


Beyond the “Lighting Problem”: Navigating Senior Vision Changes
It began as a “lighting problem,” the kind you try to solve with a brighter bulb and a shrug. Then the porch steps started feeling unpredictable, faces at church went oddly soft, and night driving turned into an exhausting glare festival.
These are the real-life patterns seniors describe before anyone says the words “vision loss.” It’s not always a dramatic blur; often, it’s a series of small negotiations with stairs, labels, headlights, and confidence. Left unaddressed, the cost isn’t just annoyance—it’s falls, near-misses, and a quiet withdrawal from the life you love.
This guide helps you spot changes as they actually appear, separating normal aging from “get checked” signals. We’ll cover plain-English patterns linked to cataracts, macular degeneration, glaucoma, diabetic eye disease, and dry eye, providing a 7-day log to make your next exam more productive. No diagnosis games—just a clear triage map and a plan.
🔍 What to Notice First
Identify the subtle shifts in depth perception and clarity before they escalate.
🚫 What to Stop Normalizing
Distinguish between expected aging and red flags that require professional intervention.
📝 What to Write Down Today
Start your 7-day symptom log to provide your doctor with concrete, actionable data.
🚨 When “Soon” Becomes “Now”
Recognize the emergency signals that demand immediate medical attention.
Table of Contents
1) That first clue: “Something’s off” moments seniors describe
The porch steps looked different overnight (depth perception shifts)
One morning, my neighbor (late 70s, proud of his independence) paused at the porch steps like they’d been rearranged overnight. He joked about “the carpenter doing midnight renovations.” But what he meant was: the step edge didn’t pop the way it used to.
Depth perception changes can show up as subtle “hesitation moments” before you even call them symptoms. People describe:
- Misjudging the last stair (especially in dim hallways)
- Reaching for a countertop and landing slightly short
- Feeling unsteady when transitioning from bright outdoors to a darker entryway
My own tell, when I was caregiving for a relative: the way she started “testing” a step with her toe before committing. Not dramatic. Just a tiny negotiation with gravity.
Faces went soft at church, but street signs stayed sharp (contrast loss)
This one is classic in true stories of vision loss in seniors: “I can read signs, but faces feel… smudged.” That isn’t you being picky. Contrast is how the brain separates edges, and when contrast drops, the world can feel like it’s been lightly fogged.
A friend once described it perfectly: “It’s not blur. It’s softness.” You can still pass a quick vision screen and still struggle socially, because social recognition isn’t a Snellen chart. It’s life at a messy angle.
Night driving turned into a guessing game (glare halos, slow adaptation)
One of the most repeated lines I hear from older adults: “Daytime is fine. Night is… exhausting.” Headlights bloom. Streetlights wear halos. The road looks shiny even when it’s dry.
And here’s the part people underplay: night driving difficulty isn’t only about eyesight. It’s about reaction time, fatigue, and confidence. When someone says, “I just avoid highways now,” they’re often already self-triaging, and it’s worth reading a practical safety guide like night driving after 70 alongside your symptom notes.
Pattern-interrupt: Let’s be honest… we normalize weird vision for months
Humans adapt. That’s our superpower and also our little sabotage artist. We start turning our head more. We hold menus farther. We blame bulbs, screens, “dry air,” “bad print.” Then one day, a moment breaks the spell.
- Notice hesitation moments, not just constant blur
- Contrast problems can hide behind “I can still read”
- Night issues often show up before daytime issues
Apply in 60 seconds: Write down one daily task that recently got harder and when it happens (day, night, bright, dim).
Quick Eligibility Checklist: “Is this worth booking an eye exam?”
Answer yes/no. This doesn’t diagnose anything. It simply tells you whether you have enough signal to stop waiting.
- Yes/No: I avoid night driving more than I did 3–6 months ago.
- Yes/No: Stairs/curbs feel less predictable (especially in dim light).
- Yes/No: Faces look “soft” or hard to recognize in normal settings.
