
Navigating the Visual Mismatch: Reading with Anisometropia
You open a book after cataract surgery expecting the page to behave, then one eye seems ready for daylight while the other is still negotiating with yesterday’s prescription.
Anisometropia after cataract surgery can make reading feel uneven, swimmy, tiring, or oddly “off,” especially between first-eye and second-eye surgery or while adjusting to monovision. The frustrating part is that your operated eye may be healing well and still not feel comfortable when both eyes try to read together.
It means your two eyes have different focusing power. After cataract surgery, this mismatch can happen when one eye has a new intraocular lens and the other still has a cataract, a different prescription, or a different near-distance target.
Common symptoms: Blur, eye strain, dizziness, depth-perception trouble, or image-size mismatch.
Keep guessing, and you may waste energy on the wrong fix: stronger readers, old glasses, dim lighting, or stubborn “just one more page” sessions. This guide helps you reduce reading strain, spot red flags, and bring better notes to your eye care professional.
Table of Contents
- One eye may now focus differently than the other.
- The page may feel clear but visually unstable.
- Temporary coping can help, but persistent symptoms deserve professional review.
Apply in 60 seconds: Open one familiar page under good light and notice whether the problem is blur, strain, dizziness, doubling, or size mismatch.
The Reading Problem Is Not “In Your Head”
Why one sharp eye can still make reading feel wrong
After cataract surgery, many people expect a simple trade: cloudy lens out, clear lens in, reading solved. Sometimes it is that tidy. Sometimes the brain receives a visual duet where one violin is tuned for near work and the other is still tuning backstage.
Anisometropia means the two eyes have meaningfully different focusing power. After cataract surgery, this can happen when one eye has been corrected and the other eye has not, or when the two eyes are intentionally set for different distances, such as with monovision. The Cleveland Clinic describes anisometropia as unequal refractive error between the eyes, and that mismatch can show up as eye strain, headaches, depth perception trouble, or blurry vision.
The frustrating part is that your operated eye may test well on the chart. You may even hear, “The surgery looks good.” Both can be true. The eye can be healing nicely while your reading system still feels like a committee meeting with no chairperson.
The difference between blur, imbalance, and image-size mismatch
Reading discomfort after cataract surgery is not one single thing. It can be blur. It can be binocular strain. It can be glare sensitivity. It can be image-size mismatch, also called aniseikonia, where the same page seems slightly larger, smaller, stretched, or spatially “off” in one eye.
That distinction matters because the fix may differ. A stronger reader may help simple near blur. It may not help if the problem is magnification difference between the two eyes. Old glasses may sharpen one eye and make the overall binocular feeling worse. The human brain is brilliant, but it is not always thrilled when handed two versions of the same paragraph.
Here’s what no one tells you: clear vision can still feel unstable
I have heard people describe this as “my eyes are arguing,” “the words swim,” or “the page feels tilted even when it is not.” Those phrases sound poetic until you are the person trying to read a medication label at 7:15 a.m. with coffee cooling beside you. If small print has become part of the daily battle, a practical guide on how to read labels aloud can help reduce guessing while your eyes are still adapting.
Clear vision is not only about sharpness. Comfortable reading also needs matching focus, steady eye teaming, enough contrast, manageable glare, and a brain that trusts what both eyes report. After cataract surgery, that trust may need time, adjustment, and sometimes a professional lens strategy.
Plain-English truth: If reading feels weird after cataract surgery, you are not being dramatic. But you also should not guess your way through persistent dizziness, double vision, or sudden changes.
Who This Is For, And Who Should Not Wait
For readers between first-eye and second-eye cataract surgery
This guide is for the person who had one cataract removed and is now living in the in-between. One eye may be brighter, clearer, and corrected by an artificial lens. The other may still be cloudy, nearsighted, farsighted, or astigmatic. Reading becomes less like a quiet task and more like negotiating a peace treaty across a kitchen table.
This in-between period can be especially odd if your first eye was set for distance and your unoperated eye still handles near tasks, or the reverse. You may feel okay walking around but uncomfortable reading. Or reading may be fine for 4 minutes, then suddenly your forehead and neck join the complaint department.
