


Beyond the Drugstore Rack: A Senior’s Guide to Clearer Vision with Astigmatism
The drugstore rack looks simple until it starts feeling like a tiny carnival of numbers. +1.50. +2.00. +2.75. One pair sharpens the soup label. Another makes the phone look better but the calendar swim. For seniors with astigmatism, choosing reading glasses is rarely just “go stronger.” The real issue is that ordinary readers magnify near work, while astigmatism can stretch, smear, or shadow letters because the eye needs cylinder and axis correction too.
Guessing can cost more than money. It can mean headaches, neck strain, misread pill bottles, awkward computer posture, and delayed care for cataracts, glaucoma, diabetic eye disease, or macular degeneration. This guide helps you compare over-the-counter readers, prescription reading glasses, bifocals, progressives, and computer lenses with a calmer hand.
What You Will Learn:
- Start with the truth, not the display rack: Know why astigmatism changes the buying decision.
- Understand SPH, CYL, AXIS, and ADD without prescription panic.
- Match the lens to the task: Choose between OTC readers, single-vision readers, bifocals, progressives, and occupational lenses.
- Protect the eyes behind the glasses: Use a senior-safe checklist before paying.
Fast Answer: The Lens Has to Correct More Than Near Blur
Seniors with astigmatism usually need more than basic drugstore reading glasses because astigmatism requires cylinder and axis correction, not just magnification. Over-the-counter readers may help mild near-vision blur, but they do not correct each eye’s full prescription. The safest first step is a current eye exam, then choosing single-vision readers, bifocals, progressives, or computer glasses based on reading distance, daily tasks, balance needs, and comfort.
Table of Contents
Safety First: When Glasses Shopping Is Really Health Screening
This article is for general education, not medical diagnosis or personal vision care. Seniors with astigmatism, sudden vision changes, eye pain, double vision, new headaches, or trouble seeing even with glasses should consult an optometrist or ophthalmologist. Over-the-counter readers can be convenient, but they are not a substitute for a full eye exam when astigmatism, cataracts, glaucoma risk, diabetes, macular degeneration, medication side effects, or fall risk may be involved.
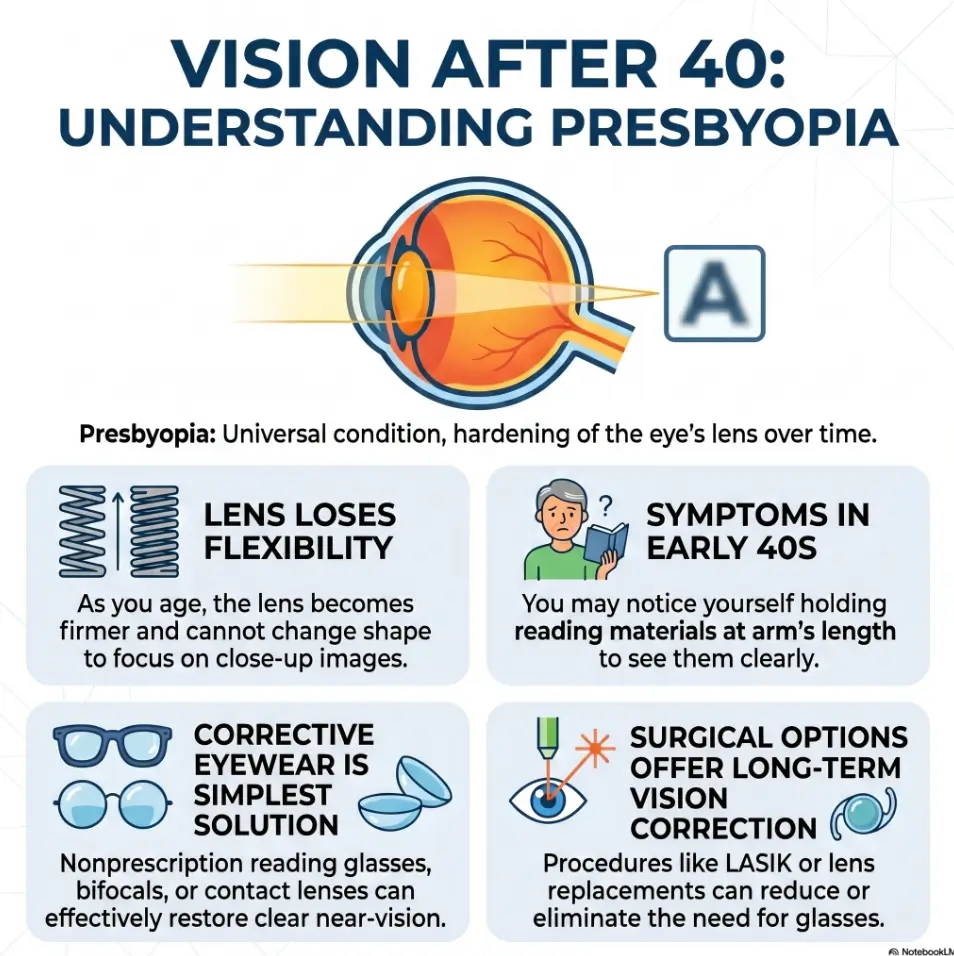
The National Eye Institute explains that presbyopia is a normal age-related near-vision change, and many people also have another refractive error at the same time. The American Academy of Ophthalmology also describes presbyopia as the age-related loss of near focusing ability. That means the question is not only “What power do I need?” It is also “What else might be changing?”