- Yes/No: Glare is new, worse, or more tiring than before.
Neutral next step: If you answered “yes” to any 2 items, schedule a routine eye exam and bring one week of notes (this annual eye exam checklist for seniors can help you prep without overthinking it).
2) The day the light changed: when “lighting” wasn’t the problem
“I thought my bulbs were dying” (low-light sensitivity)
Older eyes do need more light for the same tasks, and almost everyone knows that. But stories usually start like this: “I changed every bulb in the kitchen and it still felt dim.”
I once stood in a hallway with my dad, both of us looking at the same lamp. He said, “It’s barely on.” I said, “It’s bright.” We weren’t disagreeing. We were describing two different visual realities.
“The sun felt louder” (photophobia and glare)
Some people describe light sensitivity like a volume knob. The sun “shouts.” Headlights “scream.” And they start squinting not because they’re dramatic, but because their eyes are trying to protect the signal.
Glare can also turn ordinary scenes into a washout: a white plate on a white table, a pale sidewalk, a bright phone screen. It’s not just discomfort. It’s functional loss.
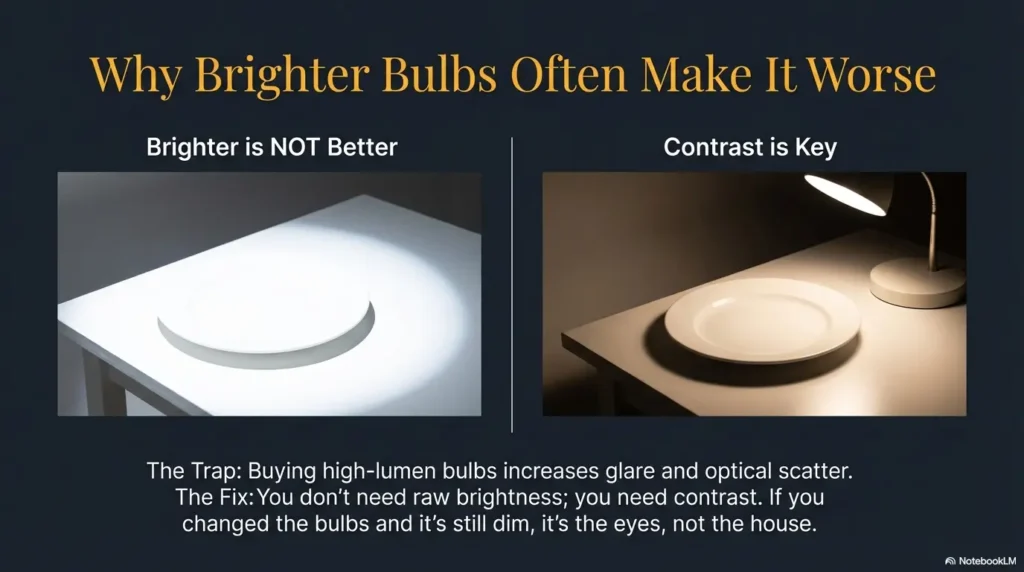
Why brighter isn’t always better (washout + reduced contrast)
More light can help, but the wrong kind of light can add glare and flatten contrast. Seniors sometimes buy a brighter lamp and then feel worse and assume they’re “getting anxious.” Nope. It might be the lighting choice. (If you’re troubleshooting glare at home, glare-free under-cabinet lighting is the kind of boringly-effective tweak that can reduce visual “noise.”)
Try this: softer, indirect lighting plus a focused task light. If that helps, keep it. If it doesn’t, that’s information too.
Open loop: The one lighting fix that can help, and when it can’t
The most reliable “cheap fix” I’ve seen is reducing glare rather than blasting brightness: matte shades, repositioning lamps so bulbs aren’t in the line of sight, and using warm, even illumination. If glare is the issue, glare reduction feels like relief.
