


Senior eye health guide
Questions Seniors Should Ask
About Near Vision Problems
Near vision blur can feel small at first. A prescription label looks softer. A church bulletin becomes oddly stubborn. The crossword that used to sit comfortably at breakfast now needs brighter light, longer arms, and a small negotiation with patience.
For many older adults, the answer is ordinary aging, outdated reading glasses, dry eye, or cataracts. But not every reading problem belongs in the “just getting older” drawer. Sudden blur, distortion, flashes, floaters, pain, one-eye changes, and vision that worsens quickly deserve a faster conversation with an eye professional.
This guide turns near vision problems into practical questions seniors and caregivers can actually bring to an appointment. No panic, no medical fog machine, no buying stronger readers every month and hoping the tiny print becomes polite again.
Spot red flags
Know which symptoms should move faster than your calendar.
Ask better questions
Bring clearer details to the exam so the visit is easier to diagnose.
Avoid the glasses trap
Learn when readers help and when they may hide a bigger issue.
One calm rule: if near vision changes suddenly, painfully, or in one eye, treat it as a medical clue, not a shopping problem. 👓
Quick snapshot
This article is for older adults, caregivers, and adult children who want to understand reading blur, outdated glasses, dry eye, cataracts, medication effects, diabetes-related eye changes, and eye exam timing. By the end, you will know what to track, what to ask, when to seek urgent help, and how to prepare for a more productive eye appointment.
Table of Contents
Safety First: When Near Vision Changes Need Medical Attention
This guide is for education only. It cannot diagnose, treat, or replace advice from an optometrist, ophthalmologist, primary care clinician, pharmacist, or emergency professional.
Near vision problems can come from simple causes, but they can also be linked to eye disease, medication side effects, diabetes, blood pressure changes, stroke symptoms, or injury. Seniors should contact an eye doctor or urgent medical service if vision changes are sudden, painful, one-sided, rapidly worsening, or linked with headache, weakness, confusion, flashes, floaters, a curtain-like shadow, new double vision, severe redness, nausea, or loss of part of the visual field.
Key takeaway:
If near vision changes suddenly or comes with pain, distortion, flashes, floaters, weakness, confusion, or a dark shadow in the vision, do not treat it as a reading-glasses problem. Get medical guidance promptly.
Why this topic has real risk
Reading blur sounds harmless because it often starts with small annoyances: a medicine label, a phone screen, a receipt, a menu in a dim restaurant. But the eyes do not live in a separate little kingdom above the nose. They are connected to blood sugar, blood pressure, medication lists, inflammation, nerves, circulation, and the aging process itself.
That is why the best first question is not “What strength readers should I buy?” It is “What changed, when did it change, and does anything else feel wrong?” The timeline matters. The eye involved matters. The symptoms around the blur matter.
A senior who slowly needs more light for reading over several years may be dealing with normal aging or cataracts. A senior who wakes up with new distortion in one eye needs a different level of attention. Same word, “blur,” very different story.
A caregiver note before the glasses aisle
Caregivers often notice near vision changes before the person mentions them. Bills sit unopened. Pill bottles are turned toward the light. The phone is held farther away. The TV remote becomes a tiny plastic riddle.
Try not to lead with “You need an eye exam,” even when that is probably true. Start with a concrete observation: “I noticed the prescription label was hard to read today. Did that start recently?” This keeps the conversation practical rather than accusatory.
For broader home-safety context, you may also find this related guide useful: home safety checklist for seniors with vision challenges. Near vision trouble is not only about books. It touches medication, cooking, mobility, mail, screens, and confidence.
“Is This Just Aging?” The First Question Seniors Should Not Skip
Many seniors first notice near vision problems when reading small print becomes a little theatrical. The book moves farther away. The lamp gets dragged closer. Someone mutters that restaurant menus were clearly printed by ants with legal training.