For a senior who is misreading medication labels, struggling with bills, or avoiding menus, glasses are not a vanity purchase. They are part of home safety. A pair that works for a crossword puzzle may still fail on a prescription bottle at 10 p.m. under a yellow kitchen light. The eyes do not live in a showroom. They live in the kitchen, the car, the pharmacy line, the church bulletin, and the little printed warnings nobody made large enough.
The Real Problem: Readers Magnify, Astigmatism Distorts
Why “+2.00” is only half the story
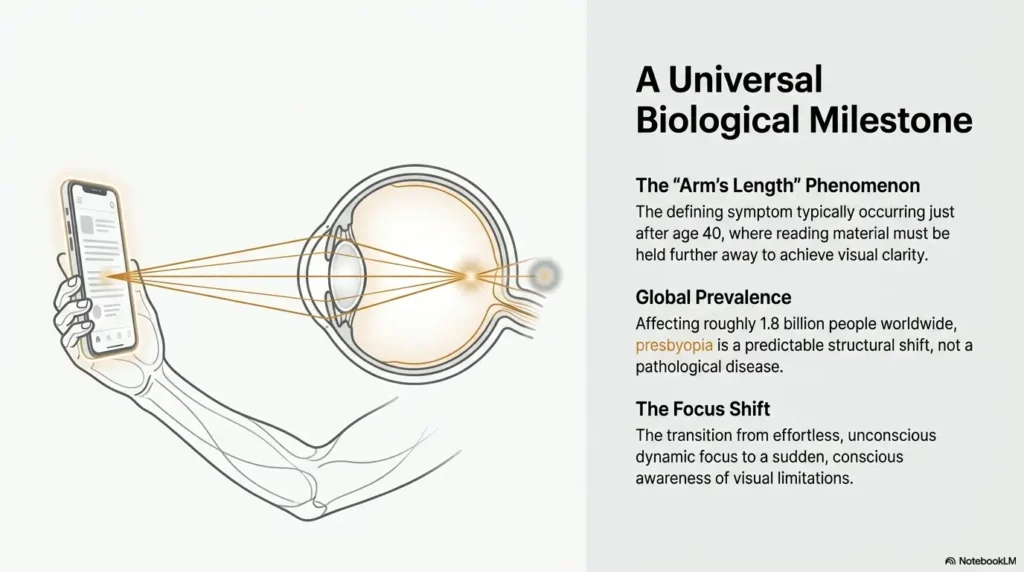
Standard reading glasses mainly add magnifying power for near work. That number, often written as +1.50, +2.00, or +2.50, helps with presbyopia. Presbyopia is the reason arms seem to get shorter after middle age. The book did not move. The lens inside the eye became less flexible.
Astigmatism is different. It usually means the eye’s front surface or internal lens focuses light unevenly. Instead of one clean focus point, light may form a blur line or shadow. A prescription corrects this with cylinder and axis numbers. That is why two people can both “need readers” but have completely different comfort levels in the same pair.
Think of basic readers as turning up the size. Astigmatism correction tunes the shape. If the shape is wrong, bigger blur is still blur. It just arrives wearing a larger hat.
The blur clue: letters look stretched, shadowed, or doubled
Uncorrected astigmatism often feels less like simple fuzz and more like distortion. Letters may look stretched, tilted, smeared, doubled, or shadowed. A black “E” on a white page may have a faint gray companion beside it. Numbers on a bill may seem to vibrate. A phone screen can look sharp for a moment, then tiring, especially when the print is small.
This is one reason seniors sometimes keep buying stronger readers without feeling truly satisfied. More magnification can make near print larger, but it cannot aim the astigmatism correction in the right direction. That direction is the axis. It is measured in degrees, and it is not something a store rack can guess by charm or fluorescent lighting.
Here’s what no one tells you…
A pair that “sort of works” for five minutes in a store may still fail during real life. Bills, medication labels, sewing, recipes, crosswords, text messages, sheet music, grocery receipts, and Bible study notes all ask different things from the eyes. The reading glasses that survive the cereal box test may not survive tax forms, and nobody wants to lose a Saturday afternoon to squinting at line 7b.
- Readers mainly add near power.
- Astigmatism needs cylinder and axis correction.
- Real-world reading tasks reveal problems faster than a store mirror.