For people adjusting to monovision or unequal prescriptions
Some people choose, or are advised to try, monovision. That usually means one eye is set more for distance and the other more for near vision. Many people adapt well. Others need time. A few never love it, and that is not a character flaw. It is biology with opinions.
This article also fits people whose new glasses prescription has not settled yet, whose old glasses now feel strange, or whose over-the-counter readers help for a page or two and then turn into tiny plastic chaos.
Not for sudden vision loss, severe pain, flashes, or many new floaters
Some symptoms after cataract surgery are not “reading quirks.” The American Academy of Ophthalmology warns that vision loss, eye pain, flashing lights, or a dark curtain in the field of vision after cataract surgery should be treated as urgent. Increasing redness, strong light sensitivity, many new floaters, or swelling should also be taken seriously.
Do not try to troubleshoot those symptoms with a lamp, a larger font, or optimism wearing a cardigan. Call your surgeon’s office, use the after-hours number, or seek urgent eye care based on your discharge instructions.
When “annoying” becomes “call the eye doctor today”
There is a difference between “my eyes tire after 10 minutes of reading” and “my vision changed suddenly this afternoon.” The first may be worth tracking and discussing. The second belongs in the prompt-call category. If you tend to freeze or forget details during medical visits, a simple doctor appointment note-taking system can keep the important clues from evaporating under exam-room lights.
- Call promptly for sudden vision loss, severe pain, or worsening redness.
- Ask urgently about flashes, many new floaters, or a curtain-like shadow.
- Report persistent double vision, nausea, or imbalance.
Apply in 60 seconds: Put your surgeon’s office number and after-hours instructions in your phone before you need them.
Eligibility checklist: Is this guide the right starting point?
Use this as a comfort and communication guide if these statements fit your situation:
- Yes or no: You recently had cataract surgery in one or both eyes.
- Yes or no: Reading feels uneven, tiring, jumpy, or spatially strange.
- Yes or no: You do not have sudden vision loss, severe pain, or urgent red-flag symptoms.
- Yes or no: You are willing to ask your ophthalmologist or optometrist before changing drops, prescriptions, or contact lens use.
Neutral action: If you answered “yes” to the comfort concerns and “no” to urgent symptoms, start a short reading log and bring it to your next eye visit.
The Sneaky Cause: Your Eyes May Be Sending Two Different Books
Anisometropia: unequal focusing power between eyes
Anisometropia sounds like a word someone dropped behind a cabinet. But the idea is practical: your two eyes do not focus the same way. After cataract surgery, this may happen because one eye now has an intraocular lens, often called an IOL, while the other eye is still using its natural cataract-clouded lens.
Imagine one eye reading a large-print hardcover and the other reading a faded paperback with a bent spine. Both may be “books,” but the brain has to merge them into one reading experience. That merger can be tiring.
Aniseikonia: when the same page looks different in each eye
Aniseikonia is related but not identical. It means the image perceived by one eye differs in size or shape from the image perceived by the other eye. Cleveland Clinic notes that aniseikonia may cause headache, dizziness, double vision, eye strain, imbalance, nausea, and trouble tolerating glasses.
This can matter after cataract surgery because glasses change not only focus but also magnification. If the prescription difference between your two eyes is large, glasses may sharpen the image while making the two-eye experience feel odd. Contact lenses sometimes reduce this magnification issue because they sit directly on the eye, but they are not appropriate for everyone, especially right after surgery unless your doctor says so.
Monovision confusion: one eye near, one eye far, one brain negotiating peace
Monovision can be clever. One eye handles distance, the other helps with near work. For some people, it feels like a tidy little magic trick. For others, the trick has too many scarves and one confused rabbit.
The brain may need days or weeks to adapt. During that time, reading can feel strange even if each eye is doing its assigned job. The issue is not that the plan is automatically wrong. The issue is that your real daily life includes menus, pill bottles, phone screens, night lights, rain on windshields, and the tiny print on a frozen lasagna box that seems designed by a raccoon with a law degree.
Show me the nerdy details
Reading comfort depends on binocular fusion, accommodation demand, convergence, contrast sensitivity, glare tolerance, and image magnification. Cataract surgery changes the optical system by replacing the cloudy natural lens with an intraocular lens. If the two eyes differ in refractive power, focal target, or magnification, the brain may struggle to combine the images smoothly. This is why a person can have good single-eye clarity but still experience strain, dizziness, spatial distortion, or trouble sustaining near work.
