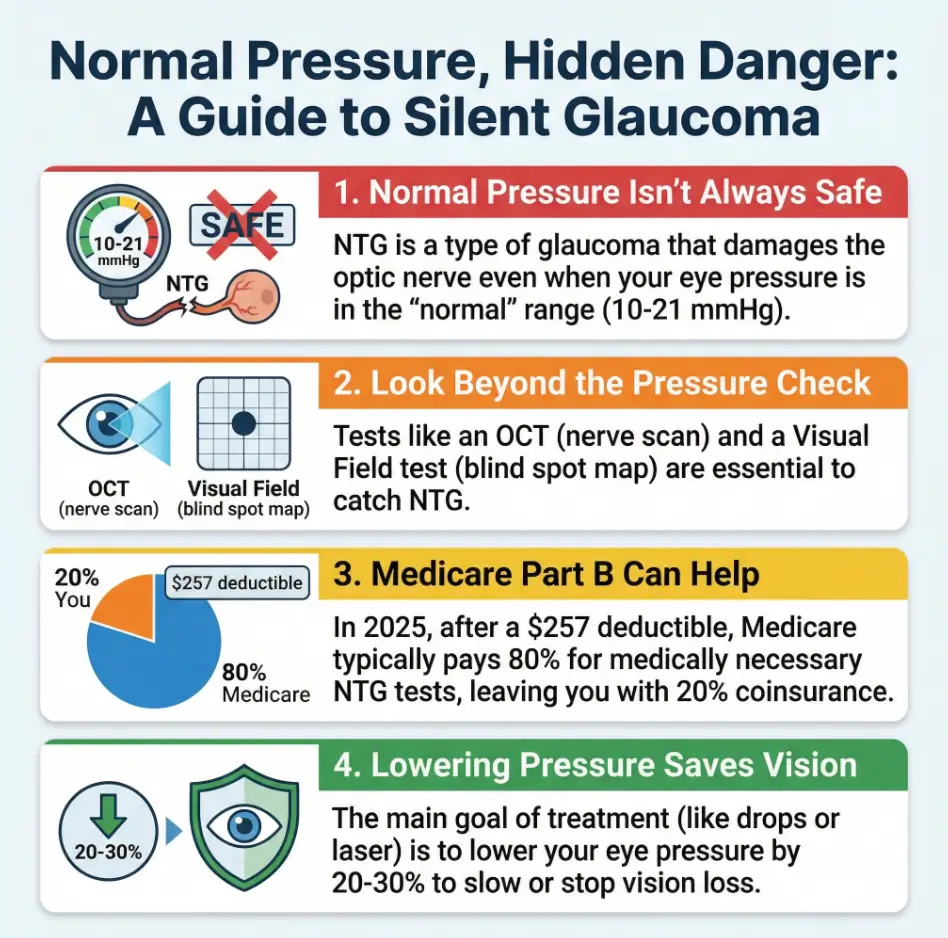
Normal-tension glaucoma (NTG) is glaucoma that damages the optic nerve even though your eye pressure reads in the “normal” range, usually between 10 and 21 mmHg. The drainage angle of the eye is open, there’s no obvious blockage, but the nerve still thins and the visual field narrows over time.
Think of your optic nerve as a fiber-optic cable. With classic glaucoma, the pressure inside the eye is too high and crushes the cable from the outside. With normal-tension glaucoma, the pressure is “fine” on paper, but the cable is still being starved or stressed—often from subtle blood-flow issues, fragile nerves, or pressure spikes that happen at night when nobody is measuring.
Researchers estimate that up to half of open-angle glaucoma in some populations looks like normal-tension glaucoma, and it’s particularly common in East Asian countries. In the US, it often shows up in people in their 60s and 70s who have “normal” pressure but tell a familiar story: “My glasses prescription keeps changing, I’m bumping into things on one side, and my eye doctor suddenly looks very serious while staring at my nerve photos.” It’s a classic example of how glaucoma can masquerade as “normal aging” symptoms, a theme we unpack more in our guide to glaucoma vs normal aging.
Left alone for years, NTG can cause permanent blind spots and, in some cases, legal blindness after 70. But most people who are diagnosed early, monitored properly, and treated consistently maintain useful vision for the rest of their lives.