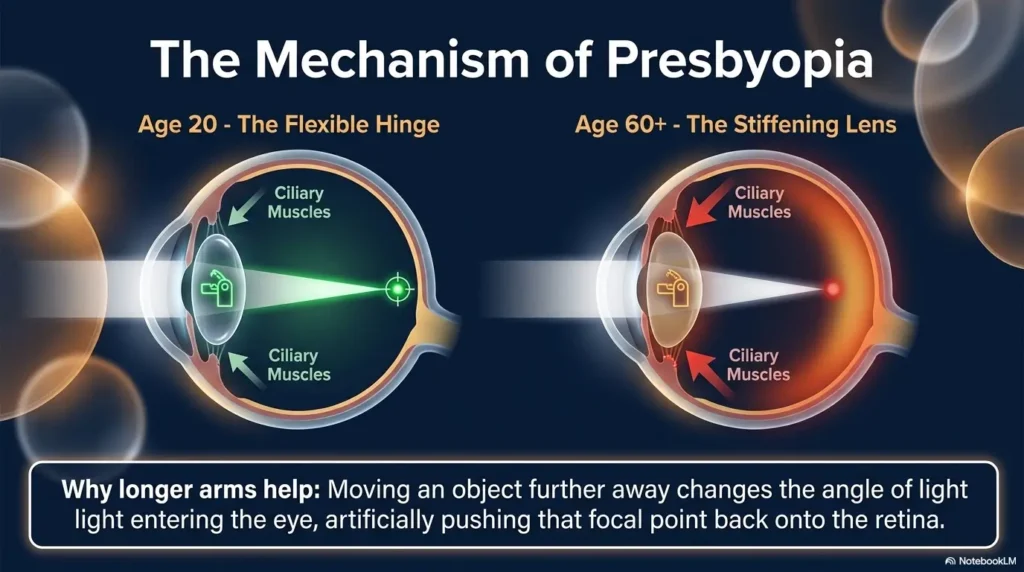
Some of this can be normal. Presbyopia, the age-related loss of the eye’s ability to focus up close, commonly makes reading harder over time. But “common” is not the same as “safe to ignore forever.” A slow change and a sudden change belong in different folders.
Presbyopia can be normal, but not every blur is harmless
Presbyopia usually develops gradually. People often notice they need to hold reading material farther away or use more light. Drugstore readers may help for simple close tasks, especially when both eyes feel similarly blurry and there are no other symptoms.
But seniors should be careful with the phrase “just aging.” It can become a velvet curtain that hides things worth checking, including cataracts, dry eye, glaucoma, retinal disease, medication effects, and diabetes-related eye changes.
A helpful question is: “Is this problem mainly focus, clarity, distortion, light sensitivity, or missing information?” Trouble focusing is not the same as seeing wavy lines. Needing brighter light is not the same as seeing a gray spot in the center of words.
Ask: “Did this change happen slowly or suddenly?”
A slow change over months or years often points toward aging focus changes, cataracts, or gradually changing glasses needs. It still deserves an exam, but it usually gives you more breathing room than sudden vision loss.
A sudden change is different. Sudden blur, sudden distortion, a new blind spot, sudden floaters, or a shadow can point to problems that need urgent evaluation. That does not mean the worst is happening, but it does mean the “let’s wait three months” plan is wearing clown shoes.
Quick timeline check:
- Years: often aging focus, cataracts, or prescription change.
- Months: still needs an exam, especially if worsening.
- Days: call an eye doctor promptly.
- Hours or overnight: treat as urgent, especially with other symptoms.
Ask: “Is near vision blurry in one eye or both?”
One-eye symptoms are easy to miss because the better eye quietly covers for the weaker one. Seniors may not notice a problem until they rub one eye, cover the other, or try to read in bed with one eye partly blocked by a pillow.
Try a simple check: cover the right eye and read a sentence. Then cover the left eye and read the same sentence. Do not press on the eye. Do not perform this while walking or driving. The goal is only to notice whether one eye seems dramatically worse, distorted, darker, or patchy.
If one eye has new blur, distortion, missing letters, flashes, floaters, or a curtain-like shadow, contact an eye professional promptly. If there are stroke-like symptoms, call emergency services.
The tiny clue: reading glasses help, but only sometimes
Reading glasses can be useful. They are not morally suspicious. A good pair can make menus, labels, and phone screens feel civilized again.
Still, readers mostly help with focusing. They do not fix cataracts, retinal swelling, macular degeneration, eye pressure problems, medication side effects, or neurological symptoms. If stronger readers are needed again and again, or if they help one task but not another, the next step should be an eye exam rather than another spin through the drugstore rack.
For a practical comparison, see reading glasses vs magnifiers. The right tool depends on whether the issue is focus, print size, contrast, tremor, lighting, or an underlying eye condition.
Sudden Near Blur: The Red-Flag Timeline Question
When a senior says, “I suddenly can’t read this,” the next question is not about font size. It is about time.
Time helps sort everyday blur from urgent blur. Eye doctors listen closely when someone can say, “It started yesterday morning,” or “It happened after I fell,” or “It was fine at breakfast and strange by lunch.” Those details are diagnostic breadcrumbs.
Ask: “When did I first notice the change?”
Write down the first moment the change was noticed. Was it while reading a pill bottle? Looking at a phone? Signing a check? Reading subtitles? The task can matter because different distances use different parts of the visual system.
Also note whether the blur stayed the same, came and went, or got worse. A blur that clears after blinking has a different flavor from blur that persists no matter what you do.
Caregivers can help by avoiding vague phrases like “for a while.” Try to turn “a while” into “about two weeks,” “since the new medication,” or “after the cataract surgery follow-up.” Doctors do not need poetry here. They need a clock and a map.