Don’t Force It: The Reading Mistake That Backfires
Why pushing through long sessions can worsen fatigue
When reading feels uncomfortable, the first instinct is often to push harder. We squint. We hold the book closer. We tilt the head. We close one eye “just for a second,” then realize we have been reading like a suspicious pirate for 12 minutes.
That heroic approach can backfire. Eye strain is not a moral test. If your visual system is already working overtime to merge unequal images, long reading sessions may increase headache, neck tension, nausea, and frustration. A tired brain is not a better brain. It is just a tired brain wearing bifocals.
The 10-minute test: stop before your eyes start arguing
Instead of asking, “Can I force myself through this chapter?” ask, “What happens in the first 10 minutes?” That gives you useful information without turning your living room into a vision endurance arena.
Try one familiar page under good light. Read for 5 minutes. Pause. Notice symptoms. Continue to 10 minutes only if you feel steady. Stop before symptoms bloom. This is not quitting. This is collecting clean data.
Let’s be honest: “I’ll just finish this chapter” is how eye strain wins
Reading has a sneaky emotional pull. You want to finish the article, the mystery chapter, the insurance letter, or the text from your cousin who uses punctuation like confetti. But after cataract surgery, especially with anisometropia, stopping early can be the smarter move.
Give yourself permission to use audio, larger fonts, or short sessions. The goal is not to prove your eyes wrong. The goal is to let your brain adapt without turning every paragraph into a wrestling match.
Mini calculator: Your reading strain score
Use this simple 3-input check after a reading session. No app, no storage, no fancy spreadsheet goblin required.
- Blur: Rate 0 to 3, where 0 is none and 3 is strong.
- Dizziness or imbalance: Rate 0 to 3.
- Headache or eye strain: Rate 0 to 3.
Total: 0 to 2 means keep tracking. 3 to 5 means shorten sessions and mention it at your next visit. 6 to 9, or any sudden symptom, means call your eye-care team sooner.
Neutral action: Write the score next to the reading time and lighting condition.
First-Week Coping: Make Reading Smaller, Brighter, and Less Heroic
Use larger text before you use more willpower
During early healing, do not make your eyes wrestle tiny print unless there is a good reason. Increase font size on your phone, tablet, e-reader, and computer. Use large-print books if you have them. Print important instructions bigger if needed.
I once watched someone enlarge a phone screen and then sigh as if the room had opened a window. Nothing medical changed. The task simply stopped being cruel. Sometimes comfort is not a grand solution. Sometimes it is a font size with manners.
Match the page to your best working distance
After cataract surgery, your old reading distance may no longer be your best reading distance. Test a few positions. Try the page at 14 inches, 16 inches, and 18 inches if your arms and posture allow. Keep your neck relaxed. The winning distance is the one that reduces strain, not the one your pre-surgery habits remember.
If one eye was set for distance, near reading may need more help. If one eye was set for near, distance tasks may feel different. This is where patient tracking helps your doctor more than a vague “it feels weird,” although “it feels weird” is still a valid first draft.
Reduce glare without making the room cave-dark
More light is not always better. Better light is better. Use a shaded lamp aimed at the page, not your eye. Avoid harsh reflections on glossy pages. Try matte paper when printing. Use dark mode carefully because some people find it easier, while others experience more blur or halos. For a deeper home setup angle, this guide to reading lamp position for central vision loss can help you think about light direction, glare, and task comfort without turning the room into a small interrogation chamber.
Cataract surgery can make colors appear brighter because the cloudy lens has been replaced. Mayo Clinic explains that vision may be blurry at first while the eye heals and adjusts, and colors may look brighter after surgery. That brightness can feel wonderful, but it can also make glare more noticeable for a while.
Build a reading nest: chair, lamp, bookmark, drops schedule, patience
A reading nest is not indulgent. It is risk control with a softer sweater. Put your chair, lamp, water, tissues, eye-drop schedule, bookmark, and phone within easy reach. Do not read while bent sideways on the couch like a punctuation mark having a difficult day.