But if you’re dealing with something like cataract glare, macular changes, or other eye conditions, lighting tweaks can improve comfort without solving the core problem. That’s why your notes matter: they tell you whether a workaround is helping or merely hiding the slope.
Show me the nerdy details
Lighting changes the “signal-to-noise” ratio for vision. Glare increases optical scatter and reduces contrast at the retina level, while uneven lighting forces constant adaptation. Task lighting works because it raises contrast on the specific target (labels, pages) without flooding the whole field with reflective noise.
3) Stories you don’t forget: the moment independence felt fragile
The missed curb, the spilled kettle, the wrong pill bottle
These are the moments people remember with surprising emotion, even years later. Not because of the injury (sometimes there isn’t one), but because the body sends a message: “You can’t autopilot this anymore.”
One caregiver told me her mother stopped cooking after she poured boiling water into the wrong mug. Not a catastrophe, but enough fear to rewrite the routine. Another described a missed curb that “shook my trust in my own legs.”
Reading fatigue: when the page “moves” after 10 minutes
This is common and often dismissed: “My eyes get tired.” But the story details matter. Does text double? Do lines drift? Does the page feel like it’s breathing? If reading fatigue has a specific time threshold (5 minutes, 10 minutes, 20 minutes), that’s useful information (and if your pattern clusters around long reading sessions, it’s worth checking dry eyes from reading and screen-driven strain as possible contributors).
I remember sitting with a relative who used to love novels. She started reading in two-minute bursts like she was rationing oxygen. That was her quiet clue.
The social cost: withdrawing because you can’t recognize faces
When faces are hard to read, people withdraw to avoid awkwardness. They stop going to groups. They skip church. They dodge events where names matter. The outside world sees “less social.” The inside world feels like a daily test you didn’t study for.
Pattern-interrupt: Here’s what no one tells you… vision loss is a confidence injury, too
Vision loss stories don’t just describe eyes. They describe identity. The “I’m capable” feeling gets bruised. And bruises change behavior.
Short Story: The Grocery Aisle That Changed Everything (120–180 words) …
It happened in the cereal aisle, which is not where anyone expects an existential moment. My uncle had a list, his glasses, and the stubborn pride of a man who’d built a life from tools and deadlines. He stood there longer than usual, then asked me, softly, “Which one is the oat one?” I pointed. He nodded like he understood, then reached for the wrong box. He laughed it off, but his laugh had a crack in it.
At checkout, he handed the cashier a bill and paused when she said the total. Later, in the car, he stared at the dashboard lights as if they were written in a language he used to speak fluently. “Maybe I’m just tired,” he said. But it wasn’t tired. It was a new rule of the world: the details were no longer volunteering. That week, we booked an eye exam and made a medication list together using a simple one-page medication list template. He didn’t lose independence that day. He gained a plan.
Decision Card: When A vs B (no drama, just trade-offs)
| Choose A | Choose B |
|---|---|
| A: Adjust home lighting + add magnification Best when comfort improves and function returns. |
B: Book an eye exam soon Best when symptoms affect safety or keep changing. |
| Time cost: 30–60 minutes setup | Time cost: appointment + travel (often 1–3 hours total) |
| Risk: may mask progression | Risk: minimal, but don’t wait if urgent signs show up |
Neutral next step: If safety tasks (stairs, driving, pills) are affected, treat it as an exam decision, not a “better bulb” project.
4) What was actually happening: common causes behind these stories (plain-English)
Let’s keep this grounded: stories can hint at patterns, but only an eye professional can diagnose. What follows is “plain-English pattern matching,” the way people describe symptoms before they know the name.
Cataracts: glare, haze, and “my glasses stopped working”
Many seniors describe cataract-like changes as a foggy windshield feeling or a glare explosion at night. People often say, “I updated my glasses twice and it still wasn’t right.” That’s a common story element (especially when early cataract signs are subtle and easy to blame on “lighting”).