Ask: “Did it appear overnight, after a fall, or after surgery?”
Near vision changes after a fall, head injury, eye injury, surgery, injection, or new medication should be taken seriously. Even if the blur seems mild, the context matters.
After cataract surgery, for example, vision may fluctuate during healing, but new severe pain, sudden vision drop, increasing redness, flashes, floaters, or a shadow should be reported quickly. After a fall, vision changes may be related to eye injury, bleeding, neurological problems, or medication effects.
Seniors should not drive themselves if vision is suddenly impaired. Ask a family member, neighbor, rideshare, or emergency service for transportation. A stubborn streak is charming in garden tomatoes, less charming behind the wheel with sudden blur.
Ask: “Do I also see flashes, floaters, shadows, or distortion?”
New flashes, a sudden increase in floaters, a dark curtain, missing side vision, or a shadow can suggest a retinal problem that needs urgent evaluation. Wavy lines, bent letters, or a gray central spot may point toward macular problems.
The important part is not to decide at home which diagnosis fits. The important part is to notice the symptom and act. A senior does not need to know the Latin name of the dragon before leaving the castle.
Key takeaway:
For sudden near vision problems, ask three questions immediately: When did it start? Is one eye worse? Are there flashes, floaters, shadows, pain, distortion, or neurological symptoms?
Do not wait-and-see if vision drops quickly
A fast drop in vision should not be monitored casually at home. Waiting may cost time that matters. Even when the final cause turns out to be less serious, the safer decision is to get guidance quickly.
Call the eye doctor’s office and describe the exact symptoms. Use plain language: “My left eye became blurry overnight,” “Straight lines look wavy,” “I see a dark shadow,” or “I suddenly have many new floaters.” These phrases help staff triage the call.
The Reading Glasses Trap: When Stronger Lenses Are Not the Answer
Drugstore reading glasses are wonderfully convenient. They are also a little too easy. When near vision gets blurrier, the obvious move is to buy a stronger pair. Sometimes that works. Sometimes it turns the real problem into a better-dressed problem.
Stronger readers magnify and shift focus. They do not check eye pressure, examine the retina, test for cataracts, evaluate dry eye, or review medication side effects. That is why repeated reader upgrades can become a trap.
Ask: “Am I increasing magnification every few months?”
If a senior keeps moving from +1.50 to +2.00 to +2.50 to +3.00 in a short period, it is time to pause. That pattern may mean the eye’s needs are changing, but it may also mean the person is compensating for blur, poor lighting, cataracts, dry eye, or retinal issues.
More power also narrows the comfortable working distance. Very strong readers may require holding material close to the face. That can be frustrating for someone with tremor, neck pain, arthritis, or limited lighting.
A better question is: “What exact task am I trying to improve?” Reading a paperback, reading a computer screen, checking a prescription label, threading a needle, and reading a glossy bill are not the same visual job.
Ask: “Do cheap readers help one task but worsen another?”
Over-the-counter readers usually have the same lens power in both eyes. That can be fine for simple presbyopia, but many older adults have astigmatism, different prescriptions between eyes, cataract changes, or post-surgery differences.
If readers help with a cereal box but make the computer feel swimmy, the issue may be distance-specific. Computer work often needs a weaker or customized prescription compared with close reading.
If you suspect astigmatism is part of the problem, this related guide on reading glasses for astigmatism may help explain why generic readers can feel almost right but still tiring.
| Situation | Readers may help if… | Get an exam if… |
|---|---|---|
| Small print is hard | The change is gradual and both eyes seem similar. | Print is distorted, missing, gray, or suddenly worse. |
| Computer blur | A weaker intermediate pair improves comfort. | Blur comes with headaches, double vision, or one-eye changes. |
| Label reading | Lighting and magnification solve the task safely. | Medication mistakes are happening or labels remain unreadable. |
| Frequent upgrades | A one-time change improves stable symptoms. | A stronger pair is needed every few months. |
Magnification can hide the real issue
Magnification can make letters bigger while the underlying image remains poor. If cataracts scatter light, dry eye breaks up the tear film, or retinal disease affects central vision, larger letters may still look faded, warped, or incomplete.
This is why seniors should describe the quality of the blur. Is it fuzzy? Dim? Wavy? Washed out? Fluctuating? Shadowy? Does blinking help? Does brighter light help? Does one eye behave differently?
Those words are more useful than “I need stronger glasses.” They help the eye doctor decide what to test and how urgently to evaluate the change.
Why prescription updates need an eye health check
A refraction tells what lens power helps focus light. A comprehensive eye exam looks at eye health. Seniors often need both, especially when symptoms have changed.
A prescription update without an eye health check can miss reasons vision is changing. A senior may walk away with new glasses but still have glare, distortion, pressure issues, retinal changes, or uncontrolled dry eye.