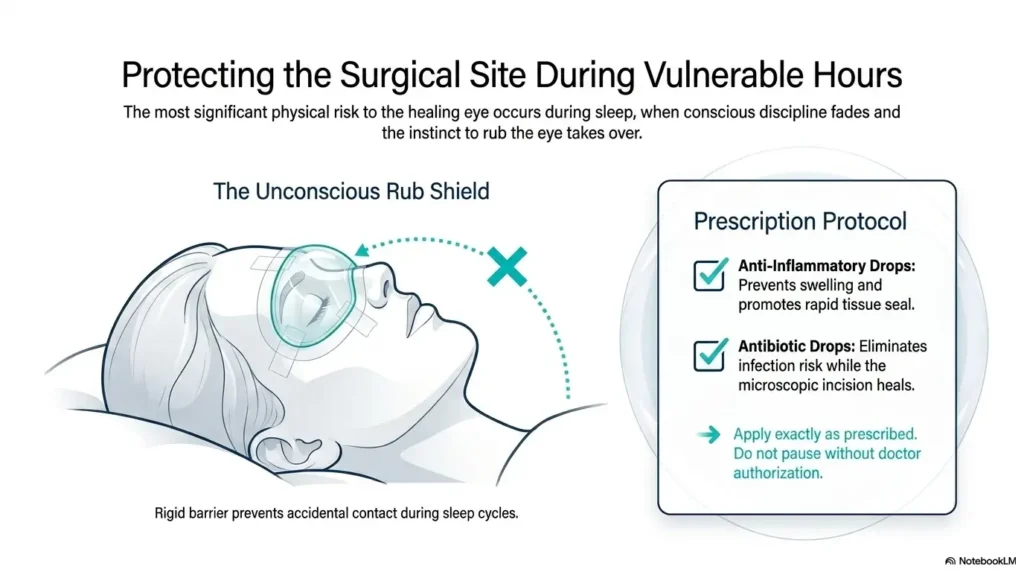
Keep post-op drops on schedule exactly as prescribed. Do not add, stop, or swap drops without your surgeon’s guidance. The eye is healing. It does not need a surprise chemistry experiment from the bathroom cabinet. If drops and supplies are starting to scatter across the nightstand, a low vision bedside organization system may help keep the essentials findable by both sight and habit.
Reading Comfort Map After Cataract Surgery
Aim lamp at the page, not the eye.
Increase font before squinting.
Test a few comfortable page positions.
Pause before strain becomes a storm.
Note blur, dizziness, doubling, or size change.
The One-Eye Test: Useful Clue, Not a DIY Diagnosis
Cover one eye briefly to describe what changes
The one-eye test is simple. While looking at a familiar page, briefly cover one eye, then the other. Do not press on the eye. Do not perform a full home eye exam. Just notice what changes.
Does the page become clearer with one eye? Does the image look larger or smaller? Does dizziness improve when one eye is covered? Does doubling disappear? These clues can help you describe the problem to your ophthalmologist or optometrist.
Notice blur, distortion, doubling, dizziness, or image-size difference
Use plain language. You do not need to arrive at your appointment sounding like a textbook with car keys. “The left eye makes the words look smaller,” “I feel dizzy after 8 minutes,” or “old glasses make the room swim” can be more useful than a dramatic but vague “my vision is broken.”
Also notice whether symptoms happen only with reading or also with walking, stairs, screens, or driving. If imbalance affects mobility, depth perception, or nausea, treat it as more than a minor reading annoyance.
Write symptoms down before your appointment so memory does not fog the lens
Post-surgery days can blur together. Drops, appointments, sleep, lights, shields, instructions, and the strange little emotional weather of healing all pile up. A short note saves you from trying to reconstruct everything under fluorescent office lighting.
Write down the date of surgery, which eye was treated, your current glasses or readers, what triggers symptoms, how long reading takes before discomfort starts, and whether covering one eye changes the problem. If you prefer a ready-made structure, a printable symptom diary for seniors can turn scattered observations into something easier to bring to an appointment.
Quote-prep list for your eye visit
Before comparing lens options, glasses timing, readers, or contact lens strategies, gather:
- Your old glasses and any current readers.
- Your eye-drop list and dosing schedule.
- Your surgery dates and which eye was done first.
- Your top 3 daily reading tasks, such as phone, books, labels, or computer.
- Your 5-minute and 10-minute symptom notes.