Personal moment: many patients describe the diagnosis visit as “the day the word glaucoma finally landed,” not when the disease started. The disease had been whispering for years; the clinic visit was just when someone finally listened.
- Eye pressure between 10–21 mmHg doesn’t guarantee safety.
- The optic nerve and visual field tell the real story.
- Early treatment can slow or stop vision loss in many people.
Apply in 60 seconds: Write down your last recorded eye pressure, ask your doctor directly, “Have you checked my optic nerve and visual field for normal-tension glaucoma?”
Why normal-tension glaucoma is so easy to miss until it’s advanced
NTG is the introvert of eye diseases: quiet, polite, and very good at not drawing attention to itself.
Early on, you usually have:
- No pain.
- No redness.
- No obvious blur in the center of the vision.
The first changes often happen out in the edges of your visual field, where your brain is surprisingly good at filling in gaps. It’s like losing tiles at the edge of a mosaic; you don’t notice until whole sections are missing.
Risk factors that raise the odds after 60 include:
- Family history of glaucoma (any type).
- Thin corneas.
- Low blood pressure at night, especially in people on aggressive hypertension meds.
- Migraine, Raynaud’s phenomenon, or other “vascular” quirks.
- Sleep apnea, especially if poorly treated.
There’s another trap: a quick “pressure-only” screening at a pharmacy or big-box optical chain can look reassuring. If all they measure is intraocular pressure, NTG walks straight past the checkpoint.
Short Story: The “perfect” pressure that wasn’t (120–180 words)
Short Story: A 67-year-old retired teacher kept every health appointment like clockwork. Her optometrist told her for years, “Your pressure is perfect, 15 and 16. See you next year.” She noticed a little trouble finding lines on the right edge of the road at night but blamed “old headlights” and cataracts. One year, a new associate added an OCT scan and a visual field “because you’re over 65 now and on blood pressure pills.”
The OCT showed thinning on the top of her optic nerve; the visual field showed a subtle but definite defect. “You have glaucoma,” the doctor said, “but the normal-tension type.” Her first reaction was anger: “How long has this been there?” The honest answer was: probably years. Once she got on drops, adjusted her blood pressure meds at night, and started six-month visual fields, the defect stopped marching. “I wish we’d done those scans sooner,” she says. “But I’m glad we didn’t keep waiting for ‘high’ pressure.”
- Ask about your optic nerve photos and visual fields, not just pressure.
- Mention migraines, low blood pressure, and sleep apnea—they matter.
- If your exam is “too quick,” ask what was skipped.
Apply in 60 seconds: Jot down any “weird vision moments” from the last month—night driving, missing steps, bumping into door frames—and bring that list—or a printable symptom diary for seniors—to your next eye appointment.
Key tests that actually catch normal-tension glaucoma (and what they feel like)
To find NTG, your doctor has to look past the pressure number and assess the structure and function of your optic nerve.
The usual “NTG workup” after 60 includes:
- Comprehensive dilated eye exam – your pupils are dilated, and the doctor looks directly at the optic nerve for thinning or notches using special lenses.
- Intraocular pressure measurement – often the “blue light” test at the slit lamp. In NTG, this is usually 10–21 mmHg, but any spikes matter.
- Optical coherence tomography (OCT) – a painless scan that creates cross-sections of the retinal nerve fiber layer. The machine compares you to an age-matched database and flags thin areas.
- Visual field test (standard automated perimetry, CPT 92083) – you press a button when you see tiny lights in a bowl. This maps the “where” of your blind spots.
- Pachymetry – a quick cornea thickness measurement; thinner corneas can make pressures look lower than they truly are.
- Angle exam (gonioscopy) – a contact lens test to confirm your drainage angle is open.
The tests are painless but, honestly, a little annoying. The visual field in particular feels like a video game you can’t win. The goal is not perfection; it’s consistency over time, so your doctor can see whether the disease is stable or progressing. If checkups blur together, an annual eye exam checklist for seniors can help you track which tests you’ve actually had.
Show me the nerdy details
OCT devices track thickness in the retinal nerve fiber layer and ganglion cell complex, structures that are often affected early in NTG. Serial OCT scans let your doctor calculate a rate of change in microns per year; even a small but consistent decline can signal that your target pressure is not low enough.
