


Navigating Visual Snow & Static in Later Life:
A Guide to Clarity and Care
A new visual disturbance in later life can turn an ordinary room into a flickering weather map: dots, glare, afterimages, and “static” that no one else can see.
This guide helps you slow the panic without dismissing the risk. Learn to describe symptoms clearly, track vital changes, adjust home lighting, and support your loved ones without the stress of constant interrogation.
Start with caution. Build comfort. Let coping become a bridge to better care.
Table of Contents
Safety note: This article is for general education and daily-life coping support, not diagnosis or treatment. Visual snow syndrome should be diagnosed by qualified clinicians after other causes are considered, especially when symptoms begin later in life, worsen suddenly, affect one eye, or appear with neurologic warning signs.
The goal is careful language: support function, reduce distress, and avoid false reassurance.
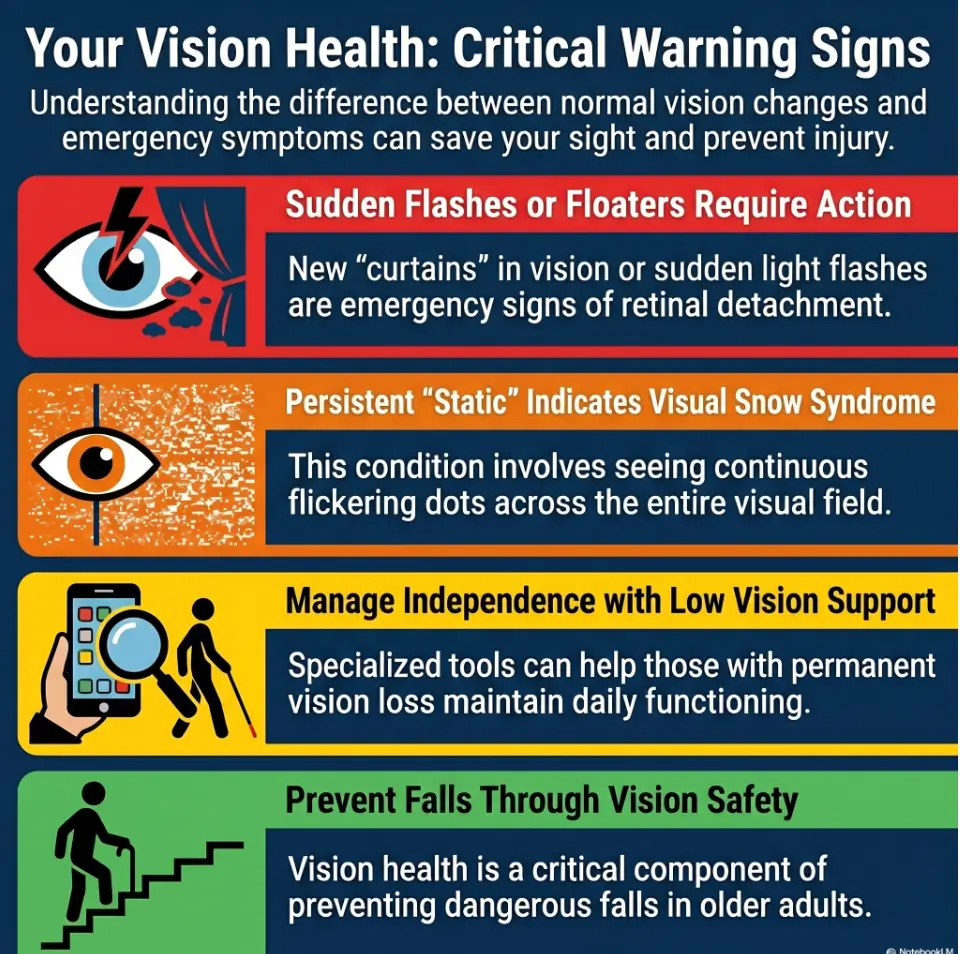
Start Here: Visual Snow in Older Adults Is Not a “Just Ignore It” Symptom
People often use “visual snow” to describe tiny dots, static, shimmering grain, afterimages, glare sensitivity, or a sense that the visual world has become noisy. It can be frightening because it is hard to explain. A knee hurts in a familiar way. A room covered in invisible confetti feels harder to defend at a doctor’s office.