Apply in 60 seconds: Look at a medicine label with your current readers and note whether the letters are small, distorted, or both.
Who This Is For, and Who Should Skip Straight to an Eye Doctor
Good fit: seniors comparing readers after a recent eye exam
This guide is useful if you already know you have astigmatism and want to make a smarter buying decision. Maybe the eye doctor gave you a prescription, but the optical shop conversation moved faster than a squirrel on espresso. Maybe you are helping a parent choose between dedicated readers, bifocals, progressives, or computer glasses. Maybe your current glasses work for books but not tablets.
It also helps if you are comparing online glasses, local optical shops, warehouse clubs, and drugstore readers. The goal is not to shame budget choices. The goal is to avoid buying the wrong thing three times, then deciding your eyes are “just old.” Age deserves more respect than that.
Not for: sudden blur, eye pain, flashes, or major vision changes
Skip shopping and seek professional care if vision changes suddenly, one eye becomes much blurrier, you see new flashes or many new floaters, eye pain appears, double vision begins, or you cannot read even with your usual correction. A stronger pair of readers is not a medical evaluation. It is plastic and hope, and hope is not licensed.
This is especially important for people with diabetes, glaucoma risk, cataracts, macular degeneration, recent eye surgery, recent falls, or neurological symptoms. Vision changes can come from many causes, including refractive changes, dry eye, medication effects, retinal problems, or brain-related visual issues. The safe path is to identify the cause before changing tools.
Caregiver note: watch the quiet compromises
Caregivers often notice vision problems before the senior names them. The clues can be quiet: more lamps turned on, menus avoided, bills pushed aside, phone font enlarged again, pill bottles held at a strange angle, or the familiar phrase, “My glasses are fine,” delivered while squinting like a lighthouse keeper.
If medication safety is part of the concern, pair glasses shopping with a home routine. A large-print medication list, better lighting, and clear labels can reduce errors. For practical home support, see this guide to low vision medication safety and this one-page medication list template.
Money Block: “Shop or See the Doctor?” Eligibility Checklist
Answer yes or no:
- Has the senior had an eye exam within the last year or two?
- Is the blur gradual, not sudden?
- Is there no eye pain, new double vision, flashes, or sudden vision loss?
- Is the goal routine near work, such as reading, phone use, or bills?
- Do you already know whether astigmatism is present?
Neutral action line: If any safety answer worries you, schedule an eye exam before buying another pair.
Prescription First: Decode SPH, CYL, AXIS, and ADD Without Panic
SPH tells the basic distance or near power
SPH stands for sphere. It is the basic focusing power of the lens. A minus number usually corrects nearsightedness. A plus number usually corrects farsightedness or near support, depending on how the prescription is written. For reading glasses, the near power may be built from distance correction plus the ADD value.
Do not worry if the prescription looks like a tiny algebra quiz. You do not need to become an optician overnight. You only need to know that a complete prescription contains more information than the single number printed on a pair of drugstore readers.
CYL and AXIS are the astigmatism coordinates
CYL stands for cylinder. It tells how much astigmatism correction is needed. AXIS tells where that correction sits, measured from 0 to 180 degrees. These two numbers travel together. Cylinder without axis is like giving someone a house number without the street name.
Prescription reading glasses can include this correction. Generic readers usually cannot. That difference matters most when astigmatism is moderate, when the eyes differ from each other, or when the reader needs long sessions of fine print. A senior who reads ten minutes of mail may tolerate more compromise than someone who sews, studies music, reads medication instructions, or works at a computer.
ADD is the near-vision boost
ADD is the extra plus power used for near vision. It is commonly used for presbyopia. In multifocal prescriptions, ADD helps create the near portion of bifocals, trifocals, or progressive lenses. It also helps determine dedicated prescription readers.
ADD is not one-size-fits-all. Reading distance matters. A person who reads paperback books at 14 inches may need a different setup than someone who uses a laptop at 24 inches. A pianist reading sheet music at arm’s length may feel trapped by ordinary readers. The music is not blurry because Beethoven was inconsiderate. The lens distance is wrong.
Show me the nerdy details
Near lenses work by changing the focal demand placed on the eye. A close book requires more focusing power than a computer screen farther away. Presbyopia reduces the eye’s ability to add that focus naturally, so plus power supplies part of the missing focusing effort. Astigmatism correction adds a separate cylindrical component at a specific axis so light focuses more evenly. This is why two prescriptions with the same ADD can feel very different if one includes cylinder and axis correction and the other does not.
Don’t Buy the Strongest Pair: The Over-Magnification Trap
Why stronger readers can feel good, then betray you
Stronger readers can seem wonderful for a minute because they make near print larger and bolder. Then the trapdoor opens. The working distance becomes too short. The reader hunches closer. The neck tightens. The page looks clear only in a narrow zone. The phone becomes crisp, but the recipe on the counter turns useless.