Macular degeneration: missing spots, warped lines, central blur
When people describe straight lines bending, a “smudge” in the center, or faces becoming the hardest thing, macular issues are often part of the conversation. A caregiver once told me: “She could see the room, but not the person.” That stuck with me. If night glare is the headline symptom, this resource on macular degeneration and night driving safety can help you frame the risk in daily-life terms.
Glaucoma: the slow steal of side vision (often silent)
Glaucoma is famous for being quiet. People might not notice peripheral loss until they bump into things or miss objects off to the side. That’s why routine checks matter even when someone feels “fine” (and why comparing glaucoma vs normal aging symptoms can clarify what’s “common” versus what’s “don’t ignore”).
Diabetic eye disease: fluctuating blur and sudden changes
For people with diabetes, vision changes may fluctuate and sometimes shift quickly. If a person says, “It’s better some days, worse others,” and diabetes is in the picture, it’s worth mentioning to the clinician right away (and if you’re working on small daily habits, even a simple post-meal walk strategy for diabetic retinopathy risk can be part of the broader care conversation).
Medication side effects + dry eye: the “it depends on the day” pattern
Dry eye can cause blurry, fluctuating vision that improves with blinking or worsens with screens and wind. Medication side effects can contribute too, especially in polypharmacy situations. This is why a medication and supplement list matters, even when it feels unrelated to eyes (start here: polypharmacy and vision problems, then narrow down symptoms like medication-related dry eye if dryness is part of the story).
Open loop: Why two people can have “20/20” and still struggle to drive at night
Because “20/20” measures one thing: sharpness under ideal conditions. Night driving is a whole orchestra: contrast sensitivity, glare recovery, pupil changes, tear film stability, and cognitive load. In real life, you don’t drive through an optometrist’s chart. You drive through weather, reflections, and surprise (this is also why practical guides like senior driving safety can matter even before anyone has a final diagnosis).
- Chart sharpness isn’t the same as real-world function
- Fluctuation is a clue, not a contradiction
- Glare + night problems deserve respect
Apply in 60 seconds: Write one sentence: “My hardest visual task is ___ and it’s worse when ___.” Bring that to the appointment.
5) Who this is for / not for: read this with the right expectations
For: seniors noticing changes, caregivers, adult children, anyone post-surgery
If you’re searching “the day I realized my vision changed forever,” you’re often looking for two things: proof you’re not imagining it, and a plan that doesn’t treat you like a spreadsheet. You’re in the right place.
For: people juggling multiple meds or chronic conditions
If there’s a pill organizer involved, the story tends to have extra chapters. Vision changes and medications can interact through dryness, blood pressure changes, glucose variation, and side effects. A medication review can be surprisingly relevant (and if dizziness or blur shows up after a med change, document it and consider reading blood pressure medication dizziness and blurry vision as a “questions to ask” primer).
Not for: emergency symptoms that need same-day care (see “When to seek help”)
Some symptoms shouldn’t wait for a blog post to finish loading. If you suspect something urgent, skip ahead to the red flags section and act on it.
Not for: replacing an eye exam or changing meds on your own
Please don’t self-adjust medications because “maybe it’s the pills.” The safe move is to document symptoms and talk to your clinician or pharmacist with that information (especially for higher-risk situations like OTC medications to avoid with narrow-angle risk).
Quote-Prep List: What to gather before you schedule (saves time and back-and-forth)
- Insurance card + plan type (or note “self-pay”)
- Current glasses/contact prescription (if you have it)
- Medication + supplement list (include OTC sleep/allergy aids)
- Symptom start window (e.g., “mid-January,” “after a fall,” “after new meds”)
- Top 2 daily-life problems (stairs, driving, reading, faces, screens)
Neutral next step: Put these in a single note on your phone or a one-page printout before calling (a one-page medication list is often the highest-impact “first page” to bring).
6) Common mistakes: the delays that show up in almost every story
Mistake #1: waiting for it to be “constant” before booking an exam
People wait because symptoms come and go. They think, “If it were real, it would be constant.” But fluctuating symptoms can still be meaningful. The better rule: if it changes what you do (driving, stairs, reading, medication management), it deserves evaluation.