The American Academy of Ophthalmology describes visual snow syndrome as persistent visual static that may come with symptoms such as palinopsia, light sensitivity, night vision trouble, or other visual disturbances. But in older adults, the safer frame is not “I have visual snow.” It is: “I have visual snow-like symptoms that need evaluation.”
What people usually mean by “visual snow”
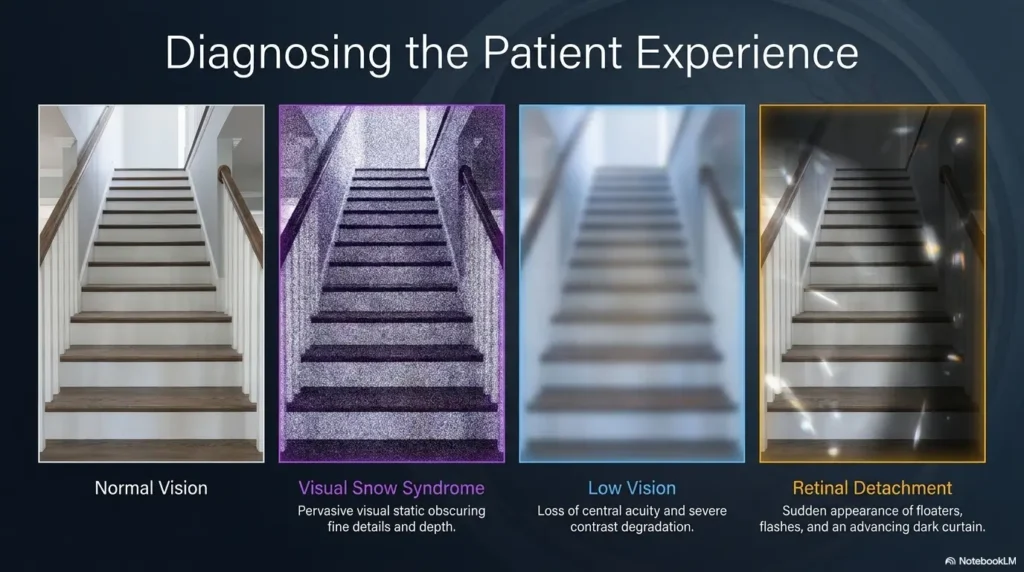
Many people mean a constant field of tiny moving dots across both eyes. Others mean “sparkle,” “grain,” “TV static,” or a faint flicker that becomes more obvious against a blank wall, white screen, dim hallway, or night sky.
That language matters. “Static everywhere all the time” is not the same as new floaters, flashes, a curtain-like shadow, blurry vision in one eye, or glare from cataracts. Those details can point clinicians in different directions.
Why older adults need a wider safety lens
Older adults have a higher chance of eye conditions that can affect vision, including cataracts, glaucoma, age-related macular degeneration, diabetic eye disease, and retinal problems. The National Eye Institute explains that low vision is more common in older adults because many causes of low vision become more common with age, not because aging itself automatically ruins vision.
So the first job is not bravery. It is sorting. The kitchen drawer of symptoms needs dividers.
The careful wording: “possible visual snow-like symptoms,” not self-diagnosis
When talking to a clinician, try saying: “I am seeing persistent static or visual noise, and I want to understand what must be ruled out first.” That sentence does two useful things. It names your experience without locking the diagnosis. It also invites the clinician to think broadly.
- Describe what you see without self-diagnosing.
- Separate static from flashes, floaters, shadows, and one-eye changes.
- Start with evaluation, then build coping strategies.
Apply in 60 seconds: Write one sentence that begins, “What I see looks like…” and bring it to your appointment.
First Rule: Rule Out the Scary Stuff Before Building a Coping Routine
Coping tips are useful only when they do not become a velvet curtain hiding an urgent problem. If a visual symptom is new, sudden, one-sided, painful, or paired with neurologic changes, do not file it under “annoying.” File it under “needs help.”
I have watched families spend 30 minutes adjusting lamps while the real issue was that nobody had asked when the symptom started. Timing is not a minor detail. Timing is the hinge on the door.
Sudden vision changes are different from long-standing static
Long-standing, stable visual static that has already been evaluated is different from a sudden burst of floaters, flashes, missing vision, or a dark curtain. Mayo Clinic lists sudden floaters, flashes, blurred vision, worsening side vision, and a curtain-like shadow as symptoms associated with retinal detachment, which is considered an emergency.