Neutral action: Put these items in one bag the night before your appointment.
Temporary Fixes: What May Help Before Your Prescription Settles
Over-the-counter readers: when they help and when they confuse things
Over-the-counter readers can help if the main problem is near focus and both eyes can tolerate the same magnification. They are easy to buy, easy to test, and easy to misplace in every room of the house like tiny plastic migratory birds.
But readers are blunt tools. They use the same power for both eyes. If your two eyes have very different needs after cataract surgery, a pair of drugstore readers may help one eye while confusing the other. That does not mean readers are bad. It means they are not customized.
Old glasses after cataract surgery: why they may feel strangely wrong
Old glasses may feel wrong because one eye no longer needs the same correction. If only one eye has been operated on, your old glasses may be too strong, too weak, or magnifying one side differently. Some people pop out one lens or use a temporary lens modification only after their eye-care professional recommends it. Do not start home-engineering glasses with kitchen tools. The screwdriver is not an optometrist.
Your surgeon or optometrist may suggest a temporary strategy while you wait for healing or the second surgery. That strategy depends on your prescription, IOL target, symptoms, and daily needs. If you are comparing lens choices or still trying to understand why one eye was targeted differently than the other, this plain-English guide to monofocal, multifocal, and toric IOL options may help you frame better questions.
Contact lens options: sometimes smoother for unequal eyes, but not for everyone
Contact lenses may reduce image-size differences caused by glasses because they sit on the eye rather than in front of it. That can help some anisometropia cases. But after cataract surgery, contact lens use must be cleared by your eye-care team, especially while the eye is healing.
Dry eye, infection risk, dexterity, hygiene, and medication schedules all matter. A contact lens can be elegant in theory and annoying in real life if your hands, tear film, or morning routine disagree.
Prescription timing: why the “final glasses” conversation usually needs healing time
Your eye needs time to heal and stabilize. Many surgeons wait until the eye is sufficiently healed before prescribing final glasses. The exact timing varies by patient, surgery details, and whether the second eye is scheduled soon.
Do not assume the first blurry or strange week predicts your final reading life. Early recovery is a moving target. It is less like buying furniture and more like waiting for bread dough to rise, except the bread has an appointment card and anti-inflammatory drops.
- Readers can help simple near blur but may not solve unequal-eye problems.
- Old glasses may feel wrong because one eye has changed.
- Contacts can help some people but require professional approval after surgery.
Apply in 60 seconds: Label your glasses and readers, then note which pair helps or worsens reading.
Common Mistakes That Make Reading Imbalance Worse
Mistake 1: switching between too many glasses all day
Switching among old progressives, new readers, backup readers, computer glasses, and the pair you found in a drawer can turn your visual system into a revolving door. If your brain is already adapting, too many optical changes may make symptoms harder to interpret.
Ask your eye-care team which pair to use for which task during the temporary period. Then keep notes. “Blue readers for phone, no glasses for TV, old progressives make stairs weird” is useful information.
Mistake 2: reading in dim light and blaming the surgery
Dim light forces more effort. After cataract surgery, your eye may still be adjusting to brightness, contrast, and glare. Reading in a cave-like room can make even a good surgical outcome feel disappointing.
Use steady, indirect light. Avoid reading with a bright window behind the page or a bare bulb reflecting into your eye. Good lighting is not glamorous, but neither is squinting at a soup label like it contains state secrets.
Mistake 3: ignoring dizziness because the eye chart looked fine
An eye chart measures important things, but it does not fully recreate reading on a couch, walking down stairs, or checking a phone in a grocery aisle. If you feel dizzy, nauseated, spatially off, or unsteady, say so clearly.
Persistent imbalance deserves attention, especially in older adults where falls can carry serious consequences. Your surgeon may want to rule out eye-related complications, prescription mismatch, or non-eye causes. If vision changes are also affecting how someone moves through hallways, curbs, or stairs, low vision walking guidance can offer practical language for safer movement support.
Mistake 4: assuming the second eye will behave exactly like the first
The second eye may heal differently. It may have a different cataract density, prescription, astigmatism pattern, ocular surface issue, or IOL target. Your experience with the first eye is helpful, not prophetic.