Over-magnification can also make computer use miserable. If the glasses are too strong, the screen may demand that the user sit too close. That can lead to shoulder tension, dry eye from reduced blinking, and the mysterious feeling that the laptop has developed an attitude.
The 10-minute test beats the 10-second test
Testing reading glasses for ten seconds is like test-driving a car by honking the horn. It gives information, but not enough. Use the glasses for at least ten minutes with real materials: a medication label, a utility bill, a paperback, a phone, and a recipe card. Notice clarity, posture, eye strain, and whether the print stays comfortable without moving the item around constantly.
Use normal lighting too. A bright store can hide problems that reappear at home. If the senior usually reads in a recliner under a side lamp, test that kind of distance and angle. Vision is practical. It belongs to chairs, counters, screens, and habits.
Let’s be honest… the display rack is not an eye clinic
A store rack cannot measure astigmatism, unequal prescriptions, pupillary distance, eye teaming, cataract changes, retinal health, or the exact distance where the person reads. It offers convenience, not diagnosis. That does not make OTC readers bad. It makes them limited.
For simple presbyopia with similar eyes and no meaningful astigmatism, over-the-counter readers may be enough for some tasks. For seniors with astigmatism, they are more likely to be a temporary tool than a complete solution.
Print is small but not shadowed. Eyes feel similar. Recent exam is reassuring.
Likely path: OTC or prescription readers.
Words smear, double, tilt, or look clearer in one direction.
Likely path: Prescription lenses with CYL and AXIS.
Book is fine, computer is not. Phone works, sheet music does not.
Likely path: Separate task lenses or occupational lenses.
Sudden blur, pain, flashes, double vision, or major change.
Likely path: Eye doctor before shopping.
OTC Readers vs Prescription Reading Glasses: The Decision Point
OTC readers may work for simple presbyopia
Over-the-counter readers can be useful for people who mainly need near magnification and whose eyes are similar enough to share the same power. They are affordable, easy to replace, and handy as backup pairs in a drawer, handbag, desk, or kitchen. They can be the umbrella of vision care: not a roof, but better than getting soaked.
They are less helpful when astigmatism matters, when one eye needs a different prescription, when the person has a high prescription, or when comfort over long sessions is the goal. Mayo Clinic’s patient education on presbyopia notes that nonprescription readers may help some people, but regular eye exams still matter because near blur can coexist with other eye concerns.
Prescription readers win when each eye needs different help
Prescription reading glasses can include sphere, cylinder, axis, ADD, and pupillary distance. They can correct each eye separately and place the optical centers more accurately. That matters for seniors who read for longer periods, have moderate astigmatism, or get headaches with generic readers.
They may also help when a senior has had cataract surgery, because one eye may not match the other exactly afterward. For people dealing with different prescriptions between eyes, anisometropia after cataract surgery can make ordinary readers feel especially strange.
Cost tradeoff: cheap pairs, expensive frustration
Drugstore readers are cheaper per pair. Prescription readers cost more upfront. But the real comparison is not sticker price alone. It is the cost of wasted pairs, headaches, return trips, poor posture, and daily annoyance. A $12 pair that sits unused in a junk drawer is not a bargain. It is a small plastic memorial to optimism.
Money Block: OTC vs Prescription Decision Card
| Choose OTC readers when… | Choose prescription readers when… |
|---|---|
| The main issue is simple near blur. | Astigmatism correction is needed. |
| Both eyes feel similar. | Each eye has a different prescription. |
| You need a backup pair for short tasks. | You read, sew, work, cook, or manage medication often. |
Neutral action line: Use OTC readers as a convenience tool, not a replacement for astigmatism correction when your prescription calls for it.
Lens Type Matters: Single-Vision, Bifocal, Trifocal, or Progressive?
Single-vision readers: best for books, phones, and close tasks
Single-vision reading glasses have one power across the whole lens. They are often the simplest choice for dedicated near work. If a senior sits down to read, knit, pay bills, or use a phone, single-vision readers can provide a wide, steady area of clarity.
The tradeoff is distance blur while wearing them. Many people perch them low on the nose or take them on and off. That can be fine for occasional reading. It can become annoying if the person switches constantly between a book, TV, and conversation.
Bifocals: useful when distance and near tasks switch often
Bifocals combine distance and near correction in one lens, usually with a visible line. The upper part helps with distance. The lower part helps with reading. They can be practical for seniors who want fewer glasses and do not mind the line.
The visible line can also be useful because it tells the eyes where the near zone begins. Some people like that certainty. Others dislike the image jump when looking across the boundary. There is no moral victory in choosing one over the other. The best lens is the one the senior actually wears without muttering.