That does not mean every floater is a disaster. It means sudden changes deserve professional attention, not a late-night search spiral and a heroic cup of tea.
One-eye symptoms deserve extra caution
Visual snow syndrome is often described as affecting the visual field broadly, usually not just one eye. A symptom that clearly affects only one eye may suggest an eye-specific issue. Cover one eye, then the other, only if you can do this safely and calmly. Do not test while driving, walking stairs, or handling hot pans.
When visual snow-like symptoms overlap with migraine, retina issues, medication effects, or neurologic concerns
Migraine aura, medication side effects, retinal disease, optic nerve problems, neurologic conditions, and anxiety-driven hypervigilance can all complicate the picture. Some overlap is real. Some is misleading. That is why a careful history beats a confident label.
Decision Card: Watchful Tracking vs. Prompt Care
| Situation | Safer next step |
|---|---|
| Stable visual static already evaluated by an eye or neuro-ophthalmology clinician | Track triggers and build coping supports |
| New flashes, many new floaters, shadow, curtain, or sudden vision loss | Seek urgent medical or eye care |
| Visual symptoms with weakness, speech trouble, confusion, severe headache, or dizziness | Treat as urgent and get immediate help |
Neutral action: Put symptom timing at the top of your notes before comparing coping tools.
Who This Is For, and Who This Is Not For
This guide is for the person who has persistent visual static or visual snow-like symptoms and wants practical ways to live more steadily while pursuing appropriate care. It is also for the adult child, spouse, neighbor, or caregiver trying to help without turning into a clipboard with shoes.
It is not for sudden vision loss, new severe headache, eye pain, stroke-like symptoms, injury-related changes, or a new one-eye disturbance. Those deserve medical attention, not home optimization.
This is for older adults with persistent, already-evaluated visual static
If a clinician has already examined your eyes and considered other causes, coping strategies can help reduce daily friction. They may not erase the static. But they can make reading, moving around the house, watching screens, and sleeping feel less like a negotiation with a swarm.
This is for caregivers trying to reduce daily friction without overstepping
A caregiver’s job is not to cross-examine. It is to notice patterns. Did the person stop reading at night? Avoid the grocery store? Turn off too many lights? Stop using stairs after dinner? Those changes can reveal how symptoms are shaping the day.
For family members who want to help without taking over, a gentle guide to offering help to someone with low vision can make support feel less like supervision and more like partnership.
This is not for sudden vision loss, stroke-like symptoms, new severe headache, or eye pain
If symptoms are abrupt, intense, or paired with neurologic warning signs, the priority is urgent evaluation. Coping tips can wait. Vision is too precious to gamble with a search result and a dim lamp.
The Symptom Map: What to Track Before the Appointment
A good symptom note can save a visit from becoming fog soup. You do not need a medical degree. You need ordinary details, collected honestly.
When my own family has prepared for appointments, the most useful note was rarely poetic. It was a blunt little list: when it started, what changed, what made it worse, what felt dangerous. Not glamorous. Extremely helpful.
Static, afterimages, glare, floaters, flashes: don’t lump them together
Use separate words for separate experiences. “Static” may mean tiny dots. “Afterimages” may mean an object remains visible after looking away. “Floaters” drift. “Flashes” may appear like sparks or lightning. “Glare” may come from light scatter, shiny surfaces, or screen contrast.
One phrase, “my vision is weird,” makes everyone work harder. Four specific phrases can move the appointment forward.
Time of day, lighting, screens, fatigue, and medication timing
Track symptoms for 7 days if symptoms are stable and non-urgent. Note morning, afternoon, evening, screens, fluorescent lighting, driving, stress, sleep quality, caffeine, migraine symptoms, and medication changes. Do not change medications on your own. Just record.
If keeping scattered notes feels unrealistic, a printable symptom diary for seniors can turn those small daily observations into something a clinician can scan quickly.
Let’s be honest: “It happens sometimes” is not enough detail
“Sometimes” is a drawer where useful facts go to nap. Try this instead:
- When: “Most noticeable after dinner and on white screens.”
- Where: “Worse in the bathroom mirror and bright grocery aisles.”
- How long: “Constant background static for 3 weeks.”
- One eye or both: “Seems present with either eye open.”
- Function: “Reading labels and night walking feel harder.”