Ask directly: “Will this visit include an eye health exam, and do I need dilation?” It is a simple question with enormous practical value.
Cataract Clues Seniors Often Mistake for Bad Lighting
Cataracts do not always announce themselves with drama. They often arrive like dust on a window, slowly changing the way light enters the eye. Seniors may first blame the lamp, the print, the weather, the restaurant, or the person who designed gray text on a gray background, a design crime with many victims.
Cataracts can make reading harder, especially in dim light or glare. They can also affect night driving, color brightness, contrast, and the crispness of print.
Ask: “Do I need brighter light than I used to?”
Needing more light can be part of normal aging, but it is also a common cataract clue. A senior may do fine outdoors but struggle in a dim kitchen, church pew, hallway, or restaurant booth.
The key is change. If the same lamp, same chair, and same book suddenly feel inadequate, write that down. If brighter light helps but causes glare, that is also useful information.
Good lighting should be bright, even, and positioned to avoid glare. A lamp shining directly into the eyes can make cataract scatter worse. Side lighting often works better than a harsh beam bouncing off glossy paper.
Ask: “Are glare, halos, or night driving problems getting worse?”
Cataracts can cause glare, halos around lights, and trouble with headlights at night. Some seniors first notice this while driving, but others notice it while reading glossy mail, looking at a bright screen, or sitting near a sunny window.
Night driving symptoms deserve special care. If glare makes lane lines, signs, pedestrians, or other vehicles harder to see, driving habits may need to change before surgery is even discussed. Safety does not have to wait for the final treatment plan.
Ask the eye doctor: “Are cataracts contributing to my reading and glare problems, and how advanced are they?” This invites a practical answer instead of a vague “You have cataracts,” which many older adults hear years before surgery is needed.
Ask: “Is print faded, yellowed, or less crisp?”
Cataracts can change contrast and color perception. White paper may look dull. Black letters may seem less black. Colors may look warmer or less vivid. Reading may feel possible but tiring.
Seniors often describe this as “the print is not sharp,” even when the font size is large enough. That distinction matters. If large print is still faded or low contrast, the problem may not be solved by size alone.
For home adjustments, increase contrast before increasing clutter. Use dark pens on white paper, matte surfaces instead of glossy ones, and task lighting that does not bounce into the eyes.
Cataract clue checklist
- Reading needs brighter light than before.
- Glare feels harsher, especially from windows, lamps, or headlights.
- Print looks faded, yellowed, or low contrast.
- Night driving feels less safe.
- New glasses help only partly.
- One eye seems cloudier than the other.
The lamp is not always the villain
Better lighting can help, but if a senior keeps buying brighter bulbs and still cannot read comfortably, the lamp has probably been over-interrogated. The eye needs a turn on the witness stand.
A comprehensive exam can clarify whether cataracts are part of the problem and whether glasses, lighting changes, monitoring, or surgery discussion makes sense. Cataract decisions should be based on daily function, safety, exam findings, and the senior’s goals, not only on the word “cataract.”
Dry Eye Blur: The Problem That Comes and Goes
Dry eye can create a maddening kind of near blur because it often changes during the day. One minute print is clear. The next minute it looks smeared. Blink a few times and it improves. Then the blur returns like a tiny, rude weather system.
Dry eye becomes more common with age and may be affected by medications, screen use, indoor heating, air conditioning, wind, eyelid conditions, autoimmune disease, and previous eye surgery. It can make reading, phone use, crafts, and computer tasks more tiring.
Ask: “Does my vision clear after blinking?”
If vision clears after blinking, resting the eyes, or using lubricating drops recommended by a clinician, dry eye may be involved. The tear film is the eye’s first focusing surface. When it is unstable, the image can break up.
Seniors can track this for a few days. Does blur worsen after reading for ten minutes? Does it improve after closing the eyes briefly? Does it happen more in the afternoon? Does it flare in certain rooms?
This kind of pattern helps the eye doctor separate dry eye blur from constant blur, distortion, or lens changes.
Ask: “Do screens, heating, air conditioning, or wind make it worse?”
People blink less when reading screens. Indoor air can also dry the eyes. A senior who reads comfortably in the morning may struggle after several hours of phone use, television subtitles, email, or online bills.
Small environmental changes may help: move chairs away from vents, reduce direct fan airflow, take blink breaks, enlarge screen text, and use better contrast. These steps do not replace medical care, but they can reduce daily irritation.
If screen-related blur is a major issue, this related guide on digital eye strain in seniors may help with practical screen adjustments.
Ask: “Are my eyes burning, gritty, watery, or tired?”
Dry eye does not always feel dry. It may feel gritty, burning, tired, sandy, sticky, or watery. Watery eyes can happen when irritation triggers reflex tearing, but those tears may not provide stable lubrication.