Mistake #2: updating glasses again and again without a full eye workup
New glasses can help, but if you keep chasing clarity and not catching it, you might be treating the instrument while ignoring the orchestra. More prescriptions do not equal more answers.
Mistake #3: hiding symptoms to avoid “being a burden”
I have heard this in so many senior vision decline stories it could be a refrain: “I didn’t want my kids to worry.” The tragedy is that silence often creates the exact burden you were trying to avoid.
Mistake #4: skipping medication review when vision changes start
Vision can be influenced by dryness, blood sugar variability, blood pressure changes, and medication side effects. Even if medication isn’t the cause, the list helps clinicians rule things in or out faster (and when steroids are in the mix, it’s worth asking directly about steroid-related glaucoma risk rather than hoping it’s irrelevant).
Open loop: The simple log that makes appointments faster and safer
It’s a 7-day log. Not a novel. Just enough signal to shorten the guessing.
Show me the nerdy details
Clinicians triage faster when you provide: onset window, triggers, and functional impact. A short log reduces “recall bias” (we remember the worst day) and helps identify patterns like glare-driven reduction, fatigue thresholds, or positional changes.
7) Don’t do this: risky workarounds that quietly raise fall and driving risk
“I just use the flashlight on my phone” (glare traps + shadows)
Phone flashlights are bright, harsh, and prone to creating shadows. They can help you find a dropped key, but using them as daily reading support can increase glare and make the room feel more confusing. A diffuse lamp, positioned well, usually beats a pocket spotlight.
Driving anyway because daytime feels fine (night vision isn’t daytime vision)
One senior told me, “I’m careful.” But careful doesn’t fix glare recovery time. If night driving feels like a guessing game, treat it as a safety decision, not a willpower test (and if this has been creeping up over months, compare your experience to night driving after 70 so you can describe the pattern clearly at your visit).
Buying stronger readers without checking for cataracts/AMD/glaucoma
Readers can help near tasks, but they won’t address glare, distortion, or field loss. Stronger readers can also create a false sense of “solved,” delaying the right evaluation.
Ignoring double vision or new distortion (this one deserves urgency)
If straight lines look wavy, if one eye suddenly sees a “missing spot,” or if double vision appears new, that’s not a “wait and see” situation. It’s a “call and triage” situation.
- Avoid harsh phone-flashlight glare as a long-term solution
- Night driving difficulty is a safety signal, not a personality flaw
- New distortion or double vision deserves prompt triage
Apply in 60 seconds: Pick one risky workaround you’re using and replace it with a safer alternative today.
8) When to seek help: red flags that shouldn’t wait
Sudden vision loss, curtain/shadow, new flashes/floaters
If vision changes suddenly, especially in one eye, or you notice a curtain-like shadow, a sudden increase in floaters, or flashing lights, treat it as urgent. The right move is not to “see if it settles.” The right move is to call for triage the same day.
Eye pain, severe headache, nausea, new halos with pain
Severe pain plus vision symptoms, especially with headache or nausea, deserves urgent evaluation. Pain changes the urgency category.
Sudden distortion (straight lines bending), new blind spot
New distortion can be a red-flag pattern. If a calendar grid, door frame, or page lines bend, don’t normalize it.
After a fall or head impact plus vision change
After a fall, even a “small” one, a new vision change should be mentioned promptly. The timeline matters here.
What to say on the phone to get triaged correctly (scripts)
Script 1 (urgent pattern): “I have a sudden vision change that started today. It’s in my right/left eye. I’m seeing a shadow/curtain or new flashes/floaters. I need to know if I should be seen today.”
Script 2 (function + safety pattern): “My vision has changed over the last few weeks and it’s affecting stairs/driving/reading. I have a list of symptoms and triggers. What’s the soonest appropriate appointment?”