Quote-Prep List: What to Gather Before Comparing Care Options
- Current glasses or contact prescription, if available
- Medication and supplement list, including recent changes
- Eye history: cataracts, glaucoma, retina problems, diabetes, surgery
- Migraine history, tinnitus, dizziness, sleep disruption, anxiety symptoms
- One week of symptom timing and function notes
Neutral action: Keep the list to one page so it actually gets read.
Lighting Fixes: Lower the Visual Noise Without Turning the House Into a Cave
Lighting is where many coping plans either become helpful or go feral. Too much glare can make visual noise feel louder. Too little light can raise fall risk, strain reading, and make hallways feel like stage sets from a haunted theater.
The goal is not darkness. The goal is predictable, gentle, layered light.
Use steady, layered lighting instead of harsh contrast
Try combining soft overhead light, task lighting, and small guide lights. The room should not jump from cave to interrogation chamber. A shaded lamp near a reading chair may help more than blasting the ceiling fixture like opening night at a stadium.
For reading chairs and bedside tables, the angle matters as much as the bulb. A dedicated guide to reading lamp position for central vision loss can help families think in terms of task lighting rather than simply making the whole room brighter.
Reduce glare on floors, counters, mirrors, and screens
Glare is not only about bulbs. It bounces from glossy floors, polished counters, mirrors, TV screens, and tablet glass. Move lamps slightly off-axis. Use matte placemats or non-glossy surfaces where possible. Tilt screens away from window reflections.
If the bathroom is the worst offender, practical fixes for bathroom mirror glare may help reduce that harsh face-level flash that makes morning routines feel visually louder than they need to be.
Night lighting should guide, not dazzle
Night lights should mark the path from bed to bathroom without shining directly into the eyes. Older adults may already be navigating balance changes, medications, or sleepiness. A tiny light placed well can be more useful than a bright one placed like a lighthouse in the face.
For people who find white night lights too sharp, comparing red vs. amber night light options can make the bedroom-to-bathroom path easier to test without turning the hallway into a miniature runway.
Infographic: The 3-Layer Lighting Stack
①
Ambient light
Soft room light that prevents harsh dark-to-bright jumps.
②
Task light
Focused light for reading, cooking, medicine labels, and bills.
③
Path light
Low, steady guidance for night routes without eye-level glare.
Best first test: Adjust one room for 3 evenings before changing the whole house.
- Layer light to reduce harsh contrast.
- Move lamps to reduce glare, not just increase bulbs.
- Keep nighttime paths visible without dazzling the eyes.
Apply in 60 seconds: Stand at the bedroom doorway tonight and check whether the bathroom path is visible without direct glare.
Screen Strategy: Make Devices Less Like Tiny Weather Systems
Screens can turn visual snow-like symptoms into a tiny weather report: static with a chance of eye strain. But the answer is not always “make the screen dimmer.” A dim screen in a bright room can make the eyes work harder.
Start with fit, not force.
Increase text size before increasing brightness
Larger text can reduce squinting and scanning effort. On phones, tablets, and computers, increase font size first. Then adjust brightness. Many people do this backward, creating a glowing rectangle that still contains microscopic text. That is not accessibility. That is a tiny punishment machine.
For iPhone users, the built-in Magnifier can become part of a practical reading routine, especially when paired with iPhone Magnifier filters for pill bottles or other high-detail labels.
Try contrast settings, reader mode, and reduced motion
Reader mode can remove visual clutter. Reduced motion settings can limit animations. High-contrast settings help some users and bother others, so test them for 10 minutes, not 10 seconds. Your eyes deserve a trial period, not a courtroom verdict.
If bright white screens feel harsh even at night, it may help to understand the difference between Reduce White Point vs. Night Shift before changing every display setting at once.
Here’s what no one tells you: a dim screen in a bright room can be worse
Match screen brightness to room lighting. Avoid bright windows behind the screen or reflected across it. Try placing the screen perpendicular to a window. Clean the screen, too. Dust plus glare plus static is a three-piece band nobody booked.
Show me the nerdy details
Screen discomfort often comes from a mix of luminance contrast, text size, motion, glare, viewing distance, and fatigue. A useful test is to change only one variable at a time for a full reading session. If you enlarge text and symptoms improve without changing brightness, the issue may be visual effort rather than light intensity alone.
Mini Calculator: The 3-Setting Screen Test
Use this quick score after a 15-minute reading session.