Before second-eye surgery, tell your surgeon exactly what reading tasks matter most. Books, phone, sheet music, computer work, sewing, labels, and night driving all create different demands.
Mistake 5: changing eye drops without asking the surgeon
Post-op drops are not decorative. They are prescribed to manage inflammation, infection risk, pressure concerns, or healing needs depending on your case. Skipping, doubling, stretching, or replacing them can create avoidable trouble.
If a drop stings, runs out, causes concern, or conflicts with another medication, call the office. Do not let discomfort quietly become nonadherence. The eye-care team has heard these questions before. You are not the first person to battle a tiny bottle at 6 a.m. For dry-eye comfort questions after surgery, this guide to preservative-free tears after cataract surgery may help you understand what to ask before adding anything new.
Decision card: When to rest, when to track, when to call
- Rest: Mild tiredness after reading, improves with breaks, no sudden change.
- Track: Repeated strain, dizziness, image-size difference, or readers that help only one eye.
- Call: Sudden vision loss, severe pain, worsening redness, flashes, many new floaters, curtain shadow, or persistent double vision.
Neutral action: Match your symptom to one category before deciding what to do next.
The Second-Eye Question: Why Timing Can Change the Reading Experience
Why imbalance may feel worse when only one eye has been corrected
The period between first-eye and second-eye surgery can be the most visually awkward. One eye may be bright and corrected. The other may still be cloudy or differently focused. The brain tries to combine both inputs, and sometimes it sends back a complaint written in headache ink.
This does not mean the first surgery failed. It may mean your two-eye system is temporarily out of balance. Many people feel more visually even after the second eye is corrected, but the details depend on IOL targets, healing, astigmatism, ocular surface health, and personal adaptation. For a broader planning view, see this guide on whether cataract surgery is done one eye or both eyes.
How second-eye planning may reduce mismatch
Second-eye planning is not just a repeat performance. It is a chance to discuss what happened after the first surgery. Did reading improve? Did distance vision feel strong? Did monovision feel tolerable? Did you experience dizziness, glare, halos, or trouble with stairs?
Your surgeon can use that lived experience when discussing the second-eye target. This is where specifics matter. “I need to read novels for 30 minutes” is different from “I mostly read phone texts and drive at night.” The lens plan should serve your actual life, not an imaginary brochure version of you wearing linen near a sailboat.
What to ask before the next surgery: near vision, distance vision, and daily reading goals
Before second-eye surgery, ask clear questions. What is the target for the second eye? Will the two eyes be matched for distance, or will there be some monovision? How might that affect reading? When should you expect temporary imbalance? What symptoms should trigger a call?
Bring your reading log. Bring your glasses. Bring the humble truth of your daily tasks. Eye care is better when it knows the difference between “I read occasionally” and “I edit legal documents on a laptop for 6 hours.”
- Tell your surgeon what felt hard after the first eye.
- Ask how the second-eye target may affect near and distance tasks.
- Discuss whether monovision is helping, tolerable, or frustrating.
Apply in 60 seconds: Write your top 3 vision priorities: reading, driving, screens, hobbies, or walking safely.