Visual field tests often use a 24-2 or 10-2 pattern. In NTG, defects can cluster closer to fixation and be deeper than in typical high-pressure glaucoma. That’s why your doctor may add a 10-2 test focused on the central field if the 24-2 shows suspicious changes near the center.
- Expect at least OCT + visual field alongside pressure checks.
- Once diagnosed, these tests are repeated every 6–12 months.
- “Stable” means the scans and fields agree, not just the pressure.
Apply in 60 seconds: Look at your last visit summary or portal: can you see OCT and visual field results listed? If not, ask your clinic when those will be done.
How Medicare Part B sees glaucoma and normal-tension glaucoma in 2025
Now the money question: how does Medicare treat all of this?
Under Original Medicare in 2025:
- Part B deductible: $257 for the year. After you meet this, Part B usually pays 80% of the Medicare-approved amount for covered services, and you pay 20%.
- Glaucoma screening benefit: once every 12 months if you’re “high risk” (diabetes, family history, African American 50+, Hispanic 65+). This covers a pressure check and optic nerve evaluation as a preventive service.
- Diagnostic glaucoma care (including NTG): office visits, OCT, visual fields, and other tests are covered when medically necessary—not just under the screening benefit, but as ongoing care for a known disease or strong suspicion.
If you also receive retina treatments—such as anti-VEGF injections for age-related macular degeneration (AMD)—you’ll notice that the same Part B deductible and 80/20 cost-sharing rules usually apply.
The key distinction:
- Screening exam – used when your doctor is checking for glaucoma because you have risk factors but no diagnosis yet.
- Diagnostic/monitoring exam – used once glaucoma or NTG is suspected or confirmed; codes and coverage are different, but Part B still uses the 80/20 rule after the deductible.
In practical terms, a typical NTG visit for a Medicare patient over 60 might include: a comprehensive exam, pressure measurement, OCT, and visual field testing. After you’ve met your Part B deductible for the year, you’re usually responsible for about 20% of the Medicare-approved total, and any Medigap plan you have may cover some or all of that 20%.
US-specific note: Everything in this section assumes you’re in the United States and enrolled in Medicare. If you split time between countries or rely on a different national health system, you’ll want to check how your local system handles glaucoma testing and then treat the cost sections here as a framework, not a quote.
The same rules apply when Medicare Part B helps with surgeries like cataract removal; we walk through that step-by-step in our guide to cataract surgery and Medicare Part B.
- Once you’re diagnosed, visits and tests are “medically necessary,” not just screening.
- Part B pays 80% after the deductible; you owe 20% unless a Medigap or Advantage plan picks it up.
- Advantage plans may add their own copays or vision extras—check the specifics.
Apply in 60 seconds: Check your latest Medicare Summary Notice or plan portal for what you paid for your last eye visit, and note the “Part B deductible” and “coinsurance” lines.
Medicare eligibility checklist: screening vs full normal-tension glaucoma workup
If you’re over 60 and trying to figure out whether Medicare will help with the bill, start by asking: “Am I being seen for a screening or known/suspected disease?”
Money Block #1 – Eligibility checklist (Original Medicare, 2025, US)
Step 1 – Are you “high risk” for the annual glaucoma screening benefit?
- You have diabetes (and are already at risk for diabetic retinopathy).
- You have a family history of glaucoma in a first-degree relative.
- You’re African American and 50 or older.
- You’re Hispanic and 65 or older.
If you said “yes” to any of these: you’re generally eligible for a yearly covered glaucoma screening under Part B. The screening still follows the deductible + 20% coinsurance rules, but it signals to Medicare that the visit is preventive and risk-based.
Step 2 – Do you already have a glaucoma or NTG diagnosis, or a strong suspicion?
- Your chart lists “glaucoma,” “normal-tension glaucoma,” or “glaucoma suspect.”
- You’ve had repeat visual fields or OCTs tracking known changes.
- Your doctor is adjusting drops or planning laser/surgery to control progression.
If you said “yes” here: your visits and tests are usually billed as diagnostic and monitoring care. The annual “screening” label matters less; Medicare expects regular follow-up as part of disease management.
Step 3 – Are you on a Medicare Advantage plan?
- If yes: copays and covered extras (like routine refractions or glasses) are plan-specific. You may see fixed copays for specialist visits and imaging.