- Add 1 point if text felt too small.
- Add 1 point if glare or reflections were obvious.
- Add 1 point if motion, pop-ups, or busy pages made symptoms feel louder.
Score 0–1: Keep settings and monitor patterns.
Score 2–3: Adjust text size, glare, and motion before buying filters.
Neutral action: Test settings on one device before changing every screen in the house.
Tinted Lenses and Filters: Helpful Tool, Not Magic Glass
Tinted lenses can be tempting because they promise a physical answer to a ghostly symptom. And sometimes, tinted or precision filters may help certain people feel less bothered by light sensitivity or visual discomfort. But buying lens after lens without guidance can become expensive theater.
A clinician familiar with visual symptoms, migraine, low vision, or neuro-ophthalmology can help you ask better questions before your drawer becomes a museum of almost-helpful glasses.
Why some people explore precision tints or migraine-style lenses
Some people with visual snow-like symptoms also report photophobia or migraine-related light sensitivity. FL-41 style tinting and precision filters are sometimes discussed in migraine and visual discomfort contexts. The key word is “sometimes.” Bodies are specific. Marketing is loud.
Avoid buying five pairs before asking the right clinician
Before spending money, ask: Is my symptom pattern consistent with visual snow syndrome? Are there eye conditions that could explain glare? Do I need a refraction update? Are cataracts or dry eye contributing? Would low-vision rehabilitation strategies help?
The indoor sunglasses trap: comfort today, light sensitivity tomorrow?
Wearing dark sunglasses indoors all day may feel soothing, but it can make normal indoor lighting feel harsher over time for some people. It may also reduce contrast and increase fall risk. In older adults, “comfortable” and “safe for movement” must sit at the same table.
- Ask about eye causes of glare first.
- Test lenses in real tasks: reading, walking, cooking, shopping.
- Avoid making the whole day darker without clinician input.
Apply in 60 seconds: Write down the 2 tasks where light bothers you most before shopping for lenses.
Migraine, Tinnitus, Anxiety, and Sleep: The Symptom Cluster Nobody Should Shame
Visual snow syndrome can travel with other sensory burdens, including migraine, tinnitus, light sensitivity, and anxiety. That does not mean the symptom is imaginary. It means the nervous system may be carrying a louder-than-usual orchestra, and every instrument wants a solo.
Shame is useless here. Tracking is useful. Care is useful. Sleep is very useful, though annoyingly hard to improve when your vision is throwing confetti at bedtime.
Visual snow syndrome often travels with other sensory burdens
Some people describe visual static alongside ringing in the ears, headache patterns, dizziness, or sensitivity to light. If this is true for you, mention the whole cluster. A clinician cannot connect dots you keep politely hidden in separate pockets.
Sleep disruption can make coping feel harder
Poor sleep can make nearly any persistent symptom feel sharper. It can reduce patience, increase anxiety, and make screen or light sensitivity harder to tolerate. The first goal is not perfect sleep. It is a repeatable wind-down routine that does not involve doom-scrolling symptoms at midnight.
If screen brightness is part of the bedtime battle, a guide to making an iPhone screen dimmer than the minimum setting may help reduce visual load without turning the room completely dark.
Stress management is not “it’s all in your head”
Stress management is not a dismissal. It is symptom load management. Breathing exercises, gentle movement, therapy, migraine-aware routines, and predictable meals may not cure visual snow-like symptoms. But they can reduce the daily volume.
Coverage Tier Map: From Basic Coping to Specialist Support
| Tier | What changes |
|---|---|
| Tier 1 | Symptom tracking, safer lighting, screen adjustments |
| Tier 2 | Routine eye exam and medication review |
| Tier 3 | Migraine, sleep, tinnitus, or anxiety support as relevant |
| Tier 4 | Neuro-ophthalmology or retina evaluation when indicated |
| Tier 5 | Low-vision rehabilitation, occupational therapy, or home safety review |
Neutral action: Start at the lowest safe tier, but move up quickly when red flags or function loss appear.
Common Mistakes: Don’t Let Coping Become Avoidance
Coping is meant to widen life, not shrink it. The danger is subtle. First you dim the lights. Then you stop driving at dusk. Then you stop reading medicine labels unless someone is nearby. Then the house becomes smaller, not safer.
The aim is not fearless independence. It is designed independence.