When to Seek Help: Red Flags, Not Reading Quirks
Call promptly for vision loss, severe pain, increasing redness, or swelling
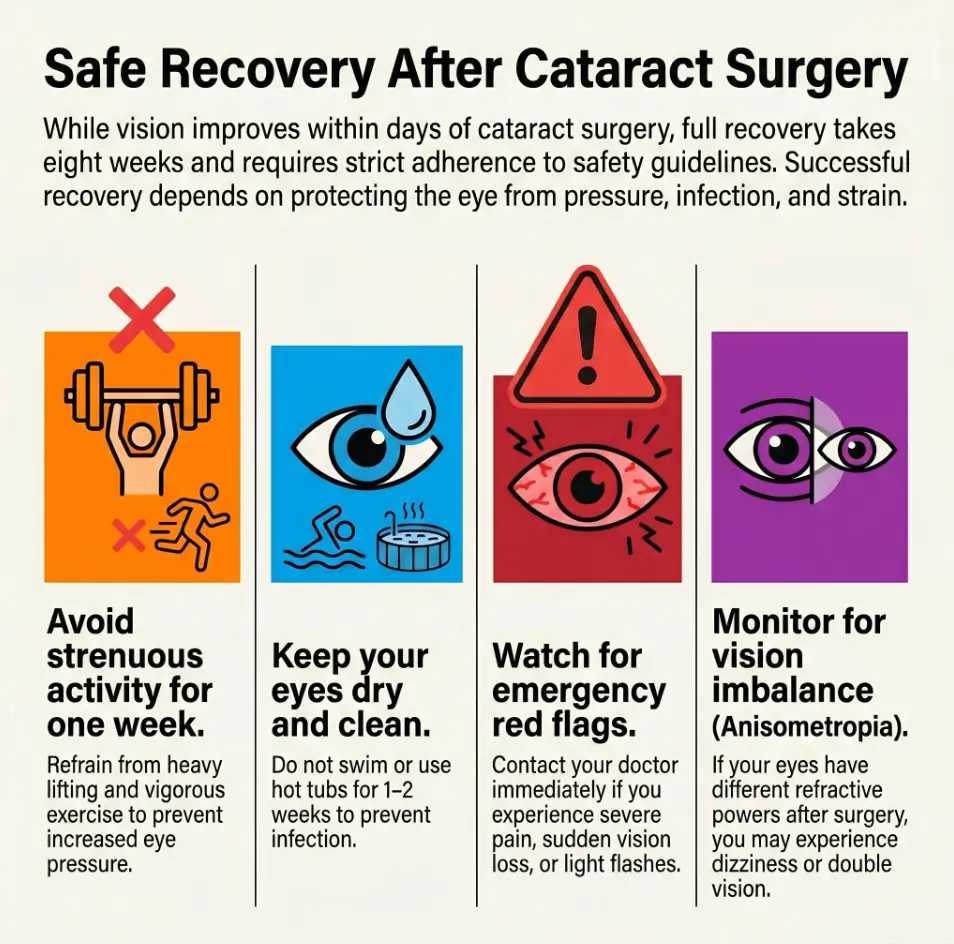
A little blur or mild scratchy sensation can occur during recovery, but sudden vision loss, severe pain, worsening redness, discharge, or eyelid swelling needs prompt professional guidance. Follow your surgeon’s post-op instructions, including emergency contact steps.
Do not wait for a routine appointment if the symptom feels abrupt, intense, or clearly worse. Eyes are small organs with no patience for calendar drama.
Ask urgently about flashes, many new floaters, or a curtain-like shadow
Flashes, many new floaters, or a curtain-like shadow can signal a retinal problem, including retinal tear or detachment. The American Academy of Ophthalmology lists flashing lights or a dark curtain after cataract surgery among symptoms that need urgent attention.
This is not meant to frighten you away from reading. It is meant to keep the category clear: reading fatigue is one thing; sudden retinal warning signs are another.
Report double vision, nausea, imbalance, or reading distortion that persists
Persistent double vision, nausea, imbalance, or distortion should be reported. These symptoms may come from anisometropia, aniseikonia, eye teaming issues, ocular surface problems, medication effects, or other causes that deserve evaluation.
If you feel unsafe walking, climbing stairs, or driving, treat that as important. Reading imbalance is not only a comfort issue when it spills into balance and mobility.
Keep the post-op visit even if the eye feels “mostly fine”
Post-op visits are not just ceremonial check-ins. They help your surgeon monitor healing, pressure, inflammation, IOL position, and visual progress. Even if your eye feels decent, keep the appointment unless your surgeon tells you otherwise.
Bring questions. Bring notes. Bring the glasses that betrayed you. Your future self will appreciate the small effort.
FAQ
Can anisometropia happen after cataract surgery?
Yes. Anisometropia can happen after cataract surgery when the two eyes have different focusing power. This is common between first-eye and second-eye surgery, and it can also happen when one eye is intentionally set for distance and the other for near vision.
Why does reading feel uneven after one cataract is removed?
Reading may feel uneven because one eye now has a clearer artificial lens while the other eye still has a cataract or a different prescription. Your brain must combine two different visual inputs. That can create strain, blur, dizziness, or the feeling that the page is not sitting still.
How long does reading imbalance last after cataract surgery?
It varies. Some people adapt within days. Others feel imbalance until the second eye is treated, the prescription stabilizes, or a better glasses or contact lens plan is made. Ask your surgeon what timeline fits your surgery, IOL target, and healing pattern.