Progressives: elegant, but not always effortless
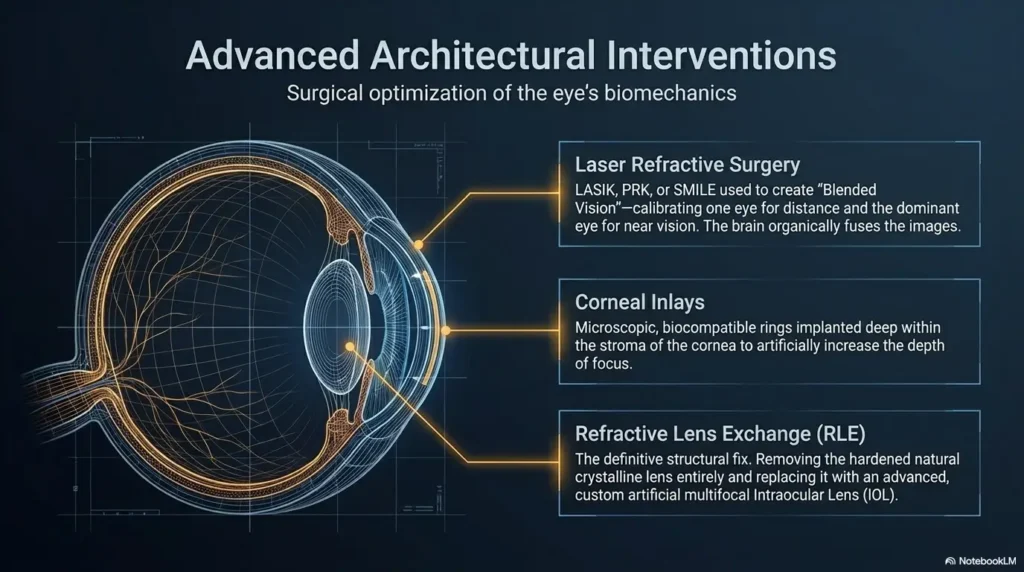
Progressive lenses offer distance, intermediate, and near correction without a visible line. They can be excellent for astigmatism because the prescription can include cylinder and axis while also supporting several distances. But they require adaptation. The wearer learns to point the nose a bit more, use the correct zone, and avoid looking through the near area while walking downstairs.
For seniors with balance problems, dizziness, neuropathy, a history of falls, or difficulty adapting, progressives deserve careful discussion. Some people love them. Others do better with separate readers and distance glasses. If walking safety is already a concern, review aging vision and fall prevention at home before choosing a lens that changes the view near the feet.
Occupational lenses: the hidden hero for computer-plus-paper work
Occupational lenses are designed for specific task distances, often intermediate and near. They can be wonderful for computer work, music stands, tablets, cooking, crafts, and home offices. Instead of trying to make one pair do everything, they make one pair do a few common tasks very well.
A senior who spends mornings at a desktop computer and afternoons reading mail may not need stronger readers. They may need the right working-distance lens. That is a quieter solution, but often a better one.
- Single-vision readers give a broad near zone.
- Bifocals help with distance-to-near switching.
- Progressives are flexible but require adaptation and careful fit.
Apply in 60 seconds: Name the three tasks you do most often before deciding on lens type.
Reading Distance Changes Everything: Book, Phone, Tablet, Computer
Measure the distance before choosing the lens
Before buying reading glasses, measure the actual distance from the eyes to the task. Do not guess. Use a tape measure or a piece of string. A paperback may sit at 14 to 16 inches. A tablet may sit at 18 inches. A laptop may sit at 22 to 28 inches. A desktop monitor may sit even farther away.
This small measurement can prevent a large mistake. Lens power is tied to working distance. A pair that feels great for a phone may be too strong for a computer. A pair that works at a laptop may not help with tiny print on a pill bottle.
Computer readers usually need less power than book readers
Computer screens usually sit farther from the eyes than books. Because of that, computer readers often need less plus power than close reading glasses. A senior using full-strength book readers at a monitor may lean forward, lift the chin, or peer through the wrong part of a multifocal lens. The result can be neck pain and tired eyes.
For screen-heavy days, reduce glare too. An anti-glare screen protector may help some users, especially when reflections from windows or overhead lights turn the screen into a mirror. For practical setup help, see anti-glare screen protector guidance and digital eye strain in seniors.
Tiny print is not the same as close distance
Tiny print tempts people to reach for stronger lenses, but size is only one part of readability. Lighting, contrast, paper glare, font style, and visual field all matter. Glossy mail can be harder than matte paper. A gray label can be worse than a black-and-white one. Small print on a curved pill bottle can feel like a message from a mischievous ant colony, except nobody invited the ants.
Before increasing power, improve the environment. Add a well-positioned reading lamp. Reduce glare. Use larger print when available. For pill bottles, a phone magnifier or label-reading routine may help. You might pair glasses with iPhone Magnifier filters for pill bottles or a system for reading expiration dates with low vision.
Money Block: 3-Input Reading Distance Mini Calculator
This simple tool does not prescribe glasses. It helps you sort tasks before talking with an eye care professional.
Neutral action line: Bring these distances to your eye exam or optical fitting.