Mistake 1: assuming every visual symptom is visual snow
Floaters, flashes, glare, double vision, blurry patches, and missing side vision are not interchangeable. The words may sound small, but the consequences can be large.
For a wider safety frame, it may help to review senior vision changes warning signs so “visual snow-like” symptoms are not accidentally used as a basket for every new visual change.
Mistake 2: waiting months because the symptom is “only annoying”
Annoying symptoms can still affect driving, medication use, cooking, walking, and sleep. If a symptom changes behavior, it deserves attention. “Only annoying” has fooled many sensible people.
Mistake 3: over-darkening the home and increasing fall risk
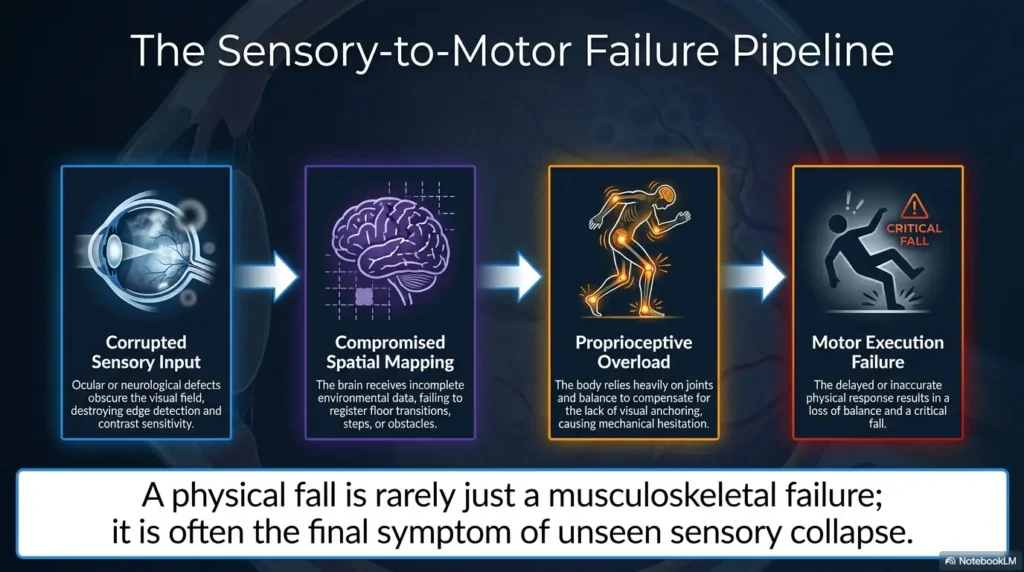
A dark home can reduce visual discomfort while quietly increasing trip risk. The CDC’s STEADI fall-prevention work emphasizes identifying modifiable fall risks. For older adults, lighting, clutter, stairs, rugs, medications, and balance all matter. Visual comfort should never come at the price of safe movement.
A broader aging vision fall prevention at home approach can help families balance comfort, contrast, lighting, and safe pathways instead of fixing one symptom while creating another risk.
Mistake 4: changing medications or supplements without medical guidance
If symptoms appeared after a medication change, tell the prescribing clinician. Do not stop or adjust medication on your own unless you have been specifically instructed to do so. A symptom note is safer than improvising with a pill bottle.
When several prescriptions are involved, a simple one-page medication list template can make the medication story easier to bring into the appointment without relying on memory.
- Do not label every visual change as visual snow.
- Do not darken rooms so much that walking becomes risky.
- Do not change medications without clinician guidance.
Apply in 60 seconds: Name one activity you have started avoiding and write it on your symptom snapshot.
Home Safety: Protect Vision, Balance, and Confidence Together
Home safety is where coping becomes practical. Not dramatic. Not cinematic. More like moving one rug, adding one light, labeling one switch, and preventing a bad Tuesday.
Visual snow-like symptoms may not directly cause falls, but glare, clutter, poor contrast, fatigue, night walking, and medication effects can combine in unpleasant ways. The quiet danger is not one villain. It is the committee.
Keep walking paths visually simple and physically clear
Clear the main path from bed to bathroom, bedroom to kitchen, and favorite chair to front door. Remove loose cords. Reduce floor clutter. Avoid patterned rugs in routes where visual noise already feels high. A floor should not look like a puzzle when someone is sleepy.
When walking feels visually busy, low vision walking guidance can help caregivers and older adults focus on path clarity, pace, and orientation instead of relying on vague reminders to “be careful.”