Can new glasses fix anisometropia after cataract surgery?
New glasses can help some cases, especially once the eye has healed enough for a stable prescription. But if the prescription difference between the eyes is large, glasses may create magnification differences. Your optometrist or ophthalmologist can explain whether glasses, contacts, or another plan fits your case.
Are contact lenses better than glasses for post-cataract imbalance?
Sometimes. Contact lenses may reduce image-size mismatch because they sit directly on the eye. However, they are not right for everyone, and you should not use contacts after cataract surgery unless your eye-care team says it is safe.
Is monovision after cataract surgery supposed to feel strange?
It can feel strange at first. Monovision asks one eye to favor distance and the other to help with near vision. Many people adapt, but some experience depth perception changes, reading discomfort, or visual imbalance. Tell your surgeon how it feels in daily life, not just on the eye chart.
Why do my old glasses feel wrong after cataract surgery?
Your old glasses were made for your pre-surgery eyes. Once one cataract is removed and an IOL is placed, that eye may no longer need the same correction. Old glasses can overcorrect one eye, undercorrect the other, or create magnification differences that make reading feel worse.
When should I call my eye doctor about post-cataract vision imbalance?
Call promptly if you have sudden vision loss, severe pain, increasing redness, swelling, flashes, many new floaters, a curtain-like shadow, persistent double vision, or dizziness that affects safety. For milder reading strain, track symptoms and discuss them at your follow-up unless your instructions say otherwise.
Next Step: Bring a Two-Minute Reading Log to Your Eye Visit
Record what happens after 5, 10, and 20 minutes of reading
The best next step is humble and oddly powerful: keep a tiny reading log. Not a diary with candlelight and leather binding. Just a few notes that show what your eyes do over time.
Choose one familiar reading task. Use the same chair, light, and page if possible. Note what happens after 5 minutes, 10 minutes, and, only if comfortable, 20 minutes. Stop sooner if symptoms increase.
Note which eye feels blurred, strained, larger, smaller, or “off”
Write down which eye seems responsible, but stay flexible. Sometimes the eye that feels “bad” is not the only cause. The problem may be how both eyes work together.
Use practical words: blurred, smaller, larger, tilted, double, swimmy, dizzy, sharp but uncomfortable, okay with one eye covered, worse with old glasses. Those phrases give your eye-care team better material than “everything is weird,” although, frankly, that phrase has earned its place in the recovery vocabulary.
Bring your old glasses, readers, and current medication list
Bring every pair you actually use. Old progressives, readers, computer glasses, sunglasses, and the backup pair from the glove compartment all have evidence to offer. Also bring your drop schedule and medication list, especially if dry eye, dizziness, or other health factors are part of the story. A one-page medication list template can make that part less fussy and much easier to update.
Ask direct questions: Should I use readers temporarily? Should I avoid old glasses? When can my final prescription be checked? Could contact lenses help? Is this expected between surgeries? What symptoms should make me call urgently?
One concrete action: test one familiar page today under good light and write down what changes
Remember the opening problem, the page that would not behave? The goal was never to fight your eyes into submission. The goal is to reduce visual conflict, spot warning signs, and give your doctor enough detail to help.
In the next 15 minutes, choose one familiar page, set good light, enlarge the text if needed, read briefly, and write down what changes. That small note can turn a foggy complaint into a usable clinical clue.
- Track time, lighting, glasses, and symptoms.
- Use plain words your doctor can act on.
- Bring every pair of glasses or readers you actually use.
Apply in 60 seconds: Write this line now: “After 10 minutes of reading, I notice…”
Final thought: Anisometropia after cataract surgery can make reading feel strangely personal, as if the page itself has developed a mood. But the problem usually has practical pieces: prescription difference, image-size mismatch, healing time, lighting, reading distance, monovision adaptation, or second-eye timing. Start small. Track honestly. Call promptly for red flags. Let your eye-care team help your two eyes return to the same conversation.
Last reviewed: 2026-05.
Tags: cataract surgery recovery, anisometropia, reading imbalance, eye health, monovision
Meta description: Practical ways to cope with anisometropia after cataract surgery, reading imbalance, temporary fixes, and red flags.