Frame Fit: The Comfort Detail Seniors Notice First
Pupillary distance is not decoration
Pupillary distance, often called PD, is the distance between the centers of the pupils. It helps place the lens centers correctly in front of the eyes. This matters for prescription lenses and can matter even more with progressives, stronger prescriptions, or astigmatism correction.
If the optical center is poorly aligned, the glasses may cause strain, swim, or a sense that the eyes are working too hard. The wearer may blame the prescription, but the problem can be placement. Good glasses are not only the right numbers. They are the right numbers in the right place.
Nose pads, bridge fit, and temple pressure matter
Seniors may notice comfort before optical precision. Nose pads can pinch. A bridge can slide. Temples can press behind hearing aids. Frames can compete with oxygen tubes, sensitive skin, or arthritis-related handling issues. Lightweight frames may matter more than style, especially for long reading sessions.
Caregivers should watch whether the glasses leave marks, slide down, tilt, or get removed quickly. A senior who says “they work” but takes them off after three minutes may be reporting a comfort problem, not a vision success.
Bigger is not always better
Bigger lenses can provide more viewing area, but they can also add weight. Progressives and bifocals need enough lens height for the zones to work properly. Tiny frames may look neat but leave too little room. Very large frames may slide, distort, or feel heavy.
The sweet spot is task-specific: enough lens height for the design, enough width for natural eye movement, and enough comfort for real use. If the senior reads in bed, cooks from recipes, or sits at a computer, the frame should be tested in those head positions when possible.
Short Story: The Paperback, the Pill Bottle, and the Purple Frames
Margaret brought three pairs of readers to her daughter’s kitchen table. One pair was scratched, one was too strong, and one had purple frames she loved but never wore. “These are my good ones,” she said, holding up the purple pair like a tiny trophy. Then she tried to read a pill bottle.
The letters looked larger, but the shadows made the dosage line uncertain. Her daughter noticed Margaret tilted the bottle, then tilted her head, then laughed it off. They wrote down the prescription date, measured her reading distance, and asked the optical shop whether the new readers would include astigmatism correction. Two weeks later, Margaret still loved purple frames, but now the lenses matched her eyes. The lesson was gentle: style can invite use, but correction and fit do the daily work.
Common Mistakes That Turn Reading Glasses Into a Daily Annoyance
Mistake 1: using someone else’s readers
Borrowed readers are tempting. They sit on the counter. They seem close enough. They are also made for someone else’s eyes, distance, prescription, habits, and tolerance. With astigmatism, borrowing becomes even less reliable because cylinder and axis correction are personal.
Using another person’s readers for one emergency label is not the same as using them daily. If a senior regularly reaches for a spouse’s glasses, it is time to get a proper assessment. Romance is lovely. Shared astigmatism correction is not usually part of the vows.
Mistake 2: buying one pair for every task
One pair may not handle phone, computer, piano, crafts, books, mail, and recipes equally well. Different tasks happen at different distances and angles. A person who cooks from a recipe card on the counter may need a different focal range than someone reading in a recliner.
For seniors with low vision or mixed vision challenges, support tools may matter too. A stand magnifier can reduce hand strain for tremor, while better lighting can make print more readable. Compare options with handheld vs stand magnifier choices for tremor and reading lamp position for central vision loss.
Mistake 3: ignoring lighting and contrast
Poor lighting can mimic a glasses problem. So can glare. A senior may think the prescription is wrong when the actual enemy is glossy paper under a bright overhead fixture. The page shines. The letters fade. The reader blames the eyes, the glasses, and possibly the entire postal system.
Improve contrast before changing power. Use matte surfaces, adjustable lamps, larger print, high-contrast labels, and reduced glare. For mail and home surfaces, reading glossy mail without glare and matte vs glossy paint choices can support the same goal.
Mistake 4: blaming age when the prescription changed
It is easy to say, “I’m just getting older.” Sometimes that is partly true. But vision changes after 60 deserve attention, not resignation. Cataracts, glaucoma, macular degeneration, diabetic eye disease, medication effects, dry eye, and refractive shifts can all affect clarity.
If reading becomes harder even with the same glasses, do not simply keep increasing reader strength. Use the change as a signal. A current eye exam can separate a lens problem from an eye health problem. For warning signs beyond ordinary aging, see senior vision changes warning signs.
- Do not borrow daily readers from someone else.
- Do not expect one pair to serve every distance.
- Do not ignore new or changing symptoms.
Apply in 60 seconds: Write “lighting, distance, fit, prescription date” on a note before buying another pair.
The Senior-Safe Shopping Checklist Before You Pay
Confirm the prescription date
Start with the date. If the prescription is old or vision has changed, update the exam first. Seniors with diabetes, glaucoma risk, cataracts, macular degeneration, or recent surgery may need more specific follow-up. The American Academy of Ophthalmology and the National Eye Institute both emphasize the importance of eye exams for detecting conditions that glasses alone cannot reveal.