Add contrast where it helps: stairs, thresholds, switches, bathroom edges
Contrast tape on stair edges, easy-to-see switch plates, and non-slip bathroom cues can help orientation. Keep contrast purposeful. Too many labels and stripes can become visual confetti, which is exactly what we are not trying to manufacture.
In the bathroom, small contrast decisions can be surprisingly functional. For example, choosing a toilet seat contrast color may support orientation without adding clutter to an already visually demanding room.
The quiet danger: glare plus clutter plus night bathroom trips
Night bathroom trips deserve special respect. Sleepiness, low light, medication effects, and urgency can turn a familiar hallway into a tiny obstacle course. Fix this route first. It is high-frequency, high-stakes, and often ignored because nobody wants to discuss bathroom logistics over coffee.
Short Story: The Hallway That Changed the Week
A caregiver once told me her father insisted the house was “fine.” He was not falling. He was not complaining. But he had stopped drinking water after dinner because the bathroom trip felt visually chaotic: shiny floor, dark hallway, bright bathroom mirror, bath mat curled at one corner. The solution was almost embarrassingly ordinary.
A low night light went near the baseboard. The bath mat was replaced. A mirror-facing bulb was softened. A small basket stopped toiletries from scattering across the counter. Nothing cured his visual symptoms. But within a week, he stopped rationing water like a desert traveler guarding a canteen. That is what good coping often looks like: not a miracle, just one less daily negotiation with fear.
For a deeper room-by-room setup, low vision nighttime bathroom safety is one of the most useful places to start because the route is repeated, sleepy, and easy to underestimate.
Caregiver Script: How to Ask Without Sounding Like a Domestic Detective
Caregivers often ask, “Are you okay?” Older adults often answer, “I’m fine.” Then everyone stands in the kitchen holding a useless sentence.
Better questions are smaller, kinder, and more functional. They do not demand confession. They invite useful detail.
Ask what changed, not whether they are “fine”
Try: “What feels harder this week than last week?” Or: “Is the static worse in any room?” Or: “Do screens, stores, or night walking feel different?” These questions are harder to brush away and easier to answer honestly.
If the person resists help because it feels embarrassing or intrusive, the language in helping a spouse with vision loss can be adapted for adult children, neighbors, and friends too.
Use function questions: reading, cooking, stairs, driving, sleep
Function questions reveal the real cost of symptoms. Ask about reading mail, cooking, stairs, showering, medication labels, driving at dusk, grocery aisles, and sleep. If a person has stopped doing 2 or 3 ordinary tasks, the symptom burden is not small.
Build a shared symptom note before the visit
A caregiver can help write the one-page symptom snapshot, but the older adult should keep control of the language when possible. Dignity is not decorative. It is part of care.
Eligibility Checklist: Does This Need More Than Home Tweaks?
- Yes/No: Did the symptom begin suddenly?
- Yes/No: Is it clearly worse in one eye?
- Yes/No: Are there flashes, many new floaters, shadows, or pain?
- Yes/No: Has driving, medication use, cooking, stairs, or sleep changed?
- Yes/No: Did it start after a medication change or injury?
Neutral action: Any “yes” answer should be written down and discussed with an appropriate clinician.
When to Seek Help: Red Flags That Should Not Wait
This is the section to save, print, or send to the family group chat where everyone uses too many thumbs-up emojis. Red flags are not meant to scare you. They are meant to prevent delay.
Sudden vision loss, curtain-like shadow, new flashes, or many new floaters
Seek urgent care if there is sudden vision loss, a curtain-like shadow, new flashes, or many new floaters. These symptoms can be associated with retinal problems that need prompt evaluation.
New weakness, numbness, confusion, speech trouble, dizziness, or severe headache
Visual symptoms plus neurologic changes should be treated seriously. Weakness, numbness, confusion, trouble speaking, severe dizziness, or a new severe headache should not be managed with lamp adjustments and optimism.
Eye pain, jaw pain, scalp tenderness, or new symptoms after injury
Eye pain, injury-related symptoms, jaw pain, scalp tenderness, or new headache in an older adult can point to concerns that need medical review. Do not downplay pain because the visual symptom is hard to describe.
New visual symptoms after medication changes
Bring a medication list and the timing of changes. Include prescription drugs, over-the-counter medicines, sleep aids, supplements, and eye drops. The bottle parade may feel tedious, but it can be clinically useful.