That is why “my eyes water, so they cannot be dry” is one of the great eye-health plot twists. The eye can be watery and dry in the functional sense, which sounds unfair because it is.
Seniors should ask before using redness-relief drops, old prescription drops, or someone else’s eye drops. Some products can worsen dryness or mask symptoms. A clinician or pharmacist can help choose safer options.
Key takeaway:
Blur that comes and goes, improves after blinking, or worsens with screens and airflow may involve dry eye. Mention the pattern, not just the blur.
Short Story: The menu that solved the mystery
Marian, 74, thought she needed stronger readers because restaurant menus had become impossible. At home, her books were mostly fine. At restaurants, the letters blurred, lights glared, and her eyes watered. She blamed the menus, then the lighting, then herself.
Her daughter asked one simple question: “Does it clear when you blink?” Marian tried it. It did, for a few seconds. Then the words smeared again.
At the eye appointment, she brought that exact detail. The doctor found dry eye and early cataracts. The plan was not just stronger glasses. It included dry eye care, lighting changes, and monitoring the cataracts.
The lesson was small but mighty: the way blur behaves can matter as much as the blur itself.
Medication Side Effects: The Quiet Vision Saboteur
Many older adults take several medications, and some can affect vision directly or indirectly. Allergy pills, sleep aids, antidepressants, blood pressure medicines, bladder medicines, pain medicines, steroids, and other drugs may contribute to dryness, focusing trouble, dizziness, light sensitivity, or pressure-related concerns in certain people.
This does not mean seniors should stop medications. It means the medication list belongs in the eye conversation. Bring the bottles, the printed list, or clear photos of labels. The medication cabinet is often the missing chapter.
Ask: “Did the blur start after a new medication?”
Timing matters. A new medication, dose increase, over-the-counter sleep aid, allergy pill, or supplement may line up with new blur or dryness. Seniors often forget to mention non-prescription products because they do not think of them as “real medicine.” The eyes may disagree.
Write down the start date of any new medication and the start date of the vision symptom. Even if the timing turns out to be unrelated, it gives the clinician a cleaner puzzle.
For a deeper companion topic, read this guide on polypharmacy and vision problems. Multiple medications can create overlapping side effects that are hard to spot one bottle at a time.
Ask: “Could allergy pills, sleep aids, blood pressure drugs, or antidepressants be involved?”
Some medications may reduce tear production. Others can affect focusing, cause dizziness, or change how comfortable the eyes feel during reading. Some drugs can be risky for people with narrow angles or certain eye conditions.
The right question is not “Is this medication bad?” The better question is “Could this medication be affecting my vision, dryness, or eye pressure risk?” That gives the doctor room to answer carefully.
A pharmacist can also be a useful ally. Pharmacists can identify common vision-related side effects, interaction concerns, and safer ways to organize medication information for medical visits.
Medication vision-prep list
- Bring a current medication list with dose and timing.
- Include over-the-counter sleep aids, allergy medicines, pain relievers, and supplements.
- Note any recent medication start, stop, or dose change.
- Write down when the vision symptom began.
- Ask whether any medication could worsen dry eye, blur, dizziness, or eye pressure risk.
- Do not stop prescribed medicine without the prescriber’s guidance.
Ask: “Should I bring my full medication list to the eye exam?”
Yes. Bring it even if the eye office does not ask with great enthusiasm. A complete list helps connect dots between dry eye, blurry near vision, dizziness, blood pressure, diabetes, allergy symptoms, and glaucoma risk.
If the senior has trouble reading labels, use a phone camera to take clear photos of each bottle. Include the front label and instructions. Better yet, ask the pharmacy for a large-print medication list.
Medication safety and near vision overlap in everyday life. If labels are becoming hard to read, consider this related guide on large-print prescription labels.
Do not stop medications on your own
Stopping medication abruptly can be dangerous. Blood pressure, heart rhythm, mood, sleep, pain, inflammation, diabetes, and other conditions may worsen if medicines are changed without guidance.
If a medication may be contributing to vision symptoms, the clinician may adjust timing, change the medication, treat the side effect, or monitor the eye more closely. The goal is coordinated care, not a kitchen-table medication rebellion.
Diabetes, Blood Pressure, and Near Vision: The Body-Wide Question
Near vision does not always begin in the eyes. Diabetes and blood pressure can affect the retina, blood vessels, fluid balance, and clarity of vision. Blood sugar swings can even make vision temporarily blurry by affecting the lens inside the eye.
For seniors with diabetes, prediabetes, high blood pressure, high cholesterol, kidney disease, or vascular disease, reading blur deserves special attention. It may still be a glasses issue. But it should not be assumed.
Ask: “Have my blood sugar levels changed recently?”
Blood sugar changes can cause blurry vision. A senior may notice fluctuating focus during periods of high glucose, medication changes, illness, steroid use, diet changes, or new diabetes treatment.