Script 3 (caregiver calling): “I’m calling for my parent. They’re having new vision issues and I’m concerned about safety. Can you help us triage whether this is urgent?”
Infographic: Vision-Change Triage Map (printable-style)
- Sudden loss or “curtain”
- New flashes/floaters surge
- Severe pain + nausea/headache
- New distortion or blind spot
- Night driving glare worsening
- Stairs/curbs less predictable
- Faces harder to recognize
- Reading fatigue thresholds
- Dryness that improves with rest/blinks
- Screen-related blur that eases away (see digital eye strain in seniors)
- Glare helped by reducing reflections
- Symptoms stable and mild
This map isn’t a diagnosis. It’s a safety-first way to choose your next call.
9) Bring signal, not stress: the 10-minute prep that transforms the eye visit
A one-page “vision change sheet” (symptoms, timing, triggers)
I’ve watched a good appointment turn into a great one when someone walks in with a simple sheet. Not perfect. Just clear. The clinician gets signal, you get taken seriously, and the visit becomes less of a guessing game.
Include:
- When it started (rough is fine: “early February,” “after new medication,” “after fall”)
- Is it constant or episodic?
- Top 2 hardest tasks (stairs, labels, faces, screens, driving)
- Triggers (glare, dim light, fatigue, screens)
The “daily-life test”: 5 tasks to note (stairs, labels, faces, screens, night)
Pick five tasks you actually do. Not “reading a newspaper,” if you never read one. Real life is better data. I’ve used: medication labels, stair edges, TV captions, phone brightness comfort, and nighttime reflections (if labels are a recurring friction point, explore practical options like large print prescription labels).
Medication + supplement list (including OTC sleep/allergy meds)
Write it down. Bring it. Include over-the-counter items. Many seniors don’t consider sleep aids “medications,” but clinicians do, because side effects can matter (if you want the simplest version, start with a one-page medication list template and update it once a month).
Pattern-interrupt: Let’s be honest… memory gets stage fright in clinic rooms
You can remember your wedding song and forget the symptom timeline the moment someone asks, “So when did it start?” That’s not failure. That’s biology. Notes beat heroics.
Mini Calculator: Appointment Readiness (takes 20 seconds)
Choose a value for each input. This doesn’t store anything. It simply helps you see what’s missing.
Result: 0 / 11
Add one data point to make the visit smoother.
Neutral next step: If your score is under 7, spend 10 minutes on the one-page sheet before the appointment.
10) Questions to ask: how to advocate without sounding dramatic
“What diagnosis fits my symptoms best and what are the alternatives?”
This question is calm, structured, and hard to dismiss. It signals you’re not looking for a label, you’re looking for reasoning.
“What’s the plan if this gets worse in 30–90 days?”
Timelines turn vague reassurance into actual planning. If you’re time-poor, this is a high-leverage question.
“What should make me call you sooner?”
This invites the clinician to give you red-flag boundaries. You leave with a safety net.
“Can you explain my results in daily-life terms (driving, falls, reading)?”
I love this one because it’s honest. You don’t live in test results. You live in hallways, parking lots, and grocery aisles.
- Ask for the “best fit” and alternatives
- Ask for a 30–90 day plan, not vague reassurance
- Ask what should trigger an earlier call
Apply in 60 seconds: Pick two questions and write them at the top of your one-page sheet.
11) Next step: one concrete action you can do today
Start a 7-day Vision & Safety Log (template bullets)
Here’s the template. Keep it short. You’re collecting signal, not writing memoir (save that for later, if you want). The goal is to reduce dangerous delays.
- Date: ___
- Hardest task today: stairs / labels / faces / screens / driving
- When it was worse: morning / night / bright light / dim light / after screens
- What it looked like: glare / halo / softness / missing spot / wavy lines / double
- Safety moment: stumble / misread label / near-miss / avoided driving
Book an eye exam and bring the log plus medication list
Book the exam. Bring the log. Bring the medication list. If you’re caregiving, go along if you can, even if you sit quietly. Two sets of ears catch more truth.