- If no (Original Medicare + optional Medigap): you follow the standard Part B deductible + 20% coinsurance structure; Medigap may cover some or all of that 20%.
Neutral action line: Save this checklist and confirm with your eye clinic’s billing staff which bucket they’re using—screening or diagnostic—before your next visit.
Mapping your normal-tension glaucoma bill with Medicare (mini calculator inside)
Let’s turn codes and jargon into something you can actually budget for.
Typical components of a normal-tension glaucoma visit under Medicare might include:
- Comprehensive eye exam – often billed under codes like 92004 (new patient) or 92014 (established).
- Visual field test – CPT 92083.
- OCT of optic nerve – CPT 92133 or 92134.
National Medicare-allowed amounts change yearly and vary by region, but ballpark 2024–2025 figures often look something like this when billed globally (technical + professional combined):
Money Block #2 – Sample Medicare Part B fee table for a glaucoma workup, 2025 (US)
| Service | Approx. Medicare-approved amount | Your 20% share after deductible | Notes |
|---|---|---|---|
| Comprehensive eye exam (92014) | $90–$120 | $18–$24 | Varies by region and complexity. |
| Visual field test (92083) | ~$55–$70 | ~$11–$14 | Higher if billed separately by test center. |
| OCT optic nerve (92133) | ~$40–$60 | ~$8–$12 | Also varies by region and device. |
So a visit with exam + visual field + OCT might have a Medicare-approved total of, say, $190–$250. After your deductible is met, your 20% share might be roughly $40–$50, before any Medigap or Advantage plan adjustments.
Neutral action line: Save this table and confirm the current year’s numbers with your clinic or the Medicare Physician Fee Schedule before you budget.
Mini calculator – estimate your out-of-pocket cost for today’s NTG visit
60-second estimator: This rough calculator assumes Original Medicare Part B in 2025.
This is an educational tool, not a quote. Always confirm actual charges with your clinic and plan.
- Big numbers on the bill—like a cataract surgery bill—are usually before Medicare discounts.
- Your 20% share is based on the Medicare-approved amount, not the “list price.”
- Medigap can bring that 20% close to zero for many services.
Apply in 60 seconds: Pull out your last Medicare Summary Notice and circle the “Medicare-approved amount” and “you may be billed” lines for your eye visit.
Treatment options for normal-tension glaucoma after 60
Once NTG is diagnosed, the main goal is simple to say and hard to execute: protect the optic nerve so that your remaining vision lasts as long as you do.
Key tools your doctor may use:
- Pressure-lowering eye drops – even in NTG, lowering pressure by 20–30% from your personal baseline can slow progression. Many people start with once-daily prostaglandin analogs, then add beta-blockers, carbonic anhydrase inhibitors, or others if needed.
- SLT laser (selective laser trabeculoplasty) – a quick, usually painless laser procedure that can reduce pressure enough to delay or replace drops in some patients.
- MIGS (minimally invasive glaucoma surgery) – often combined with cataract surgery to improve drainage with tiny stents or other devices.
- Traditional filtering surgery – trabeculectomy or drainage implants if disease is advanced or fast-moving.
- Systemic tweaks – adjusting night-time blood pressure medications, treating sleep apnea, and avoiding extreme head-down positions that spike eye pressure.
Because NTG is so tied to blood flow and fragile nerves, many glaucoma specialists are extra cautious about very low blood pressure at night. It’s one reason they’ll sometimes ask your primary doctor to relax bedtime blood-pressure targets a little, especially if you wake light-headed.
Personal moment: one patient joked that his care team had started a “truce negotiation” between his heart and his eyes. Lowering blood pressure protected his heart, but lowering it too far at night was starving his optic nerve. The solution was more nuanced than “good” or “bad” numbers; it was about the whole system.
- Most people start with drops or SLT; surgery is the backup, not the opening move.
- Night-time blood pressure, sleep apnea, and posture can all influence progression.
- No single number decides your fate; trends over time do.
Apply in 60 seconds: Make a list of all meds you take at night and give it to both your glaucoma specialist and primary doctor; ask them to discuss your night-time blood pressure together.
Paying for treatment: Original Medicare + Medigap vs Medicare Advantage
Once you move beyond “just tests,” the money picture shifts. Now you’re looking at ongoing drops, potential laser or surgery, and frequent follow-up visits.