If vision blur changes along with glucose readings, bring that pattern to both the eye doctor and the primary care clinician. Do not order new glasses during a period of unstable blood sugar without asking the clinician whether timing matters.
A glasses prescription measured during unstable blood sugar may not represent the eye’s usual focusing needs. That can lead to frustrating glasses that feel wrong after levels stabilize.
Ask: “When was my last dilated eye exam?”
A dilated eye exam lets the eye professional examine the back of the eye, including the retina and optic nerve. This is especially important for seniors with diabetes because eye disease can develop before obvious symptoms appear.
Some people assume they have had a full eye exam because they had a quick vision screening or bought new glasses. Those are not the same thing. Ask specifically: “Was I dilated?” and “Was my retina checked?”
Ask: “Could swelling, bleeding, or retinal changes affect reading vision?”
Diabetic eye disease can affect the retina, including the macula, the part used for sharp central vision. Central vision is what lets people read, recognize faces, see fine details, and look directly at objects.
If the macula is affected by swelling or other changes, reading may become blurry, distorted, patchy, or harder even with new glasses. Seniors should describe any wavy lines, missing letters, or gray spots clearly.
Blood pressure and cholesterol control also matter. Eye health is not only an eye chart. It is circulation, inflammation, metabolism, and daily habits braided together.
Show me the nerdy details
Near vision depends on several systems working together. The cornea and lens focus light. The tear film keeps the front surface smooth. The retina receives the image. The macula handles sharp central detail. The optic nerve sends information to the brain. A problem in any part can make reading harder.
That is why one word, “blur,” can have many meanings. Presbyopia is a focusing problem. Cataract is a cloudy lens problem. Dry eye is a tear-film problem. Diabetic macular edema is a retinal swelling problem. Double vision may involve eye alignment, nerves, muscles, or neurological concerns. The symptom feels simple, but the machinery is elegant and busy.
Why “just blurry print” may deserve a medical look
Blurry print can affect medication safety, cooking, bills, driving paperwork, medical instructions, phone messages, and fall prevention. For seniors with chronic conditions, near vision is part of self-care.
If a person cannot read glucose meter numbers, appointment texts, prescription labels, or after-visit instructions, the issue becomes more than inconvenience. It becomes a safety and independence problem.
That is why caregivers should treat reading difficulty as a practical health signal. The goal is not to hover. The goal is to remove tiny hazards before they grow teeth.
Distorted Words: The Question That Points Beyond Glasses
Distortion is different from ordinary blur. Blur makes things fuzzy. Distortion bends, warps, hides, or breaks them. Seniors should learn to describe this difference because it can point beyond glasses.
If straight lines look wavy, letters disappear, or the center of vision looks gray, blurry, or smudged, the macula may need evaluation. This is especially important if the change is new or in one eye.
Ask: “Do straight lines look wavy?”
Door frames, tile grout, window blinds, notebook lines, and refrigerator magnets can all serve as informal clues. If lines look bent in one eye, write it down and call the eye doctor promptly.
Do not diagnose from a home test. Use it as a reason to seek professional evaluation. A home observation is a smoke alarm, not the fire report.
For people already diagnosed with macular degeneration or central vision loss, distortion monitoring may be part of a doctor’s plan. Follow the plan given by the eye professional, and report changes quickly.
Ask: “Are letters missing, bent, or gray in the center?”
Missing letters are easy to mistake for dirty glasses, poor lighting, or tiredness. Seniors may say, “The word disappears when I look right at it,” or “The middle of the line looks smudged.” That deserves attention.
Central vision problems can make reading especially frustrating because the eye may see the page but not the exact letters being viewed. The person may move their eyes around the word, trying to catch it from the side.
If this sounds familiar, do not simply increase magnification. Ask for an exam that evaluates the retina and macula.
Near Vision Decision Flow
1. Timing
Sudden, overnight, or fast change moves first.
2. One eye?
Cover each eye gently and compare reading clarity.
3. Distortion
Wavy lines or missing letters need prompt attention.
4. Body clues
Check diabetes, blood pressure, surgery, falls, and medications.
5. Exam prep
Bring glasses, drops, medications, and symptom notes.
Ask: “Is one eye doing worse when I cover the other?”
The cover-one-eye check is simple and useful. Many seniors discover that the “reading problem” is mainly in one eye. That changes the urgency and the questions.
Use the same reading material, same lighting, and same distance. Cover one eye gently without pressing. Then switch. Notice clarity, brightness, distortion, missing spots, and comfort.
If one eye is newly worse, especially with distortion or missing vision, call promptly. The better eye may have been quietly carrying the load for weeks.
The refrigerator-magnet test: simple, not silly
Pick a straight vertical line at home: a door frame, cabinet edge, calendar grid, or refrigerator magnet border. Look at it with one eye at a time. If it appears wavy, broken, bowed, or missing in one eye, write that down and contact an eye professional.