For families trying to connect medication timing with blurry vision, glare, or dizziness, polypharmacy and vision problems can help frame the question without encouraging anyone to stop medication on their own.
- Sudden changes should not be treated as routine visual snow.
- One-eye changes, shadows, flashes, or neurologic symptoms need caution.
- Medication timing belongs in the symptom story.
Apply in 60 seconds: Add “sudden or gradual?” and “one eye or both?” to the top of your notes.
FAQ
Can visual snow syndrome start in older adults?
It can be reported in adults, but new visual snow-like symptoms in older adults should be approached carefully. Later-life onset makes it especially important to rule out eye, neurologic, medication-related, migraine-related, or urgent causes before settling into a coping plan.
Is visual snow syndrome an eye disease or brain-processing issue?
Visual snow syndrome is often discussed as a visual processing condition rather than a simple eye disease. Still, an eye exam is important because eye conditions can create symptoms that people may describe as static, glare, spots, blur, or visual disturbance.
Can cataracts, glaucoma, or retina problems look like visual snow?
They may not be the same thing, but they can create visual complaints that overlap in everyday language. Cataracts may increase glare. Retina issues may create flashes, floaters, shadows, or distorted vision. Glaucoma can affect peripheral vision. The words matter because the causes and risks differ.
Are floaters the same as visual snow?
No. Floaters usually drift through vision and may look like specks, strings, or cobwebs. Visual snow is often described as persistent tiny static across the visual field. Sudden new floaters, especially with flashes or a shadow, should be evaluated promptly.
Can stress make visual snow-like symptoms feel worse?
Stress can make many persistent symptoms feel louder because attention, sleep, muscle tension, migraine patterns, and anxiety can all interact. That does not mean the symptom is fake. It means reducing stress may reduce symptom burden while medical evaluation continues.
Should older adults stop driving if they notice visual static?
If visual symptoms affect clarity, glare tolerance, night vision, reaction confidence, or attention, driving should be discussed with an eye care professional or physician. Sudden visual symptoms should be evaluated before driving. Safety beats pride every time, even when pride has excellent posture.
For a related safety lens, night driving after 70 can help families discuss glare, reaction confidence, and route choices without turning the conversation into a battle over independence.
Do tinted lenses help visual snow syndrome?
Some people explore tinted lenses or filters for light sensitivity, migraine-related discomfort, or visual strain. They are not a guaranteed fix. Older adults should be cautious with dark indoor lenses because reduced light and contrast may increase fall risk.
Is there a cure for visual snow syndrome?
The American Academy of Ophthalmology notes that there is no known cure for visual snow syndrome. Management often focuses on reducing symptom burden, treating related conditions when present, and supporting daily function through practical adjustments and clinician-guided care.
Next Step: Make a One-Page Symptom Snapshot Before You Search for Fixes
The hook at the beginning was that strange bad-TV feeling: the room tuned to static. The answer is not to pretend the static is harmless. It is to turn the static into information, then turn the information into safer decisions.
Write down what you see, when it happens, and what makes it worse
Use plain words. Draw a tiny map if helpful. Note whether symptoms are constant or episodic, one eye or both, sudden or gradual, and whether they affect reading, cooking, stairs, driving, sleep, or confidence.
Bring medication lists, eye history, migraine history, and timing notes
Bring current medications, supplements, eye drops, glasses, prior eye diagnoses, surgeries, migraine history, tinnitus notes, and recent medication changes. The more organized the story, the less likely the appointment becomes a guessing contest.
If reading labels or small print has become part of the daily friction, learning how to read labels aloud can be a practical bridge while you prepare for medical guidance and safer routines.
Ask one practical question: “What must we rule out first?”
That question is the heart of safe coping. It keeps urgency in view without panic. It tells the clinician you are not chasing a trendy label. You are trying to protect vision, function, and peace of mind.
- Keep the note to one page.
- Put red flags and timing at the top.
- Use coping tools to support life, not avoid care.
Apply in 60 seconds: Start a note titled “What must we rule out first?” and add today’s date.
Your 15-minute next step: Make the one-page symptom snapshot, check the bedroom-to-bathroom lighting path, and schedule appropriate medical or eye care if symptoms are new, changing, one-sided, or affecting daily function.
Last reviewed: 2026-05.