If Medicare or insurance questions are part of the decision, remember that routine refraction and glasses coverage can differ from medical eye care. For coverage context, review Medicare refraction fee basics and Medicare glasses after cataract surgery.
Ask whether astigmatism correction is included
This is the key question: “Do these glasses correct my astigmatism for the distance I actually use most?” Ask it online, in-store, or at the optical shop. If the answer is unclear, slow down. You are not being difficult. You are buying a medical-adjacent tool that sits on the face and negotiates with the brain all day.
For online glasses, confirm that you entered SPH, CYL, AXIS, ADD if needed, and pupillary distance. Check whether the site supports prescription readers with astigmatism correction. Some “readers” pages sell magnification only. That may not be enough.
Check return and remake policies
Return and remake policies matter, especially for progressives, bifocals, and first-time prescription readers. Ask how long the adjustment window lasts. Ask whether non-adaptation to progressives is covered. Ask whether frame fit changes are free. Ask what happens if the prescription was entered incorrectly.
Progressives in particular can be sensitive to measurements and frame position. A generous remake policy is not a luxury. It is a cushion between your wallet and the unpredictable theater of human adaptation.
Bring the real-world reading sample
Bring the actual things the senior needs to read: medication labels, paperback pages, tablet, phone, craft pattern, sheet music, grocery receipt, church bulletin, menu, or utility bill. The tiny paper kingdom matters. It shows what the glasses must do beyond a neat eye chart.
If medication labels are the pain point, also consider large-print labels and pharmacy support. These pair well with the right glasses. For practical scripts and systems, see a low vision pharmacy help script and large-print prescription labels.
Money Block: Quote-Prep List for Prescription Reading Glasses
- Current prescription with SPH, CYL, AXIS, and ADD.
- Pupillary distance, especially for online orders.
- Main reading distance in inches.
- Top three tasks: phone, computer, books, medication labels, crafts, music, or cooking.
- Frame comfort needs: hearing aids, sensitive nose bridge, arthritis, oxygen tubing, or balance concerns.
- Return, remake, and progressive adaptation policy.
Neutral action line: Compare glasses using the same task list, not only the lowest advertised price.
When to Seek Help Instead of Trying Another Pair
New or sudden vision changes
Seek prompt professional care for sudden blur, sudden vision loss, new double vision, flashes, many new floaters, eye pain, or a curtain-like shadow. These symptoms should not be treated as shopping clues. They are medical clues. The next step is evaluation, not +3.00 readers.
For older adults, sudden changes can be especially important because eye disease, circulation problems, medication effects, and neurological issues may overlap. When in doubt, choose care over guessing.
Headaches, nausea, or eye strain that keeps returning
Recurring headaches or eye strain can come from the wrong prescription, poor fit, uncorrected astigmatism, binocular vision issues, dry eye, lighting problems, or posture strain. The pattern matters. If discomfort appears after reading for ten minutes, at the computer, or when switching distances, write it down.
A symptom diary can make appointments more useful. Include when symptoms happen, what glasses were used, what task was involved, and whether one eye seems worse. A simple diary often reveals the culprit faster than memory, which tends to file everything under “Tuesday was annoying.”
Trouble with walking, stairs, or depth perception
Multifocal lenses can affect how the floor, stairs, and curbs look, especially during adaptation. A senior who feels unsure walking in progressives should not be told to “just get used to it” without review. Balance and fall risk matter.
Some people use distance-only glasses for walking and dedicated readers for near tasks. Others adapt well to progressives with careful fitting. The right answer depends on vision, mobility, habits, and safety. If low vision walking is part of the picture, low vision walking guidance can support safer routines.
Diabetes, cataracts, glaucoma, or macular degeneration history
Readers may help near focus, but they cannot monitor eye disease. People with diabetes need appropriate eye care because diabetic eye disease can threaten vision before symptoms feel dramatic. Cataracts can change prescription and glare. Glaucoma can affect field of view. Macular degeneration can affect central reading ability.
If the senior has known eye disease, glasses are only one layer of the plan. Home safety, lighting, magnification, medication systems, and routine medical follow-up all matter. Related guides include glaucoma field loss home safety, low vision reading for an 80-year-old with AMD, and how often seniors should get dilated eye exams.
- Sudden changes need prompt attention.
- Progressive lens discomfort can affect mobility.
- Eye disease history changes the risk level.
Apply in 60 seconds: Write down whether the problem is new, worsening, task-specific, or constant.
FAQ
Can seniors with astigmatism use drugstore reading glasses?
Yes, but only in limited cases. Standard drugstore readers may help near magnification, but they usually do not correct astigmatism. If letters look shadowed, stretched, or doubled, or if one eye needs different correction, prescription reading glasses are usually the more comfortable and safer route.
What type of reading glasses are best for astigmatism?