This is not a replacement for an Amsler grid or medical test. It is a plain-language observation that helps a senior describe distortion. Sometimes the humble refrigerator, keeper of leftovers and family photos, becomes the first useful witness.
What to Ask at the Eye Appointment
A good eye appointment is easier when the senior arrives with better questions. The goal is not to sound medically impressive. The goal is to leave with clear next steps.
Bring all glasses, readers, magnifiers, eye drops, medication lists, and a symptom timeline. If a caregiver attends, agree beforehand who will speak about what. Nobody enjoys a family press conference in a small exam room.
Ask: “Do I need a comprehensive dilated eye exam?”
This is one of the most useful questions in the entire visit. Dilation helps the eye professional examine the retina, optic nerve, and blood vessels inside the eye. It may be especially important for seniors with diabetes, macular symptoms, glaucoma risk, sudden changes, or unexplained blur.
Ask whether dilation is being done today, whether it should be scheduled soon, and whether someone should drive afterward. Dilation can make vision blurry and light-sensitive for a while.
If transportation is hard, say so. Many clinics can help schedule at a time when a caregiver can attend or explain what to expect.
Ask: “Is this presbyopia, cataract, dry eye, retinal disease, or something else?”
This question asks the clinician to sort causes rather than simply update glasses. It also helps seniors understand whether more than one issue is contributing.
It is common for older adults to have overlapping causes. A senior may have presbyopia, early cataracts, dry eye, and mild macular changes. The plan may include readers, prescription glasses, dry eye treatment, monitoring, medical follow-up, or specialist referral.
Ask for the answer in practical terms: “What part of my reading problem can glasses fix, and what part cannot be fixed by glasses?” That single sentence can prevent weeks of confusion.
Appointment question list
- Do I need dilation today or soon?
- Is the problem mainly focus, cataract, dry eye, retina, medication, or another cause?
- What symptoms should make me call immediately?
- Do I need separate glasses for reading, computer use, and driving?
- Would a magnifier, better lighting, or contrast tool help?
- When should I come back?
- Should my primary care clinician review blood sugar, blood pressure, or medications?
Ask: “Do I need separate glasses for reading, computer use, or driving?”
Many seniors use one pair of glasses for too many jobs. Reading glasses may be too strong for computer distance. Distance glasses may not help with labels. Progressives may be convenient but frustrating for some people with balance issues, narrow reading zones, or specific hobbies.
Tell the eye doctor what tasks matter most: reading books, pill bottles, phone screens, recipes, sewing, woodworking, computer work, piano music, TV subtitles, driving, or church bulletins. A prescription is more useful when it serves real life rather than an abstract eye chart.
If the senior has tremor, arthritis, or trouble holding materials close, mention that too. The best visual solution is not only about lens power. It is about posture, hand stability, lighting, contrast, and safety.
Ask: “How often should I be checked from now on?”
Eye exam timing depends on age, symptoms, diagnosis, diabetes, glaucoma risk, macular findings, medications, surgery history, and overall health. Some seniors need routine monitoring. Others need prompt follow-up.
Before leaving, ask for a specific interval: “Should I return in one year, six months, three months, or sooner if symptoms change?” Also ask what symptoms should override the scheduled date.
Write the answer down before leaving the office. Memory after appointments can be slippery, especially when pupils are dilated and the world looks like it has been dipped in bright soup.
When to Seek Help or Stop Waiting
Some near vision problems can wait for a routine appointment. Others should not. The safest approach is to recognize symptoms that need faster action.
When in doubt, call the eye doctor, primary care clinician, nurse line, or emergency service and describe the symptoms clearly. Staff can help decide the next step. Do not drive yourself if vision is suddenly impaired.
Seek urgent care for sudden vision loss or a curtain-like shadow
Sudden vision loss, a dark curtain, a shadow moving across the vision, or missing side vision should be treated as urgent. These symptoms may point to serious eye or neurological problems.
Use direct language when calling: “I have sudden vision loss,” “I see a curtain,” or “Part of my vision is missing.” Do not soften the description to “a little weird” if the change is significant.
If symptoms come with weakness, facial droop, confusion, trouble speaking, severe headache, or trouble walking, call emergency services. Those may be stroke-like symptoms.
Call promptly for new flashes, floaters, or wavy central vision
New flashes, a sudden shower of floaters, or wavy central vision should be reported promptly. These symptoms may need a dilated retinal exam.
Some floaters are harmless and common with aging, but a sudden change is the key concern. A senior does not need to decide whether it is serious. That is the clinician’s job.
If the eye office is closed, follow the after-hours instructions or seek urgent care according to the symptom severity and local options.