One of the most tender moments I’ve seen: a parent saying, “I didn’t want to worry you,” and the adult child responding, “I’d rather be worried early than surprised late.” That’s not drama. That’s love with a schedule.
If you’re a caregiver: do a quick home “trip hazard + lighting” sweep
In 15 minutes: clear cords, improve stair lighting, add contrast tape if needed, and make sure the most-used pathways aren’t booby-trapped by throw rugs. You’re not redesigning the home. You’re reducing fall risk while the medical picture gets clarified (a detailed room-by-room checklist like aging vision fall prevention at home can make this fast and systematic).

FAQ
Is it normal for vision to change suddenly with age?
Some changes happen gradually with age, but sudden changes deserve triage. If it’s new, fast, or one-sided, treat it as urgent until a clinician tells you otherwise.
Why is night driving harder even with new glasses?
Because night driving depends on glare recovery and contrast, not just “sharpness.” Many people can read the chart and still struggle with headlights, reflections, and adaptation to darkness.
Can cataracts cause glare and halos around lights?
Yes, cataract-related glare and halo complaints are common in real stories, especially with night driving. But other issues can also cause halos, so it’s worth getting evaluated rather than guessing.
What does wavy or distorted vision mean?
New distortion, like straight lines bending, should be triaged promptly. It can be a red-flag pattern. Don’t wait for it to become “constant.”
How often should seniors get a dilated eye exam?
Many reputable eye-health organizations encourage regular dilated exams for older adults, but the right interval depends on risk factors (diabetes, glaucoma risk, prior eye disease). If you’re noticing changes, don’t wait for the next routine window (this guide on how often seniors should get dilated eye exams helps you pick an interval based on risk, not vibes).
Can medications cause blurry vision or dry eyes?
They can contribute, especially with multiple medications and certain OTC sleep or allergy products. The safest approach is to bring a complete list to your clinician or pharmacist and discuss it, rather than changing anything on your own (see medication-related dry eye and blurry vision after for a “what to document” checklist).
What’s the difference between macular degeneration and glaucoma symptoms?
In everyday descriptions, macular issues often show up as central blur or distortion, while glaucoma is often quiet early and may affect side vision. But symptoms overlap, and only an exam can clarify what’s happening.
When should I go to urgent care vs schedule an eye doctor visit?
Sudden loss, curtain/shadow, new flashes/floaters surge, severe pain with nausea/headache, or new distortion are “call now” patterns. Gradual changes that affect function should be scheduled soon, not ignored.
Can dry eye really make vision fluctuate day to day?
Yes. Dry eye can cause blur that changes with blinking, screen use, wind, and fatigue. The key is documenting the pattern so your clinician can distinguish discomfort from risk.
What are low-vision aids that actually help at home?
People often get meaningful wins from better contrast (labels, stair edges), targeted task lighting, larger print settings on devices, and simple magnification tools. The best aid is the one that reduces strain without adding glare (and if meds are part of the daily routine, low vision medication management is a solid place to start).
Conclusion: Close the loop, keep the plan
Remember the hook: the “lighting issue” that turned out not to be lighting at all. The truth is, many seniors don’t notice vision decline as a single dramatic event. They notice it as a string of small negotiations: with stairs, with glare, with faces, with fatigue. That’s why real-life senior vision changes warning signs stories matter. They help you name the pattern before the pattern names you.
Your next step doesn’t need to be heroic. In the next 15 minutes, start a 7-day log, write your top two daily-life problems, and list medications and supplements. Then schedule the right appointment or urgent triage if red flags are present. The goal is simple: bring signal, not stress, so you get answers faster and stay safer in the meantime (and if nighttime bathroom trips are part of the fall-risk story, consider a small upgrade like low-vision nighttime bathroom safety while you’re scheduling care).
Last reviewed: 2026-02.