Money Block #3 – Decision card: Original Medicare + Medigap vs Medicare Advantage for NTG care (2025, US)
| When to lean toward… | Original Medicare + Medigap | Medicare Advantage (Part C) |
|---|---|---|
| You see multiple specialists often | Predictable low coinsurance; many Medigap plans cover most Part B 20% shares. | Copays per visit; may be cheaper if glaucoma care is infrequent but can add up with frequent testing. |
| You want maximum choice of glaucoma specialist | Any provider that accepts Medicare nationwide. | Network-based; top glaucoma surgeons may be out of network in some areas. |
| You care about routine vision extras | Usually need separate vision discount or pay out of pocket for glasses/refraction. | Many plans offer routine eye exams and glasses allowances. |
| You’re on costly brand-name drops | Part D plan choice is critical; check your glaucoma meds on each formulary. | Drug copays and prior authorization rules vary; some plans push generics strongly. |
Neutral action line: Before you switch plans, ask your glaucoma clinic which local Advantage plans they see most often for NTG patients, and where prior authorizations cause delays.
Money Block #4 – Quote-prep list before comparing plans
- List every glaucoma drop you use (brand + generic name, strength, how often).
- Ask your doctor whether laser or surgery is likely in the next 2–3 years.
- Collect your last 2 years of glaucoma-related visit and test dates.
- Note whether you travel often or split time between states—this affects networks.
When you talk to a plan counselor or use an online plan finder, plug in these specifics, not just “glaucoma.” It can easily change your yearly out-of-pocket estimate by several hundred dollars.
- Check your actual drops and likely tests against each plan’s rules.
- Networks, prior authorizations, and drug tiers all matter.
- Changing plans every year can disrupt a carefully tuned treatment routine.
Apply in 60 seconds: Write down your current glaucoma drops and how many eye visits you had last year; keep that list next to your computer when you review Medicare plan options.
Living with normal-tension glaucoma after 60: daily systems, not daily panic
Normal-tension glaucoma is a marathon, not a sprint. Your goal is to build small systems that make protection automatic, so you don’t have to think about your eyes 24/7.
Helpful daily/weekly systems include:
- Drop rituals: tie drops to something you never skip—brushing teeth, evening TV, or your bedtime pillbox. Missing one dose occasionally isn’t a disaster; missing a week quietly matters.
- Appointment ladder: keep future OCT and visual field dates listed in large print on the fridge or in your phone calendar with reminders 1 week and 1 day ahead.
- Night-time routine: avoid long head-down positions (deep yoga inversions, reading in bed with your head bent sharply), especially if your disease is advanced.
- Driving honesty check: if your visual field has central or near-central defects, ask your doctor directly, “Would you feel safe if I drove your family?” It’s a blunt but clarifying question.
And yes, humor helps. Many glaucoma patients quietly nickname their drops and celebrate “boring” visits where the doctor says, “No change—see you in six months.” In chronic disease, boring is the win.
- Automate drops and appointments so willpower isn’t the bottleneck.
- Ask direct questions about driving and independence.
- Share your plan with at least one trusted person.
Apply in 60 seconds: Choose one “anchor habit” (like brushing teeth) and decide that your glaucoma drop lives right next to that anchor starting tonight.
Infographic: your normal-tension glaucoma care map on Medicare
1. Risk & Symptoms
- Age 60+
- Family history
- Low night-time blood pressure
- Migraines / Raynaud’s / sleep apnea
2. Key Tests
- Dilated exam & nerve photos
- Pressure check (often “normal”)
- OCT nerve scan
- Visual field map
3. Diagnosis & Plan
- NTG vs glaucoma suspect
- Target pressure set
- Follow-up interval chosen
- Night-time BP & sleep reviewed
4. Medicare Coverage
- Part B deductible ($257 in 2025)
- 80% of approved amount for exams/tests
- 20% coinsurance (often reduced by Medigap)
- Advantage plans: copays & networks vary
5. Long-Term Protection
- Drop/laser/surgery as needed
- Regular OCT & field tests
- Plan review each open enrollment
- Daily habits to keep vision usable
FAQ
1. Is normal-tension glaucoma really as dangerous as high-pressure glaucoma?
Yes. It can be just as serious over time. The difference is that the “enemy” is quieter. The risk of significant vision loss over 10–20 years depends on how early it’s caught, how aggressively it’s treated, and how well other risk factors—like blood pressure and sleep apnea—are managed. For more context on how glaucoma fits into the broader picture of age-related eye diseases after 60, it can help to see where NTG sits alongside cataracts and macular degeneration. Your 60-second action: ask your doctor what your current risk of meaningful vision loss is over the next decade and what they’re doing to lower that risk.