Get checked for eye pain, redness, nausea, or halos
Eye pain with redness, nausea, vomiting, headache, halos around lights, or sudden blur can be urgent. Some eye pressure problems require quick treatment.
Do not try to solve painful red eye with old drops or borrowed drops. Call for medical guidance. Eye pain is not a good place for improvisation.
If the senior recently started a medication and then developed eye pain, halos, or sudden blur, mention that during the call. Medication timing can help triage risk.
Key takeaway:
Stop waiting and seek help faster for sudden vision loss, one-eye changes, curtain-like shadows, flashes, new floaters, wavy central vision, severe pain, red eye with nausea, or stroke-like symptoms.
Do not drive yourself if vision is suddenly impaired
Sudden impaired vision can make driving dangerous even if the senior feels calm. Peripheral vision, depth judgment, glare tolerance, and reaction time may be affected.
Ask someone else to drive, use a ride service, call a medical transport option, or call emergency services if symptoms are severe. The goal is to arrive safely and quickly, not heroically.
FAQ: Questions Seniors Ask About Near Vision Problems
Why can I read better when I hold things farther away?
This often happens with presbyopia, the age-related change that makes close focusing harder. Holding material farther away can bring it into a clearer focus range. If this is new, worsening quickly, or paired with distortion, pain, or one-eye symptoms, schedule an eye exam.
Are drugstore reading glasses safe for seniors?
They can be safe for simple, occasional near tasks if both eyes need similar help and there are no warning symptoms. They are not a substitute for an eye health exam, especially if vision has changed, one eye is worse, or stronger readers are needed repeatedly.
Why does my near vision change throughout the day?
Fluctuating near vision may be related to dry eye, screen use, fatigue, medication effects, blood sugar changes, or lighting. Track when it happens, what improves it, and whether blinking clears it. Bring those notes to the eye appointment.
Can cataracts make reading harder before distance vision gets bad?
Yes, cataracts can affect contrast, glare, and clarity in ways that make reading harder, especially in dim light or with glossy paper. Some people notice reading fatigue, faded print, or glare before they describe distance vision as truly poor.
Why do my eyes water when I read?
Watery eyes can happen with dry eye because irritation may trigger reflex tearing. Reading and screen use can reduce blinking, which worsens tear-film instability. Ask an eye professional before relying on redness-relief drops or old prescription drops.
Can diabetes cause blurry near vision?
Yes. Blood sugar changes can temporarily affect focusing, and diabetes can also cause retinal disease that affects vision. Seniors with diabetes should ask about dilated eye exams and report blur, distortion, floaters, or vision changes promptly.
Should I see an optometrist or ophthalmologist?
Both can provide eye care, and the right choice depends on symptoms, diagnosis, local access, and urgency. Optometrists commonly handle exams, glasses, dry eye, and detection of eye disease. Ophthalmologists are medical doctors who can manage complex disease and perform surgery. Sudden or severe symptoms should be triaged urgently.
How often should seniors get an eye exam?
Exam timing depends on age, symptoms, diabetes, glaucoma risk, macular disease, cataracts, medications, and past eye history. Ask your eye professional for a specific schedule and what symptoms should make you call sooner.
Your 15-Minute Next Step Before the Next Appointment
The best next step is not dramatic. It is a one-page symptom note. In 15 minutes, a senior or caregiver can gather the details that make an eye appointment more useful.
Write down when the near vision problem started, whether it affects one eye or both, what tasks are hardest, whether blinking or lighting helps, and whether there are red-flag symptoms. Add medications, eye drops, recent surgery, falls, diabetes status, and blood pressure concerns.
Then schedule a comprehensive eye exam if near vision has changed noticeably, especially if the change is new, worsening, or affecting medication safety. Bring all glasses, readers, magnifiers, eye drops, and medication lists. A clear little note can turn a vague visit into a focused conversation.
Key takeaway:
Within 15 minutes, create a symptom timeline, compare one eye at a time, gather medications and glasses, and book an eye exam if near vision has changed. Small preparation can save a surprising amount of confusion.
15-minute appointment prep card
- Minute 1 to 3: Write the first date or week the blur appeared.
- Minute 4 to 6: Cover each eye gently and note whether one eye is worse.
- Minute 7 to 9: List symptoms: blur, distortion, glare, dryness, pain, flashes, floaters, shadow, or double vision.
- Minute 10 to 12: Gather glasses, readers, magnifiers, eye drops, and medication list.
- Minute 13 to 15: Call or schedule the appointment, and ask whether dilation may be needed.
Near vision problems can make the world feel smaller: fewer books, fewer recipes, fewer labels read without help. But the right questions can reopen the room. Ask when it started. Ask whether one eye is worse. Ask whether lines are wavy. Ask whether medicines, diabetes, cataracts, dry eye, or retinal changes might be involved. Then let an eye professional look where readers cannot.
Last reviewed: 2026-06