Prescription reading glasses are usually best because they can include sphere, cylinder, axis, and near ADD power. The best format may be single-vision readers, bifocals, progressives, or occupational lenses depending on reading distance, computer use, balance needs, and how often the senior switches tasks.
Why do my reading glasses make letters look shadowed?
Shadowed or doubled letters can happen when astigmatism is not corrected, the lens power is wrong, the frame fit is off, or the optical centers do not line up well with the eyes. It can also happen when cataracts, dry eye, or other eye conditions reduce clarity. If the problem persists, schedule an eye exam.
Are progressive lenses good for seniors with astigmatism?
Progressive lenses can work well for seniors with astigmatism because they can include full prescription correction across several distances. However, comfort depends on accurate measurements, frame fit, lens design, adaptation time, and mobility needs. Seniors with balance concerns may need extra caution around stairs and curbs.
Do I need separate computer glasses if I have astigmatism?
Possibly. Computer screens usually sit farther away than books, so full-strength reading glasses may be too strong for screen work. Prescription computer glasses or occupational lenses can include astigmatism correction while matching the intermediate distance more comfortably.
How often should seniors update reading glasses?
A practical rule is to update reading glasses when vision changes, headaches appear, reading becomes harder, the glasses no longer match daily tasks, or an eye doctor recommends a new prescription. Seniors with diabetes, glaucoma risk, cataracts, macular degeneration, or recent surgery should follow their clinician’s exam schedule.
Can the wrong readers damage my eyes?
Wrong readers usually do not permanently damage healthy eyes, but they can cause eye strain, headaches, neck pain, poor posture, and avoidable frustration. The larger risk is delay: a senior may keep buying stronger readers while an eye health problem goes unchecked.
Should caregivers help choose reading glasses?
Yes, especially when the senior misreads medication labels, avoids reading, has memory issues, struggles with fit, or feels embarrassed asking for help. Caregivers can bring real-world reading samples, check return policies, measure reading distances, and watch for quiet signs of strain.
Next Step: Do the Two-Paper Test Today
Paper 1: write down the actual reading tasks
Take one sheet of paper and list the tasks that matter: phone, tablet, books, medication labels, computer, recipes, crafts, bills, mail, sheet music, menus, and church bulletins. Put a star beside the top three. Those top three should guide the glasses decision more than a random rack strength.
Next, write the rough distance beside each task. Do not chase perfection. A quick measurement is enough. If the book is 15 inches away and the computer is 26 inches away, those are not the same visual job.
Paper 2: write down the current prescription numbers
On the second sheet, copy the prescription numbers: SPH, CYL, AXIS, ADD, prescription date, and any notes from the eye doctor. Also write down known conditions such as cataracts, glaucoma, diabetes, macular degeneration, double vision, dry eye, or recent surgery.
This page turns a vague shopping trip into a focused conversation. It also helps caregivers, optical shops, and online ordering forms stay honest. The paper does not have to be elegant. It only has to stop the guessing.
Then ask one clean question
The clean question is: “Do these glasses correct my astigmatism for the distance I actually use most?” If the answer is yes, you are closer to a useful purchase. If the answer is no, you may be looking at magnifiers, not full reading correction.
For seniors with broader vision challenges, combine glasses with practical supports. A low vision clock, bump dots or tactile tape, and low vision bedside organization can reduce daily friction while the right prescription handles the optical work.
Money Block: Five-Tier Comfort Map
| Tier | Setup | Best for |
|---|---|---|
| Tier 1 | OTC readers | Short, simple near tasks without meaningful astigmatism correction needs. |
| Tier 2 | Prescription single-vision readers | Books, bills, phone, labels, and longer reading sessions. |
| Tier 3 | Bifocals | Switching between distance and near with a visible line. |
| Tier 4 | Progressives | Multiple distances in one pair, if adaptation and balance are good. |
| Tier 5 | Occupational lenses plus home supports | Computer, crafts, music, kitchen work, and low-vision-friendly routines. |
Neutral action line: Start at the lowest tier that truly solves the task, then move up only when comfort or safety requires it.
Conclusion: Stop Chasing Strength and Start Matching the Job
The display rack makes reading glasses look like a simple strength contest. For seniors with astigmatism, that is the wrong game. The better question is not “How strong should the readers be?” It is “What correction does each eye need, and at what distance will these glasses be used?”
That shift protects comfort, safety, and confidence. It helps separate presbyopia from astigmatism, a bargain from a compromise, and ordinary near blur from symptoms that deserve care. It also respects the daily reality of older eyes: medication labels, tablet screens, stairs, recipes, bills, and the paperback waiting patiently beside the chair.
Your 15-minute next step is simple: write down the top three reading tasks, measure each distance, and copy the current prescription date plus SPH, CYL, AXIS, and ADD. Then ask one clean question before buying: “Do these glasses correct my astigmatism for the distance I actually use most?”
Last reviewed: 2026-05.