2. How often should I have OCT and visual field tests if I have NTG after 60?
Many specialists aim for OCT and visual field testing at least once a year in stable NTG, and more often (every 3–6 months) if the disease is moderate to severe or changing quickly. The exact interval depends on how fast your scans and fields are changing. Your 60-second action: look at your last several visit summaries and count how many OCTs and fields you’ve had in the past 24 months; if it’s fewer than your doctor initially planned, ask why and whether you’re still on track.
3. What does Medicare usually pay for in an NTG visit, and what do I pay?
For Original Medicare Part B in 2025, once you’ve met the $257 deductible, Medicare generally pays 80% of the approved amount for medically necessary eye exams and tests, and you pay the remaining 20%, which may be picked up by a Medigap plan. Advantage plans replace that structure with plan-specific copays. Your 60-second action: grab your most recent eye-care Explanation of Benefits or Medicare Summary Notice and highlight the lines that show “Medicare-approved amount” and “you may be billed.”
4. Do Medicare Advantage vision extras help with normal-tension glaucoma?
Vision extras—like free routine exams or glasses allowances—are nice but separate from glaucoma care. The NTG-relevant part is how the plan treats specialist visits, imaging, and glaucoma procedures. Some plans have low copays but tighter networks or prior-authorization rules for lasers and surgery. Your 60-second action: call your plan or log in online and check the copay for a specialist visit, visual field test, and OCT, using those exact terms.
5. Can I appeal if Medicare or my plan denies a glaucoma test or treatment?
Often, yes. Sometimes denials happen because a code was missing or the reason wasn’t explained clearly enough. Your doctor can submit supporting notes that show the test or treatment is medically necessary for NTG. Your 60-second action: if you receive a denial letter, circle the reason given and schedule a quick call with your eye clinic’s billing staff to ask what they recommend as the first step in an appeal.
6. What lifestyle changes actually matter for NTG, beyond taking drops?
Evidence points toward controlling sleep apnea, avoiding smoking, staying physically active, and protecting overall vascular health as meaningful levers. For some people, adjusting aggressive night-time blood pressure targets matters too. Your 60-second action: write down whether you snore, wake unrefreshed, or have been told your blood pressure runs “very low” at night; bring that note to your next glaucoma visit and ask whether further testing or coordination with your primary doctor makes sense.
7. I’m scared of losing my driver’s license. How early will my doctor tell me if it’s not safe to drive?
Good glaucoma specialists usually bring this up long before catastrophe—especially if defects encroach on the central field or your local laws require reporting. The key is honest two-way communication. Your 60-second action: at your next visit, ask directly, “Based on my current visual field, would you be concerned about my driving?” and request a simple explanation of how they’ll monitor this over time.
Conclusion: a 15-minute next step that protects future you
Normal-tension glaucoma after 60 is the definition of “silent but serious.” It doesn’t announce itself with pain, and it often hides behind a reassuring pressure number. But with the right tests, steady treatment, and a realistic understanding of Medicare, you can turn it from a looming threat into a managed part of your life.
In the next 15 minutes, you can:
- Write down your last known eye pressures, any OCT/visual field dates you remember, and all current drops.
- Run the mini calculator above with a realistic total from your last visit.
- Open your Medicare Summary Notice or plan portal and check how much of the Part B deductible you’ve met this year.
Then, at your next eye appointment, bring this article’s core questions:
- “Do my scans and fields look stable, or are they changing?”
- “Is my current treatment strong enough for normal-tension glaucoma?”
- “Given my Medicare setup, what should I expect to pay for tests or surgery if we need to escalate?”
Your optic nerve cannot speak, but your future self can. They will not care whether today’s paperwork was annoying. They will care that you still recognize your grandchildren’s faces, read the fine print, and cook without fear of missing the stove edge.
Last reviewed: 2025-12; sources included current Medicare rules and major glaucoma organizations in the United States.